Alphonso Brown1, Benjamin Young1, John Morton2, Kevin Behrns3, Nicholas Shaheen4
1The Beth Israel Deaconess Medical Center, Harvard Medical School. Boston, MA, USA
2Stanford Hospitals and Clinics, Stanford, CA, USA
3University of Florida, Gainesville. Gainesville, FL, USA
4Division of Digestive Diseases, The University of North Carolina at Chapel Hill School of Medicine. Chapel Hill, NC, USA
- *Corresponding Author:
- Alphonso Brown
Dana Research Center: Room 554
330 Brookline Avenue
Boston, MA 02215 USA
Phone: +1-617.667.2141
Fax: +1-617.667.1234
E-mail: abrown4@bidmc.harvard.edu
Received August 18th, 2006 - Accepted October 16th, 2006
Keywords
Epidemiology; Mortality; Pancreatitis, Acute Necrotizing; United States
Abbreviations
NIS: National Inpatient Sample
INTRODUCTION
Acute pancreatitis is a potentially fatal condition that has an estimated incidence of 17 cases/year per 100,000 inhabitants in the U.S. [1]. Within the last twenty years there has been notable improvement in our ability to diagnose this disease. It appears there has been also been a decrease in mortality associated with acute pancreatitis [2, 3]. The amount which mortality rates have changed in acute pancreatitis is not known.
Prior work in quantifying the mortality associated with acute pancreatitis has usually come from autopsy studies [4, 5, 6, 7]. Earlier reports from such data reported mortality rates associated with acute pancreatitis as high as 20% [6]. Within recent years it appears the mortality of disease has significantly decreased but it is has been difficult to decide the exact degree [1]. Another potential problem is that autopsy data may not reflect true population estimates because not all families will consent to autopsy.
The purpose of this study is to report on the frequency of discharges with a principal diagnosis of acute pancreatitis and mortality associated with acute pancreatitis within the U.S. during the period from January 1st, 1997 to December 31st, 2003. In addition, we have also reported the patient and hospital characteristics and we have evaluated how these factors may have influenced health related outcomes in acute pancreatitis.
METHODS
This study was designed to assess the frequency of discharge diagnoses of acute pancreatitis and the relative mortality of acute pancreatitis in the U.S. over the period 1997- 2003. In order to obtain a proper population based estimate of national trends we used the National Inpatient Sample (NIS) database.
Characteristics of the NIS Database
The NIS database is the largest all-payer inpatient care database in the U.S.. The NIS is a comprehensive database. It is updated yearly with data from nearly 8 million hospital stays. The most recent updates to the database contain discharge data from 994 hospitals representing 37 states. The hospitals which provide data to the NIS represent a stratified sample of 20% of all U.S. community hospitals. The most recent NIS sampling reflected data on 90% of all hospital discharges in the U.S.. This fairly large database is an excellent representative sample of the general U.S. population. The NIS database provides only administrative data for analysis. Patient specific clinical data are not available.
Search Strategy
To identify cases of acute pancreatitis we queried the NIS database in order to recover hospital data on all admissions with a primary ICD-9-CM diagnosis code of 577.0 (acute pancreatitis). All hospitalizations in which acute pancreatitis was the primary diagnosis were included in our analysis.
The query parameters were configured for the period 1997-2003. The NIS query provides a graphical user link which enables the user to get data on multiple demographic and hospital variables.
Variables Recorded
The patient demographics recorded were age and gender and the hospital characteristics recorded were type (teaching vs. nonteaching), location (urban vs. rural), and size (small, medium, and large). Teaching hospitals were defined as academic medical centers in which care was provided by faculty and physicians in training such as interns, residents and medical students. Urban centers were defined as major metropolitan areas with populations greater than 500,000 persons. The definition of bedsize varied according to the hospital location and teaching status. The range for small hospitals was from 1 to 249 beds. The bed size range for medium hospitals was from 30 to 374 and the bed size range for large hospitals was from 50 to 450 and more. The smallest hospitals were rural non-teaching hospitals in the West and Midwest. The largest hospitals were urban teaching hospitals in the Northeast and the South.
STATISTICS
The trends for the annual point estimates of the frequency of acute pancreatitis and percentage mortality for the data sample were plotted and analyzed. The annual frequency of discharges with acute pancreatitis was computed by dividing the annual number of discharges with acute pancreatitis listed in the NIS database in a given year by the total number of all discharges listed in the NIS for the same year. The chi-square test for trend was used to test for the significance of the trend of both increased frequencies in discharges with acute pancreatitis and the trend of decreased percentage mortality from acute pancreatitis observed from 1997 to 2003 and the linear regression was used to test correlations. All statistical calculations were made by using the SPSS statistical software (Version 13.0, Chicago, IL, USA). Two-tailed P values were computed.
RESULTS
Table 1 summarizes the data from the NIS for all reported cases of pancreatitis in the period 1997-2003. We identified 1,476,498 hospital discharges which had a primary ICD-9 code of 577.0 (acute pancreatitis). There were similar percentages in the number of individuals with acute pancreatitis when stratified by gender. These data are similar to results reported by other authors [8, 9]. Most of the subjects were within the age range of 18-65 with an overall mean age of 52.6 years). Most of the subjects with acute pancreatitis were from urban areas and were evaluated at non-teaching hospitals. The highest concentration of study subjects were treated at hospitals with large bed capacity.
The southern U.S. was the geographic area
with the highest number of subjects with
acute pancreatitis.
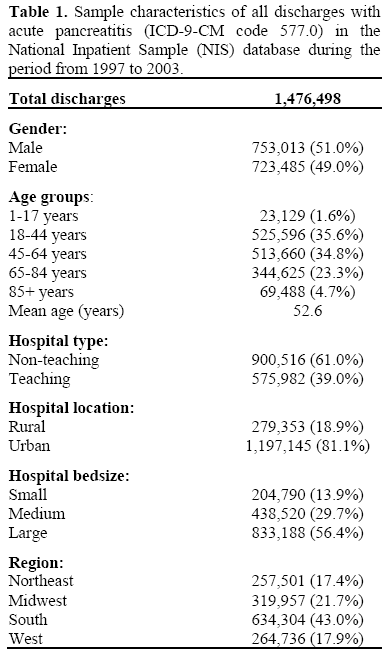
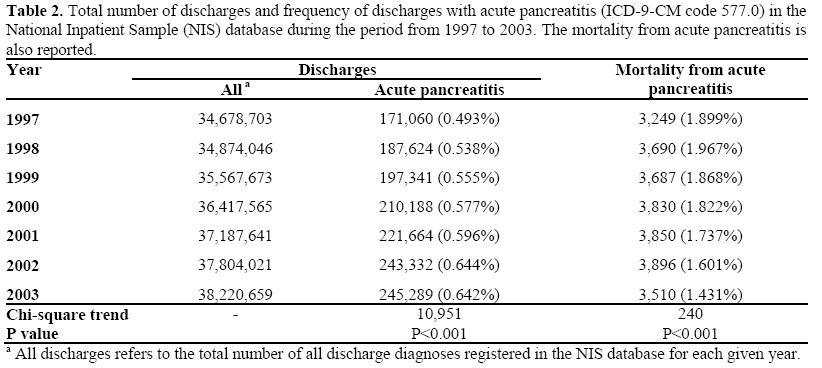
Table 2 lists the frequency of hospital
discharges with a principal diagnosis of acutepancreatitis during the period from 1997 to 2003. During this study period the frequency of discharges with acute pancreatitis increased by 30.2% (from 0.493 to 0.642%; P<0.001). while the overall mortality decreased of 35.2% (from 1.899% to 1.431%; P<0.001). The overall percentage mortality for acute pancreatitis during the study period was 1.741%. Mortality and frequency of acute pancreatitis showed a significant inverse relationship (r=-0.881; P=0.009).
The mean stay for subjects with acute pancreatitis decreased of 9.4% over the time period from 1997 to 2003 (P=0.002; Figure 1). The decrease of the hospital stay was significantly related both to the increased frequency of acute pancreatitis (r=0.949; P=0.001) and the decrease of mortality (r=0.839; P=0.018).
Figure 1. Mean length of hospital stay for patients
discharged with acute pancreatitis (ICD-9-CM code
577.0) in the National Inpatient Sample (NIS) database
during the period from 1997 to 2003.
DISCUSSION
Our study shows that during the period from 1997-2003 the frequency of individuals discharged with a diagnosis of acute pancreatitis has increased. Mortality associated with acute pancreatitis has decreased by 35.2% over the study period and was about 1.7% of all cases. The length of stay in the hospital was used as a surrogate for disease severity. It was assumed that the longer the hospital stay the sicker the patient population. Our data showed that the mean length of stay steadily decreased over the period from 1997 to 2003. Our study also found that unlike in chronic pancreatitis [10], acute pancreatitis occurs with similar frequency in males and females.
The increase in hospital discharges during the study period may be because of improvements in our ability to diagnose acute pancreatitis. During the last 20 years our imaging technology has improved dramatically. There has also been an increase in the availability of serum amylase and lipase testing. The combination of these reasons has improved our ability to diagnose acute pancreatitis in subjects who present for evaluation. One limit of the generalizability of our study results is the NIS database only captures data on subjects who are admitted to the hospital.
Individuals who are seen in the emergency room but not admitted would not be included in the analysis. There are two possible solutions to this problem. The first solution is that it is unlikely that an individual with biochemical and clinical evidence of acute pancreatitis would be discharged to home without a hospital admission. The second solution is the NIS database does provide data on where admissions come from. Individuals can be: 1) admitted directly from home; 2; admitted after emergency room evaluation; 3; admitted from another hospital; or 4) admitted from a long-term care facility. During the study period the total number of admissions from the emergency room with acute pancreatitis increased from 68.7% to 80.1% (P<0.001) (data not shown). This increase in percentage of admissions from the emergency room occurred with increasing numbers of subjects. During this period the number of direct admissions from home with a discharge diagnosis of acute pancreatitis decreased from 29% to 16% (P<0.001) (data not shown).
Another possible explanation for the increased number of discharges is there has been an increase in the clinical conditions which predispose to acute pancreatitis. In the U.S. the two most common causes of acute pancreatitis are gallstones and alcohol use. A review of the NIS database revealed that during the study period the number of hospital discharges with gallstones (ICD-9 code 574.20) increased by 11% (P<0.05; data not shown). During this same period the number of hospital admissions because of alcohol abuse (ICD-9 codes 305.0, 303.9, 303.0, 303.9) increased by 31% (P<0.05; data not shown). The increase in the number of discharges with gallstone and/or alcohol disease does not prove that either of these agents was responsible for the increase in discharges with acute pancreatitis. This observation does however; provide a logical theory for the observed increase in the incidence of acute pancreatitis. Well designed clinical trials in which strength of association is directly measured would provide a more definitive answer to this question. Despite the observed increase in discharges of subjects with acute pancreatitis the mortality associated with acute pancreatitis steadily decreased during the study period. The U.S. mortality trend mirrors what has been seen in several other countries during a similar time period [11, 12, 13, 14, 15, 16, 17, 18]. One possible explanation for the decrease in mortality is the more efficient diagnosis and severity stratification of subjects with acute pancreatitis. Early diagnosis of severe complications of pancreatitis is important because ICU care is believed to be critical to clinical improvement [19]. During the study period there was a greater than 15% increase in the number of ICU beds in the U.S. [20]. Nearly 99% of the deaths that occur in severe acute pancreatitis occur in subjects with severe complications of disease [21, 22]. It is accepted that individuals with severe complications of acute pancreatitis should be managed in an ICU. It is important to note there is no data showing that ICU care improves outcomes in severe acute pancreatitis. We can only infer based on secular trends the decreased mortality in acute pancreatitis correlate with an increase of the availability of high-level care centers such as ICUs.
Our data show that the majority of subjects with a diagnosis of acute pancreatitis are being seen in large urban areas. This trend is likely to reflect population demographics since urban areas tend to be more population dense. Almost 50% of discharges with a diagnosis of acute pancreatitis were at hospitals located in the South. The reason for this is unclear but one possible explanation is that obesity rates in the southern U.S. are among the highest in the nation. Obesity is a risk factor for developing gallstone disease. During the study period the percentage of individuals seen at hospitals in the South who had a discharge diagnosis of gallstones increased by 1.5% (P<0.05). During the study period hospitals in the south had the greatest percentage (41%) of discharges in which gallstones were the principal diagnosis. The second highest percentage of individuals with gallstones as the principal discharge diagnosis was the Northeast which averaged only 21% of the total hospital admissions over the study period.
Our data provide new insights into the epidemiology of acute pancreatitis in a large hospital based cohort. Our study design and the data used provide some limitations which must be considered when attempting to generalize. One limitation of our data is that this is an administrative data set which is reflective of the coding practices of the data abstractors. We have no way of controlling for errors that may have occurred during the data entry. We cannot also obtain individual patient specific clinical data but can only comment on the characteristics of the research sample. Newer versions of the NIS database will allow for assessment of patient comorbidities. One final limitation of this analysis is that our study is an ecological study and can only comment on secular trends. To prove causality between associations seen here would require analytic studies (cohort, RCT, or case-control).
These data represent a large sample of the characteristics of hospitalized patients with acute pancreatitis. It appears the incidence of acute pancreatitis is increasing while mortality has fallen. Continued investigation will help better define which potentially modifiable factors have the strongest association with our reported trends.
Acknowledgement
The Center for Gastrointestinal Biology and Disease (Princeton, NJ, USA) and The Robert Wood Johnson Foundation (Princeton, NJ, USA)
Conflict of interest
The authors have no potential conflicts of interest
References
- Kimura Y, Takada T, Kawarada Y, Hirata K, Mayumi T, Yoshida M, et al. JPN Guidelines for the management of acute pancreatitis: treatment of gallstone-induced acute pancreatitis. J HepatobiliaryPancreatSurg 2006; 13:56-60. [PMID 16463212]
- Tinto A, Lloyd DA, Kang JY, Majeed A, Ellis C, Williamson RC, Maxwell JD. Acute and chronic pancreatitis--diseases on the rise: a study of hospital admissions in England 1989/90-1999/2000. Aliment PharmacolTher 2002; 16:2097-105. [PMID 12452943]
- Andersson R, Andersson B, Haraldsen P, Drewsen G, Eckerwall G. Incidence, management and recurrence rate of acute pancreatitis. Scand J Gastroenterol 2004; 39:891-4. [PMID 15513389]
- Corfield AP, Cooper MJ, Williamson RC. Acute pancreatitis: a lethal disease of increasing incidence. Gut 1985; 26:724-9. [PMID 4018637]
- Wilson C, Imrie CW. Deaths from acute pancreatitis: why do we miss the diagnosis so frequently? Int J Pancreatol 1988; 3:273-81. [PMID 2455008]
- Mann DV, Hershman MJ, Hittinger R, Glazer G. Multicentre audit of death from acute pancreatitis. Br J Surg 1994; 81:890-3. [PMID 8044613]
- Fan ST, Choi TK, Lai CS, Wong J. Influence of age on the mortality from acute pancreatitis. Br J Surg 1988; 75:463-6. [PMID 3390679]
- Gullo L, Migliori M, Oláh A, Farkas G, Levy P, Arvanitakis C, et al. Acute pancreatitis in five European countries: etiology and mortality. Pancreas 2002; 24:223-7. [PMID 11893928]
- Kim CD. Current status of acute pancreatitis in Korea. Korean J Gastroenterol 2003; 42:1-11. [PMID 14532725]
- Lowenfels AB, Maisonneuve P, Grover H, Gerber E, Korsten MA, Antunes MT, et al. Racial factors and the risk of chronic pancreatitis. Am J Gastroenterol 1999; 94:790-4. [PMID 10086667]
- Talamini G, Bassi C, Falconi M, Sartori N, Frulloni L, Di Francesco V, et al. Risk of death from acute pancreatitis. Role of early, simple "routine" data. Int J Pancreatol 1996; 19:15-24. [PMID 8656023]
- Lowham A, Lavelle J, Leese T. Mortality from acute pancreatitis. Late septic deaths can be avoided but some early deaths still occur. Int J Pancreatol 1999; 25:103-6. [PMID 10360222]
- Mutinga M, Rosenbluth A, Tenner SM, Odze RR, Sica GT, Banks PA. Does mortality occur early or late in acute pancreatitis? Int J Pancreatol 2000; 28:91-5. [PMID 11128978]
- Blum T, Maisonneuve P, Lowenfels AB, Lankisch PG. Fatal outcome in acute pancreatitis: its occurrence and early prediction. Pancreatology 2001; 1:237-41. [PMID 12120201]
- Kandasami P, Harunarashid H, Kaur H. Acute pancreatitis in a multi-ethnic population. Singapore Med J 2002; 43:284-8. [PMID 12380724]
- Ma XX, Galiana A, Pedreira W, Mowszowicz M, Christophersen I, Machiavello S, et al. Communityacquired methicillin-resistant Staphylococcus aureus, Uruguay. Emerg Infect Dis 2005; 1:973-6. [PMID 15963301]
- Lankisch PG, Assmus C, Maisonneuve P, Lowenfels AB. Epidemiology of pancreatic diseases in Lüneburg County. A study in a defined german population. Pancreatology 2002; 2:469-77. [PMID 12378115]
- Floyd A, Pedersen L, Nielsen GL, Thorladcius- Ussing O, Sorensen HT. Secular trends in incidence and 30-day case fatality of acute pancreatitis in North Jutland County, Denmark: a register-based study from 1981-2000. Scand J Gastroenterol 2002; 37:1461-5. [PMID 12523598]
- Nathens AB, Curtis JR, Beale RJ, Cook DJ, Moreno RP, Romand JA, et al. Management of the critically ill patient with severe acute pancreatitis. Crit Care Med 2004; 32:2524-36. [PMID 15599161]
- Halpern NA, Pastores SM, Greenstein RJ. Critical care medicine in the United States 1985-2000: an analysis of bed numbers, use, and costs. Crit Care Med 2004; 32:1254-9. [PMID 15187502]
- Johnson CD, Kingsnorth AN, Imrie CW, McMahon MJ, Neoptolemos JP, McKay C, et al. Double blind, randomised, placebo controlled study of a platelet activating factor antagonist, lexipafant, in the treatment and prevention of organ failure in predicted severe acute pancreatitis. Gut 2001; 48:62-9. [PMID 11115824]
- Ogawa M, Hirota M, Hayakawa T, Matsuno S, Watanabe S, Atomi Y, et al. Development and use of a new staging system for severe acute pancreatitis based on a nationwide survey in Japan. Pancreas 2002; 25:325-30. [PMID 12409824]


