Keywords
Antibodies; Azathioprine; Crohn Disease; Inflammatory Bowel Diseases; Pancreas; Pancreatitis; Serology
Abbreviations
IBD: inflammatory bowel disease; PAB: pancreatic autoantibodies
INTRODUCTION
Crohn’s disease is a chronic inflammatory disease involving the entire gastrointestinal tract. The etiology is thought to consist of an inappropriate immune response to commensal bacteria in the gut and a failure to downregulate this inflammatory response. Genetic and environmental factors play an important role in the pathogenesis. It is a chronic disorder characterized by periods of quiescence and periods of active disease [1]. Azathioprine is a purine analogue which is frequently used as maintenance therapy for Crohn’s disease. However, the occurrence of side effects is a major drawback in the use of azathioprine. In up to 23% of patients with IBD, azathioprine is withdrawn due to these side effects. It is increasingly more apparent that side effects occur more often in IBD than in other autoimmune diseases [2, 3]. One of the most severe side effects is the occurrence of acute pancreatitis which is seen in approximately 5% of patients with Crohn’s disease and very rarely in patients treated with azathioprine for other diseases [2].
Polymorphisms in the gene encoding for thiopurinemethyltransferase (TPMT), which metabolizes azathioprine to 6-mercaptopurine and 6-methyl-mercaptopurine, have been associated with the development of dosedependent side effects such s myelosuppression but not with azathioprine-induced pancreatitis [4]. A possible mechanism for the occurrence of side effects in azathioprine therapy might be explained by inosine triphosphate pyrophospatase (ITP-ase) deficiency. In one study, flu-like symptoms, rash and acute pancreatitis were associated with a missense mutation in the gene encoding for inosine triphosphate pyrophospatase [5]. However subsequent studies failed to confirm this association [6, 7]. Consequently, azathioprine-induced pancreatitis is a very severe side effect but the pathogenetic mechanism is unknown.
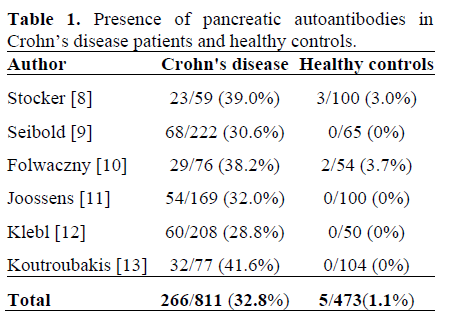
Circulating pancreatic autoantibodies (PABs) are found in approximately 30% of patients with Crohn’s disease (Table 1) [8, 9, 10, 11, 12, 13]. PABs are not found in healthy controls, in patients with other gastrointestinal diseases or in various autoimmune disorders (including autoimmune hepatitis, systemic lupus erythematosis and rheumatoid arthritis). Since PABs and azathioprine-induced pancreatitis are both specific for Crohn’s disease, an association or a pathogenic role of PABs in azathioprine-induced pancreatitis could be expected. One pathogenic mechanism could be that azathioprine aggravates the inflammation in an already inflamed pancreas in Crohn’s disease in PAB-positive patients. We evaluated the prevalence of PABs in patients with azathioprine-induced pancreatitis in Crohn’s disease and in controls with Crohn’s disease, hypothesizing that most or all patients with azathioprine-induced pancreatitis have circulating PABs.
MATERIALS AND METHODS
Patients
Patients were available from the IBD-cohort of the University Medical Center of Groningen [14]. Patients fulfilling the diagnostic criteria for Crohn’s disease were eligible for the study. These criteria are based on accepted clinical, endoscopic, radiological and histological findings [1]. The diagnosis of azathioprine-induced acute pancreatitis was made by the attending physician according to the following criteria: upper abdominal or radiating pain with or without nausea and vomiting with at least a three-fold rise in serum amylase in combination with the disappearance of these symptoms after the withdrawal of azathioprine. All patients had an upper abdominal ultrasonography to exclude biliary pancreatitis. Patients with suspected alcohol-induced pancreatitis were excluded. Ten patients with azathioprineinduced pancreatitis were selected.
Based on the assumption that azathioprineinduced pancreatitis was associated with the presence of PABs, one could hypothesize that a control group of Crohn’s disease patients using azathioprine but without pancreatitis would have a lower than expected prevalence of PABs. Therefore, the controls consisted of 31 randomly selected patients with Crohn’s disease but not using azathioprine.
Serum Samples
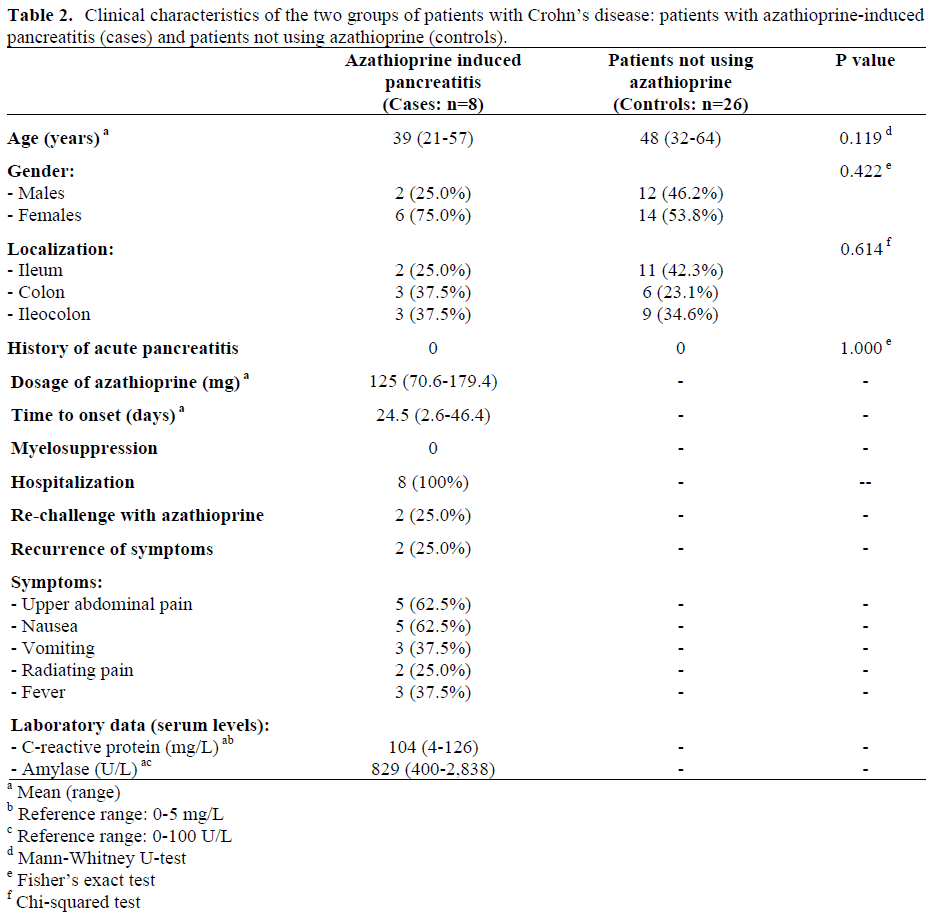
Serum samples were drawn from patients enrolled in the study as outpatients at the Department of Gastroenterology and Hepatology of the University Medical Centre of Groningen, the Netherlands and were stored at -80°C until analysis. Serum samples were obtained from 10 patients with azathioprine-induced pancreatitis (case group) and 31 patients with Crohn’s disease not using azathioprine (control group). Two out of the 10 case samples (20.0%) as well as 5 out of the 31 control samples (16.1%) could not be evaluated due to the poor quality of the sera. Therefore, the sample of patients evaluated in the study included 8 cases with azathioprine-induced pancreatitis and 26 controls with Crohn’s disease not using azathioprine. Serum samples were obtained before the development of azathioprineinduced pancreatitis in two patients and subsequently in the other six patients with azathioprine-induced pancreatitis. The characteristics of the patients included with a successful PAB determination are shown in Table 2.
Pancreatic Autoantibodies
Autoantibodies to the exocrine pancreas were determined on frozen sections of human blood group 0 Rh- pancreata using an indirect immune fluorescence technique. The slides were incubated for 30 minutes with both an undiluted and a 1:10 diluted sample of the patient’s serum. Binding of pancreatic autoantibodies was detected using fluorescein isothiocyanate (FITC)-labelled polyclonal rabbit anti-human IgG antibodies (F0202, Dakocytomation, Glostrup, Denmark). The slides were read under a fluorescence microscope (Leica DMRBE, Bensheim, Germany) by two independent observers. Serum samples showing either staining of the lumen of the acini (extracellular) or the cytoplasm of the exocrine cells (intracellular) were considered to be positive. There was 100% agreement for negative and positive samples between the two independent reviewers. Positive sera were diluted for semiquantitative interpretation of the results.[11, 12, 13, 15, 16].
ETHICS
Written informed consent was obtained from all participating subjects. The study protocol conforms to the ethical guidelines of the "World Medical Association Declaration of Helsinki”, as reflected in a priori approval by the Medical Ethical Committee of the University Medical Center Groningen, the Netherlands.
STATISTICS
The sample size calculation, as well as the post-hoc evaluation of the power, were performed by using the PS Power and Sample Size Calculations Program Version 2.1.30 provided by the Department of Biostatistics of Vanderbilt University (https://www.mc.vanderbilt.edu/ prevmed/ps/index.htm) [17]. The sample size calculation was made taking into account the assumption of a 0.85 prevalence of PABs in the Crohn’s disease patients with azathioprine-induced pancreatitis and a 0.328 value in the control Crohn’s disease group (Table 1). With a power of 0.80, a two-tailed significant level of 0.05 and a ratio of control to case patients equal to 3, a sample size of 10 patients with azathioprine-induced pancreatitis (together with 30 controls) was required. The Fisher’s exact, the chi-squared, and the Mann-Whitney U tests were applied by using the SPSS 14.0.2 statistical package (SPPS Inc., Chicago, IL, USA). Mean, range and frequencies were used as descriptive statistics.
RESULTS
Only two out of the eight patients with azathioprine-induced pancreatitis were positive for circulating PABs (25.0%); the titers were high being 1:40 and 1:160, respectively. These two samples were taken before the development of azathioprineinduced pancreatitis. None of the 6 samples which were obtained after the development of azathioprine-induced pancreatitis were PABpositive. From the 26 serum samples of the controls, only two (7.7%) were positive for circulating PABs, both in low titers of 1:2. All positive samples had an extracellular fluorescence pattern. The prevalence of PABs in the two groups was not statistically significant having a P value of 0.229.
DISCUSSION
Since circulating PABs and azathioprineinduced pancreatitis are both specific for Crohn’s disease, we hypothesized that the occurrence of PABs might be a risk factor for azathioprine-induced pancreatitis in Crohn’s disease patients. We evaluated the occurrence of PABs in selected patients with azathioprine- induced pancreatitis and compared this with a control group of patients with Crohn’s disease not using azathioprine.
Samples from 8 patients with azathioprineinduced pancreatitis were obtained and 25% of the patients with azathioprine-induced pancreatitis had circulating PABs versus 8% of the controls with Crohn’s disease. Although there was a difference, this was not statistically significant. Moreover, there were no significant differences in clinical or demographic variables between PAB-positive and PAB-negative patients (data not shown). PAB titers in the controls were very low whereas PABs were detectable in high concentrations in the patients with pancreatitis. This may indicate that the presence of PABs at high titers increases the risk of developing pancreatitis but is not a determining factor .
One study suggests that patients with Crohn’s disease and pancreatic exocrine insufficiency were significantly more likely to be PAB positive than patients with Crohn’s disease without pancreatic insufficiency [18]. The reason why Crohn’s disease patients have pancreatic insufficiency is unknown, but it might be due to a low-grade inflammation of the pancreas, possibly as an extraintestinal manifestation of Crohn’s disease. Furthermore, the use of azathioprine worsens the inflammation of the pancreas which has been shown in an animal model of acute pancreatitis in rats [19]. By extrapolating these findings, one could suggest that adding azathioprine to an already inflamed pancreas in PAB positive Crohn’s disease patients aggravates the inflammation and leads to a clinical overt picture of acute pancreatitis.
Interestingly, we could not confirm the previously described prevalence of PABs in approximately 30% of the patients with Crohn’s disease (Table 2) [8, 9, 10, 11, 12, 13]. In our population a total of 11.8% (4 out of 34) of the patients were positive for PABs. Although our sample size was small, the difference with each individual previous study is noticeable. Since PABs have not been shown to be associated with either disease severity or the use of medication and are stable in time, this difference is probably not caused by a selection bias. Furthermore, the antibodies were determined by a laboratory with extensive experience in immunofluorescent autoantibody testing, especially in the determination of islet cell antibodies for the purpose of type-1 diabetes diagnostics [15, 16]. The technique applied did not differ from what has been described in previous studies in Crohn’s disease [11, 12, 13], thus indicating that the prevalence of PABs varies between Crohn’s disease patient groups.
In recent years, many circulating antibodies have been identified in patients with inflammatory bowel disease. These antibodies have mainly been evaluated for the purpose of classification and the prediction of disease behavior [20]. The two most specific serological tests for ulcerative colitis and Crohn’s disease are perinuclear antineutrophil cytoplasmic antibodies (pANCA) and antibodies against Saccharomyces cerevisiae (ASCA), respectively [21]. In addition to PABs, pANCA and ASCA, various antibodies have been described including antibodies against outer-membrane porine C (OmpC) from Escherichia coli and, recently, serum reactivity to CBir1 flagellin has been identified in a subset of patients with complicated Crohn’s disease [22, 23]. Whether these antibodies are of pathogenic relevance and directly cause tissue inflammation or are merely an epiphenomenon is a matter of debate.
A major limitation of this study was the poor quality of the sera. In fact, about one-fifth of the samples could not be used for PAB determination (2 patients with azathioprineinduced pancreatitis and 5 controls). We reevaluated the statistical power by using the observed frequencies and the numbers of patients in our groups and this post-hoc analysis yielded a very low power of 0.155. Therefore, this study was underpowered for finding an association of PABs with azathioprine-induced pancreatitis; however neither can we disprove our hypothesis. Larger, preferably prospective, studies must be performed to clarify this. Moreover, due to the low prevalence of azathioprine-induced pancreatitis, this should be done in multiple centers.
CONCLUSIONS
We studied the occurrence of PABs in patients with Crohn’s disease and azathioprine-induced pancreatitis and in controls with Crohn’s disease not using azathioprine. Although the numbers were small, this study does not support an association between PABs and azathioprineinduced pancreatitis in Crohn’s disease. However, due to the lack of power detected in the post-hoc analysis and the high titers of PABs found in patients with azathioprineinduced pancreatitis when compared to controls, neither can we rule out this association. Additional larger studies are needed to clarify the pathogenetic mechanisms of azathioprine-induced pancreatitis in order to eventually enable clinicians to identify patients at risk.
Conflict of interest
The authors have no potential conflicts of interest
Acknowledgements
We appreciate the assistance of the technicians from the Reinier de Graaf Group, Department of Medical Immunology for their assistance in the pancreatic antibody determination.
References
- Podolsky DK. Inflammatory bowel disease. N Engl J Med 2002; 347:417-29. [PMID 12167685]
- Weersma RK, Peters FT, Oostenbrug LE, van den Berg AP, van Haastert M, Ploeg RJ, et al. Increased incidence of azathioprine-induced pancreatitis in Crohn's disease compared with other diseases. Aliment Pharmacol Ther 2004; 20:843-50. [PMID 15479355]
- Bajaj JS, Saeian K, Varma RR, Franco J, Knox JF, Podoll J, et al. Increased rates of early adverse reaction to azathioprine in patients with Crohn's disease compared to autoimmune hepatitis: a tertiary referral center experience. Am J Gastroenterol 2005; 100:1121- 5. [PMID 15842588]
- Krynetski EY, Tai HL, Yates CR, Fessing MY, Loennechen T, Schuetz JD, et al. Genetic polymorphism of thiopurine S-methyltransferase: clinical importance and molecular mechanisms. Pharmacogenetics 1996; 6:279-90. [PMID 8873214]
- Marinaki AM, Ansari A, Duley JA, Arenas M, Sumi S, Lewis CM, et al. Adverse drug reactions to azathioprine therapy are associated with polymorphism in the gene encoding inosine triphosphate pyrophosphatase (ITPase). Pharmacogenetics 2004; 14:181-7. [PMID 15167706]
- Gearry RB, Roberts RL, Barclay ML, Kennedy MA. Lack of association between the ITPA 94C>A polymorphism and adverse effects from azathioprine. Pharmacogenetics 2004; 14:779-81. [PMID 15564886]
- Allorge D, Hamdan R, Broly F, Libersa C, Colombel JF. ITPA genotyping test does not improve detection of Crohn's disease patients at risk of azathioprine/6-mercaptopurine induced myelosuppression. Gut 2005; 54:565. [PMID 15753546]
- Stöcker W, Otte M, Ulrich S, Normann D, Stöcker K, Jantschek G. Autoantibodies against the exocrine pancreas and against intestinal goblet cells in the diagnosis of Crohn's disease and ulcerative colitis. Dtsch Med Wochenschr 1984; 109:1963-9. [PMID 6150841]
- Seibold F, Weber P, Jenss H, Wiedmann KH. Antibodies to a trypsin sensitive pancreatic antigen in chronic inflammatory bowel disease: specific markers for a subgroup of patients with Crohn's disease. Gut 1991; 32:1192-7. [PMID 1955175]
- Folwaczny C, Noehl N, Endres SP, Loeschke K, Fricke H. Antineutrophil and pancreatic autoantibodies in first-degree relatives of patients with inflammatory bowel disease. Scand J Gastroenterol 1998; 33:523-8. [PMID 9648993]
- Joossens S, Vermeire S, Van Steen K, Godefridis G, Claessens G, Pierik M, et al. Pancreatic autoantibodies in inflammatory bowel disease. Inflamm Bowel Dis 2004; 10:771-7. [PMID 15626896]
- Klebl FH, Bataille F, Huy C, Hofstädter F, Schölmerich J, Rogler G. Association of antibodies to exocrine pancreas with subtypes of Crohn's disease. Eur J Gastroenterol Hepatol 2005; 17:73-7. [PMID 15647645]
- Koutroubakis IE, Drygiannakis D, Karmiris K, Drygiannakis I, Makreas S, Kouroumalis EA. Pancreatic autoantibodies in Greek patients with inflammatory bowel disease. Dig Dis Sci 2005; 50:2330-4. [PMID 16416183]
- Weersma RK, Oostenbrug LE, Nolte IM, Van Der Steege G, Oosterom E, Van Dullemen HM, et al. Association of interleukin-1 receptor-associated kinase M (IRAK-M) and inflammatory bowel diseases. Scand J Gastroenterol 2007; 42:827-33. [PMID 17558906]
- Verge CF, Stenger D, Bonifacio E, Colman PG, Pilcher C, Bingley PJ, Eisenbarth GS. Combined use of autoantibodies (IA-2 autoantibody, GAD autoantibody, insulin autoantibody, cytoplasmic islet cell antibodies) in type 1 diabetes: Combinatorial Islet Autoantibody Workshop. Diabetes 1998; 47:1857-66. [PMID 9836516]
- Winnock F, Christie MR, Batstra MR, Aanstoot HJ, Weets I, Decochez K, et al. Autoantibodies to a 38- kDa glycosylated islet cell membrane-associated antigen in (pre)type 1 diabetes: association with IA-2 and islet cell autoantibodies. Diabetes Care 2001; 24:1181-6. [PMID 11423499]
- Dupont WD, Plummer WD. PS power and sample size program available for free on the Internet. Control Clin Trials 1997; 18:274.
- Seibold F, Scheurlen M, Müller A, Jenss H, Weber P. Impaired pancreatic function in patients with Crohn's disease with and without pancreatic autoantibodies. J Clin Gastroenterol 1996; 22:202-6. [PMID 8724258]
- Foitzik T, Forgacs B, Ryschich E, Hotz H, Gebhardt MM, Buhr HJ, Klar E. Effect of different immunosuppressive agents on acute pancreatitis: a comparative study in an improved animal model. Transplantation 1998; 65:1030-6. [PMID 9583861]
- Vernier G, Sendid B, Poulain D, Colombel JF. Relevance of serologic studies in inflammatory bowel disease. Curr Gastroenterol Rep 2004; 6:482-7. [PMID 15527678]
- Quinton JF, Sendid B, Reumaux D, Duthilleul P, Cortot A, Grandbastien B, et al. Anti-Saccharomyces cerevisiae mannan antibodies combined with antineutrophil cytoplasmic autoantibodies in inflammatory bowel disease: prevalence and diagnostic role. Gut 1998; 42:788-91. [PMID 9691915]
- Cohavy O, Bruckner D, Gordon LK, Misra R, Wei B, Eggena ME, et al. Colonic bacteria express an ulcerative colitis pANCA-related protein epitope. Infect Immun 2000; 68:1542-8. [PMID 10678972]
- Targan SR, Landers CJ, Yang H, Lodes MJ, Cong Y, Papadakis KA, et al. Antibodies to CBir1 flagellin define a unique response that is associated independently with complicated Crohn's disease. Gastroenterology 2005; 128:2020-8. [PMID 15940634]

