Keywords
Biopsy, Large-Core Needle; Pancreatic Neoplasms; Ultrasonography
Abbreviations
CNB: Core needle biopsy LUS: Laparoscopic ultrasonography FNAB: Fine-needle aspiration biopsy
INTRODUCTION
Patients with pancreatic cancer have a dismal prognosis. Pancreatic cancer is the fourth leading cause of cancerrelated death [1]. The nonspecific nature of the early symptoms of pancreatic cancer may cause a delayed diagnosis. At initial presentation, only approximately 20% of patients are candidates for tumor resection.
Staging laparoscopy is applicable to locally advanced pancreatic cancer patients with no evidence of distant disease who are being considered for chemoradiotherapy. Staging laparoscopy may effectively identify occult stage IV disease that cannot be detected by imaging, and may prevent morbidity and unnecessary treatment costs. In addition, staging laparoscopy may improve adjuvant therapy protocols by allowing better selection of treatment method [2]. Laparoscopic ultrasonography (LUS) reportedly improved the accuracy of pancreatic cancer tumor staging [3-5].
The histological analysis of a pancreatic mass is beneficial before beginning antitumor treatment. Specifically, several authors have suggested that genetic and molecular analyses using laser micro dissection of pancreatic tumors contributed to the development of tailor-made treatments [6, 7]. Endoscopic ultrasound-guided fine-needle aspiration and biopsy (EUS-FNA) is thought to be a safe, accurate, and sensitive method to obtain tissue from a pancreatic lesion [8-10]. However, there is evidence that the degree of accuracy depends greatly on the experience of the endoscopist. Unfortunately, EUS-FNA is not always useful for the recognition of pancreatic tumor malignancy or the differentiation between pancreatic cancer and chronic pancreatitis [8, 11, 12]. On the other hand, core needle biopsy (CNB) provides sufficiently large tissue samples [13]. Laparoscopic surgical techniques and LUS have made it possible to perform needle biopsies for pancreatic tumors. However, there are few reports concerning the evaluation of LUS-guided CNB. This study aimed to assess the feasibility and role of LUS-guided CNB in determining the most effective treatment strategy for locally advanced unresectable pancreatic cancer.
MATERIALS AND METHODS
Two-hundred and sixty-five patients diagnosed with pancreatic cancer were admitted to our hospital between February 1, 2006 and December 31, 2011. Data from 60 consecutive patients who underwent staging laparoscopy were retrospectively analyzed. All patients were diagnosed with advanced, unresectable pancreatic tumors without obvious distant metastasis by multi-detector computed tomography (MD-CT) or magnetic resonance imaging (MRI) and positron emission tomography-computed tomography (PET-CT). The criteria for the diagnosis of a locally advanced, unresectable tumor were tumor invasion into the superior mesenteric artery, celiac artery, common hepatic artery, aorta, inferior vena cava, or bifurcation of the superior mesenteric vein. These patients were nominated for the candidate of chemotherapy or chemoradiotherapy.
Staging laparoscopy was required to identify small metastatic lesions for the determination of a suitable therapeutic strategy; namely, systemic chemotherapy or chemo radiotherapy. A standard approach for laparoscopic surgery was performed through three to four ports using a multi-incision technique. LUS-guided CNB was performed to obtain tissue samples for a pathological diagnosis. LUS was performed with an LUS probe (Linear Probe UST- 5550; ALOKA, Tokyo, Japan) connected to a high-end ultrasonographic scanner (ProSound SSD-5500; ALOKA, Tokyo, Japan) through a 12-mm trocar under laparoscopic imaging. Inspection of the whole liver, including the deep parenchyma, was performed to detect small nodules.
LUS-guided CNB was performed using an 18-gauge needle that was introduced through the right anterior abdominal wall above the pancreatic tumor (Figure 1). Tumors with cystic components were excluded to avoid the risk of peritoneal dissemination resulting from needle puncture. Before the CNB, we dissected a part of the omentum and opened the omental bursa using two laparoscopic dissectors through 5-mm working ports to observe the distal pancreas and directly puncture the tumors. All punctures were performed several times under LUS from a laparoscopic view. Ultrasonographic procedures consisted of the following three steps: (1) measurement of tumor location and size, (2) a search for critical vessels around the tumor using Doppler mode, and (3) a confirmation of safe puncture sites in the tumor (Figure 2). If critical vessels crossed the puncture line, we aborted the biopsy and later switched to EUS-FNA. The obtained tissue samples were used for frozen sections and the final pathological diagnosis (Figure 3). Immediate LUS-guided CNB-related complications were recorded during the procedure, and patients were monitored for late complications (>24 h postoperatively) before discharge. Umbilical open wounds were sutured with absorbable sutures.
Figure 1. Image of Laparoscopic ultrasonography (LUS)-guided core
needle biopsy (CNB).
Figure 2. Laparoscopic ultrasonographic images during the puncture of
the pancreatic tumor. (a) The dotted line indicates the pre-puncture path
through the tumor. (b) The identification of critical vessels using color
Doppler imaging around the tumor. (c) The white arrow indicates the
needle puncturing the tumor.
Figure 3. Pathological images of a core needle biopsy (CNB) sample of
pancreatic adenocarcinoma with hematoxylin-eosin staining. a. A stick
of tissue was collected using a Tru-Cut needle. b. Not only the cancer
nest, but also the neighboring connective tissue was gathered without
destruction of the tissue structure.
As six patients were found peritoneal dissemination during the examination, we acquired the tissue from disseminated lesion and did not perform tumor puncture. Two patients who were performed EUS-FNA at another hospital before admissions were excluded. As LUS-guided CNB was aborted in four patients to avoid critical vessel injury, a total of 25 patients underwent CNB. Another 23 patients successively underwent EUS-FNA alone for a pathological diagnosis in the division of endoscopy at our hospital before staging laparoscopy. As twelve patients received neither LUSguided CNB nor EUS-FNA in our hospital, 48 patients were enrolled during the study period finally. Informed consent was obtained from all patients. As these patients were not divided into the two groups prospectively, this study is not a randomized control study.
The outcomes of operating time, bleeding volume, histological diagnosis status, incidence of postoperative complications, and incidence of peritoneal dissemination following the examination were evaluated between the two groups. All patients started the anticancer treatment after the examination, and were followed up at the out-patient center of our hospital. Radiographic diagnostic imaging by enhanced CT or MRI was performed to all patients every three months for detecting recurrence. Clinical stage was determined according to the General Rules for the Study of Pancreatic Cancer by the Japan Pancreatic Society (sixth edition).
ETHICS AND STATISTICS
This study was approved by the institutional review board of Kagoshima University Hospital and conformed to the provisions of the World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects.
All data are presented as the number of patients or means, and were compared by a Mann–Whitney U-test. Characteristic factors in the two groups were compared using chi-squared tests. A p-value <0.05 indicated statistical significance. All statistical analyses were performed using StatView for Windows Version 5.0 (SAS Institute, North Carolina, USA).
RESULTS
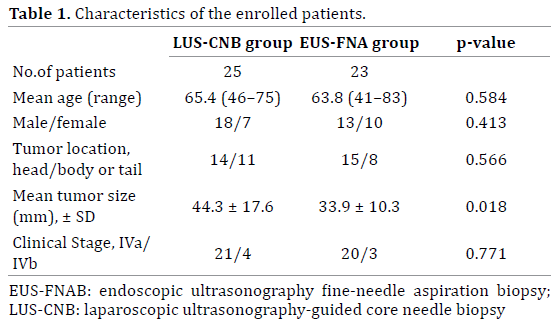
A comparison of the characteristic results between the LUS-guided CNB group and the non-LUS-guided CNB group is shown in Table 1. There was no significant difference in age, sex, distribution of tumor location, or clinical stage proportion. The mean tumor size in the LUS-guided CNB group was significantly larger than that in the non-LUSguided CNB group (p < 0.05).
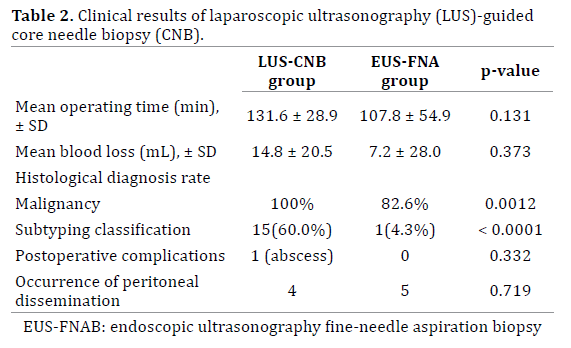
A comparison of the clinical results between the two groups is shown in Table 2. The operation time was longer in the LUS-guided CNB group, although the difference was not statistically significant. A small volume of bleeding was recorded in both groups without a significant difference. The rates of malignancy diagnosis and histological classification subtyping were significantly higher in the LUS-guided CNB group. Although one patient in the LUSguided CNB group had an abdominal abscess resulting from a pancreatic fistula at the puncture site, it resolved after conservative treatment within 2 weeks. Median time of following up period for all patients was 12.7 months. Peritoneal dissemination occurred in five patients with no peritoneal lesion at the time of laparoscopy. There was no significant difference in the occurrence of peritoneal dissemination after laparoscopic examination between the two groups.
Details of the LUS-guided CNB pathological results are shown in Figure 4. One patient with suspected carcinoma diagnosed by EUS-FNA at another hospital was diagnosed with chronic pancreatitis by LUSguided CNB. Immunohistochemical staining using DF3 (MUC1) antibody for the tissue sample obtained by LUSguided CNB revealed moderately differentiated tubular adenocarcinoma, although EUS-FNA failed to prove malignancy. On the other hand, EUS-FNA succeeded in providing pathological differentiation in only one patient. It was difficult to diagnose malignancy in four patients because of insufficient tissue volumes.
Figure 4. The pathological diagnosis results of each sample acquired by
LUS-guided CNB or EUS-FNA.
DISCUSSION
Patients with disease initially deemed to be unresectable pancreatic cancer on the basis of imaging studies should undergo biopsy to obtain a histological diagnosis if chemotherapy or chemoradiotherapy is planned. Tissue for histological analysis can be obtained percutaneously or laparoscopically by various biopsy techniques such as fineneedle aspiration biopsy (FNAB) under ultrasonography, EUS, or CT guidance [14-16]. However, a limitation of FNAB is that the tissue volume obtained may be too small for an accurate diagnosis [14]. CNB under laparotomy is a more accurate method to obtain enough tissue for a histological diagnosis. Few articles have compared the advantages and shortcomings of LUS-guided CNB with those of EUS-FNA. Therefore, we compared the clinical difference between these two approaches for the histological diagnosis of unresectable pancreatic cancer. The direct CNB technique under LUS imaging has made it possible to safely obtain sufficient tissue for certain pathological diagnoses, including the cancer differentiation of a pancreatic mass.
To determine a treatment strategy for locally unresectable pancreatic cancer, a laparoscopic approach is desirable for tumor staging [17, 18]. Even the most advanced CT scan is inadequate for the accurate staging of locally extended pancreatic cancer because occult distant disease will be found with high frequency by laparoscopic inspection [19]. Therefore, we employed staging laparoscopy to precisely identify small metastases and select the appropriate treatment [20]. A number of studies have evaluated the additive benefit of LUS at the time of laparoscopic staging [21]. In our experience, staging laparoscopy revealed metastatic lesions in 33% of advanced pancreatic cancer patients with no obvious metastasis by preoperative imaging (data not shown). We performed a detailed LUS inspection of every patient, and LUS-guided CNB has been introduced since staging laparoscopy began.
Strasburg et al. reported that direct LUS-guided CNB provides a rapid and safe diagnosis of pancreatic lesions [22]. Although LUS-guided CNB has been introduced as a less invasive procedure than laparotomy, FNAB has been recently performed under the guidance of EUS without general anesthesia or surgical stress. Kilment et al. reported that EUS-FNA provides an accurate diagnosis in 92% of cases and has a positive therapeutic impact in two-thirds of patients with solid pancreatic masses [8]. It has been reported that the diagnostic sufficiency, technical performance, and safely profiles of 22-gauge aspiration and 22-gauge biopsy needles for EUS-guided sampling are comparable [23]. However, CNB yielded a significantly higher sensitivity than FNA in several organs, including the pancreas [24]. Despite the use of EUS-FNA, up to 7% of pancreatic cancer patients who underwent resection had benign disease in a postoperative pathologic examination [11]. Gleeson et al. reported that the false-positive rate was 5.3% and increased to 7.2% when false-suspicious cases were included [25]. Butturini et al. showed that the laparoscopic biopsy of advanced unresectable pancreatic cancer was a feasible, safe, and reliable procedure to obtain a cytohistological diagnosis whenever ultrasonographyguided FNA fails [26]. The combination of FNA and CNB sampling techniques increases diagnostic sensitivity and occasionally provides more accurate classifications of tumors and benign lesions in the diagnosis of radiologically detected abdominal lesions [27]. These studies discussed that CNB had an advantage in the preservation of the tissue architecture of the specimen, which may be important in the assessment and subtyping of some tumors, and retained the possibility of performing immunohistochemical techniques [24].
A large-scale analysis of gene expression has been widely proposed as a powerful method for the diagnosis and identification of predictive factors for the treatment of various malignant tumors [28-31]. The availability of tumor tissue is critical for an accurate assessment of gene expression, and laser microdissection and primary cell cultures may be useful tools to separate tumor cells from stromal reactions [6]. Ashida et al. reported an analysis of mRNA related to gemcitabine sensitivity using a high-fidelity RNA amplification technique that allowed analysis of gene expression profiles from EUSFNA samples of unresectable pancreatic cancer [28]. However, contamination of normal tissue with tumor tissue obtained by the EUS-FNA procedure may be a major obstacle to an accurate analysis. If we need to know only confirmation of the tumor malignancy, EUS-FNA may be enough for the diagnosis. But the sufficiently large amount of tissue obtained by CNB may help allow determination of differences in the genetic characteristics of tumor and normal tissue using advanced tissue extraction techniques such as laser microdissection. The tissue samples obtained from an 18-gauge needle had not only cancer tissue, but also environmental connective tissue in this series. Although multidisciplinary approaches such as chemotherapy and chemoradiotherapy are applicable for treatment of locally advanced unresectable pancreatic cancer, it is still controversial that which is better for the initial therapy [32, 33]. This technique may contribute to genetic analyses that will help determine the best treatment options, such as the selection of an antitumor reagent, and evaluations of the radiosensitivity of pancreatic cancer in the future. It is also important that we need to set the criterion for selection of the patients who receive the profit of this technique in control of cancer.
Because CNB requires a larger cutting needle than FNAB, a higher risk of complications such as bleeding can be hypothesized. In our study, although there was no bleeding complication, we observed one case of a pancreatic fistula as a postoperative complication. This complication was believed to have been caused by the use of a 16-gauge needle when this procedure was performed in the early stage. Thereafter, we had no complications with the use of an 18-gauge needle. It is also a concern that needle puncture may cause dissemination. Micames et al. reported that peritoneal carcinomatosis may occur more frequently in patients who undergo percutaneous FNA than in those who undergo EUS-FNA for the diagnosis of pancreatic cancer [16]. The occurrence rate of peritoneal dissemination was equivalent in both groups in this series. As the number of cases was not large enough, we limited performing CNB to unresectable cases. It is necessary to verify the long-term results of the risk of dissemination in a larger number of cases.
The major limitation of this study was the small number of the patients and the lack of randomization in patient selection. In this study, there were no significantly different characteristics between the LUS-guided CNB group and the EUS-FNA group, except for mean tumor size. As CNB required a tumor thickness >2 cm to avoid dorsal tissue injury, smaller sized tumors were included in the EUS-FNA group. Moreover, it was difficult to perform a percutaneous puncture of a tumor located in the uncus of the pancreas head because of the presence of the superior mesenteric vein on the ventral side of the tumor. The significance of LUS-guided CNB for pancreatic cancer should be evaluated through a prospective study in a larger number of cases.
CONCLUSION
In conclusion, LUS-guided CNB is a technically feasible and safe procedure that can be easily applied following staging laparoscopy for pancreatic cancer. The sufficient amount of tissue obtained by this technique makes it possible to achieve high diagnostic accuracy. The clinical impact may be conveyed in terms of the determination of treatment strategies for advanced pancreatic cancer by tissue extraction using the LUS-guided CNB technique.
Conflict of Interest
There are no conflicts of interest to declare.
References
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin 2010; 60:277-300. [PMID: 20610543]
- Stefanidis D, Grove KD, Schwesinger WH, Thomas CR Jr. The current role of staging laparoscopy for adenocarcinoma of the pancreas: a review. Ann Oncol 2005; 17:189-99.[ PMID: 16236756]
- John TG, Wright A, Allan PL, Redhead DN, Paterson-Brown S, Carter DC et al. Laparoscopy with laparoscopic ultrasonography in the TNM staging of pancreatic carcinoma. World J Surg 1999; 23:870-81.[ PMID: 10449813]
- John TG, Greig JD, Carter DC, Garden OJ. Carcinoma of the pancreatic head and periampullary region. Tumor staging with laparoscopy and laparoscopic ultrasonography. Ann Surg 1995; 221:156-64.[ PMID: 7857143]
- Thomson BN, Parks RW, Redhead DN, Welsh FK, Madhavan KK, Wigmore SJ et al. Refining the role of laparoscopy and laparoscopic ultrasound in the staging of presumed pancreatic head and ampullarytumours. Br J Cancer 2006; 94:213-17.[ PMID: 16434983]
- Funel N, Giovannetti E, Del Chiaro M, Mey V, Pollina LE, Nannizzi S et al. Laser microdissection and primary cell cultures improve pharmacogenetic analysis in pancreatic adenocarcinoma. Lab Invest 2008; 88:773-84.[ PMID: 18490900]
- Giovannetti E, Funel N, Peters GJ, Del Chiaro M, Erozenci LA, Vasile E et al. MicroRNA-21 in pancreatic cancer: correlation with clinical outcome and pharmacologic aspects underlying its role in the modulation of gemcitabine activity. Cancer Res 2010; 70:4528-38.[ PMID: 20460539]
- Kliment M, Urban O, Cegan M, Fojtik P, Falt P, Dvorackova J et al. Endoscopic ultrasound-guided fine needle aspiration of pancreatic masses: the utility and impact on management of patients. Scand J Gastroenterol 2010; 45:1372-79.[ PMID: 20626304]
- Goldin SB, Bradner MW, Zervos EE, Rosemurgy AS 2nd. Assessment of pancreatic neoplasms: review of biopsy techniques. J GastrointestSurg 2007; 11:783-90.[ PMID: 17562121]
- Jani N, Dewitt J, Eloubeidi M, Varadarajulu S, Appalaneni V, Hoffman B et al. Endoscopic ultrasound-guided fine-needle aspiration for diagnosis of solid pseudopapillary tumors of the pancreas: a multicenter experience. Endoscopy 2008; 40:200-3.[ PMID: 18067066]
- de la Fuente SG, Ceppa EP, Reddy SK, Clary BM, Tyler DS, Pappas TN. Incidence of benign disease in patients that underwent resection for presumed pancreatic cancer diagnosed by endoscopic ultrasonography (EUS) and fine-needle aspiration (FNA). J GastrointestSurg 2010; 14:1139-42.[ PMID: 20424928]
- Detlefsen S, Mohr Drewes A, Vyberg M, Klöppel G. Diagnosis of autoimmune pancreatitis by core needle biopsy: application of six microscopic criteria. Virchows Arch 2009; 454:531-9.[ PMID: 19238431]
- Paulsen SD, Nghiem HV, Negussie E, Higgins EJ, Caoili EM, Francis IR. Evaluation of imaging-guided core biopsy of pancreatic masses. AJR Am J Roentgenol 2006: 187:769-72.[ PMID: 16928943]
- Kim TH, Choi KH, Song HS, Kim JW, Jeon BJ. Histology combined with cytology by endoscopic ultrasound-guided fine needle aspiration for the diagnosis of solid pancreatic mass and intra-abdominal lymphadenopathy. Gut Liver. 2013;7:605-10.[ PMID: 24073320]
- Xu K, Zhou L, Liang B, Niu L, Zheng X, Xu J et al. Safety and accuracy of percutaneous core needle biopsy in examining pancreatic neoplasms. Pancreas. 2012 ;41:649-51. [ PMID: 22504382]
- Micames C, Jowell PS, White R, Paulson E, Nelson R, Morse M et al. Lower frequency of peritoneal carcinomatosis in patients with pancreatic cancer diagnosed by EUS-guided FNA vs. percutaneous FNA. GastrointestEndosc. 2003 ;58:690-5.[ PMID: 14595302]
- Shoup M, Winston C, Brennan MF, Bassman D, Conlon KC. Is there a role for staging laparoscopy in patients with locally advanced, unresectable pancreatic adenocarcinoma? J GastrointestSurg 2004; 8:1068-71.[ PMID: 15585395]
- Morak MJ, Hermans JJ, Smeenk HG, Renders WM, Nuyttens JJ, Kazemier G et al. Staging for locally advanced pancreatic cancer. Eur J SurgOncol 2009; 35:963-8.
- Liu RC, Traverso LW. Diagnostic laparoscopy improves staging of pancreatic cancer deemed locally unresectable by computed tomography. SurgEndosc 2005; 19:638-42.[ PMID: 15776215]
- Maemura K, Shinchi H, Mataki Y, Kurahara H, Hayashi T, Kuwahata T et al. Advanced staging laparoscopy using single-incision approach for unresectable pancreatic cancer. SurgLaparoscEndoscPercutan Tech. 2011;21:e301-5. [PMID: 22146176]
- Jakimowicz JJ. Intraoperative ultrasonography in open and laparoscopic abdominal surgery: an overview. SurgEndosc 2006; 20:S425-35. [PMID: 16544064]
- Strasberg SM, Middleton WD, Teefey SA, McNevin MS, Drebin JA. Management of diagnostic dilemmas of the pancreas by ultrasonographically guided laparoscopic biopsy. Surgery 1999; 126:736- 41; discussion 741-3.[ PMID: 10520923]
- Bang JY, Hebert-Magee S, Trevino J, Ramesh J, Varadarajulu S. Randomized trial comparing the 22-gauge aspiration and 22-gauge biopsy needles for EUS-guided sampling of solid pancreatic mass lesions. GastrointestEndosc. 2012;76:321-7.[PubMed PMID:22658389]
- Schoellnast H, Komatz G, Bisail H, Talakic E, Fauster M, Ehammer T et al. CT-guided biopsy of lesions of the lung, liver, pancreas or of enlarged lymph nodes: value of additional fine needle aspiration (FNA) to core needle biopsy (CNB) in an offsite pathologist setting. 2010;17:1275-81. [PMID: 20621527]
- Gleeson FC, Kipp BR, Caudill JL, Clain JE, Clayton AC, Halling KC et al. False positive endoscopic ultrasound fine needle aspiration cytology: incidence and risk factors. Gut 2010; 59:586-93.[ PMID: 20427392]
- Butturini G, Crippa S, Bassi C, Salvia R, Piccoli M, Pederzoli P. The role of laparoscopy in advanced pancreatic cancer diagnosis. Dig Surg 2007; 24:33-7.[ PMID: 17369679]
- Stewart CJ, Coldewey J, Stewart IS. Comparison of fine needle aspiration cytology and needle core biopsy in the diagnosis of radiologically detected abdominal lesions. J ClinPathol. 2002 ;55:93-7. [PMID: 11865001]
- Ashida R, Nakata B, Shigekawa M, Mizuno N, Sawaki A, Hirakawa K et al. Gemcitabine sensitivity-related mRNA expression in endoscopic ultrasound-guided fine-needle aspiration biopsy of unresectable pancreatic cancer. J ExpClin Cancer Res 2009; 28:83 DOI: 10.1186/1756- 9966-28-83.[ PMID: 19531250]
- Laurell H, Bouisson M, Berthelemy P, Rochaix P, Dejean S, Besse P et al. Identification of biomarkers of human pancreatic adenocarcinomas by expression profiling and validation with gene expression analysis in endoscopic ultrasound-guided fine needle aspiration samples. World J Gastroenterol 2006; 12:3344-51.[ PMID: 16733850]
- Leung TH, Ngan HY. Interaction of TAp73 and breast cancerassociated gene 3 enhances the sensitivity of cervical cancer cells in response to irradiation-induced apoptosis. Cancer Res 2010; 70:6486-96. [ PMID: 20647320]
- Yu G, Zhu MH, Zhu Z, Ni CR, Zheng JM, Li FM. Expression of ATM protein and its relationship with p53 in pancreatic carcinoma with tissue array. Pancreas 2004; 28:421-6.[ PMID: 15097860]
- Huguet F, Mukherjee S, Javle M. Locally advanced pancreatic cancer: the role of definitive chemoradiotherapy. ClinOncol (R CollRadiol). 2014; 26:560-68. [PMID:25001636]
- He J, Page AJ, Weiss M, Wolfgang CL, Herman JM, Pawlik TM. Management of borderline and locally advanced pancreatic cancer: where do we stand? World J Gastroenterol. 2014 ;20:2255-66. [PMID: 24605025]





