Keywords
erlotinib; gemcitabine; Pancreatic Neoplasms; S 1 (combination)
Abbreviations
GTX: gemcitabine, docetaxel and capecitabine; S- 1: tegafur, 5-chloro-2,4-dihydroxyuridine and potassium oxonate; SPARC: secreted protein acidic and rich in cysteine; Src: v-src sarcoma (Schmidt-Ruppin A-2) viral oncogene homolog (avian)
INTRODUCTION
Pancreatic cancer remains the 4th cause of cancer death after lung, prostate (breast in women), and colorectal cancer since 1970s in the USA [1]. Small localized tumors can be possibly cured by surgical resection, however, majority of the tumors are either locally advanced or metastatic upon diagnosis. Among all studied chemotherapeutic agents, gemcitabine was the only one demonstrating a significantly higher clinical benefit response compared to historical 5-fluorouracil (5-FU) infusion [2]. Since 1997, gemcitabine established its unshakable status as first-line therapy for advanced pancreatic cancer. Various combinations using gemcitabine as a backbone were subsequently investigated in large randomized clinical trials; none of the combinations is proved to be superior to gemcitabine monotherapy except erlotinib plus gemcitabine [3].
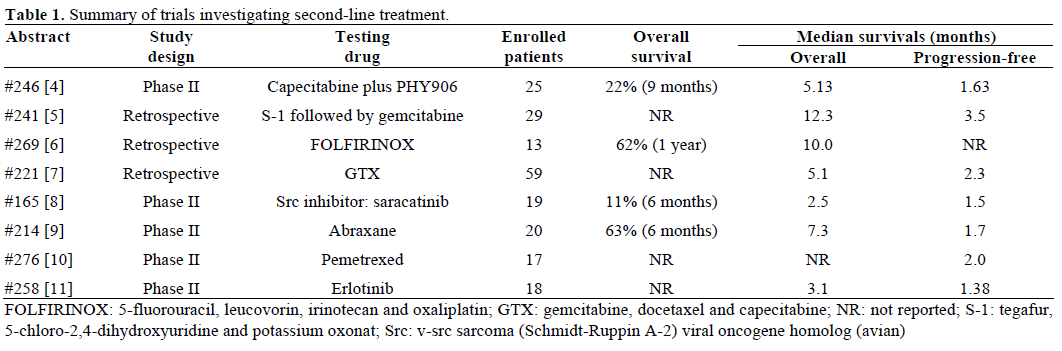
What if patients are not responding to first-line gemcitabine-based regimen? Is there a standard second-line therapy? Unfortunately, the answer is still no, though there is growing evidence supporting some benefit of chemotherapy after gemcitabine in selected patients. Several encouraging abstracts presented on the 2010 ASCO Gastrointestinal Cancers Symposium in the field of pancreatic cancer deserve a discussion here (Table 1).
Combination Therapies
Capecitabine plus Chinese Herbal Medicine PHY906
PHY906 has not only synergistic antitumor activity with several chemotherapeutic agents including irinotecan, capecitabine and gemcitabine, but also cytoprotective effect. Our institute, Yale Cancer Center, has opened several early phase trials investigating the use of PHY906 in different types of cancers such as colorectal, pancreatic cancer and hepatocellular carcinoma. In our phase II trial, PHY906 is administered with capecitabine for patients refractory to first-line gemcitabine therapy [4]. The anti-diarrhea and anti-hand-foot syndrome effects were very promising. In patients who received more than 2 cycles, median overall survival was 6.8 months.
S-1 Followed by Gemcitabine
Among all combination trials, tegafur, 5-chloro-2,4- dihydroxyuridine and potassium oxonate (S-1) followed by gemcitabine sequential use is probably the most exciting one. Its anti-tumor activity has been explored beyond gastric cancer in Japan. S-1 and gemcitabine were administrated sequentially in 29 patients with gemcitabine refractory pancreatic cancer [5]. One patient (3.4%) achieved complete response and 5 patients (17.2%) achieved partial response. Median overall and progression free survivals were 12.3 and 3.5 months, respectively.
5-Fluorouracil, Leucovorin, Irinotecan and Oxaliplatin (FOLFIRINOX)
Both oxaliplatin and irinotecan are known to have survival benefit in combination with 5-fluorouracil and leucovorin (5-FU/LV) in metastatic colorectal cancer. Breysacher et al. reported a retrospective study investigating the role of FOLFIRINOX as second-line therapy [6]. No response was seen in 13 patients and 1- year survival rate was 62%. GI toxicity was frequent but mild and manageable.
Gemcitabine, Docetaxel, and Capecitabine (GTX) Regimen
GTX regimen has shown activity in both neoadjuvant and metastatic settings. No data exists on the use of GTX in second-line. In a retrospective study of 59 patients received GTX after initial standard therapies, a drop greater than 75% in CA 19-9 after treatment predicted longer overall survival [7].
Single Agents
Abraxane
Pancreatic cancer cells and surrounding stroma overexpress SPARC (secreted protein acidic and rich in cysteine). Abraxane increased tumor accumulation of paclitaxel through binding of albumin to SPARC. Abraxane plus gemcitabine did demonstrate clinical benefit in early phase trials [12]. Abraxane alone appears to be promising as well. One of 19 patients (5.3%) achieved partial response [8]. Whether SPARC expression is a predicative biomarker needs further investigation.
Pemetrexed
In a phase II trial, pemetrexed rendered median progression free survival of 2 months to patients who failed gemcitabine [8]. No concerning adverse events were found except grade 3 neutropenia in two patients (10.5%).
Molecular Target Therapy
Erlotinib with gemcitabine combination gained FDA approval for a small overall survival benefit. However, when erlotinib used as single agent, it lost this modest benefit completely [9]. Src family tyrosine kinases are overexpressed in pancreatic cancers. The anti-tumor activity of Src inhibitor saracatinib was demonstrated in a mouse model [13]. Unfortunately, saracatinib failed to improve 6-month survival in a phase II trial [10]. Only 2 of 18 patients survived beyond 6 months (11.1%).
Discussion
Options for pancreatic cancer in advanced or metastatic setting remain limited. Gemcitabine as the only FDAapproved chemotherapeutic agent has been intensively and extensively investigated in combination with other drugs; unfortunately, no additional benefit was seen. Unlike the first-line setting, there is no standard of care after gemcitabine failure. Drugs in this setting should consider clinical benefit more importantly than antitumor activity. Several abstracts report either single agents or combinations with or without gemcitabine did demonstrate some potential clinical benefit. Chinese herbal medicine PHY906 provides convincing cytoprotective effect when used in combination with chemotherapeutic agents. More clinical trials of PHY906 are being conducted at Yale Cancer Center. FOLFIRINOX is also an interesting and promising combination. Surprisingly, the toxicity profile was not alarming. Other two combinations continued to use gemcitabine even after failure in the initial therapy. Sequential S-1 and gemcitabine should be tested in clinical trial setting. Among single agents, abraxane and pemetrexed warrant further investigation.
Conflict of interest
The authors have no potential conflicts of interest
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, ThunMJ. Cancer Statistics, 2009. CA Cancer J Clin 2009; 59:225-49. [PMID 19474385]
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, ModianoMR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J ClinOncol 1997; 15:2403-13. [PMID 9196156]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J ClinOncol 2007; 25:1960-6. [PMID 17452677]
- Saif M, Li J, Chu E, Lamb L, Kaley K, Elligers K, et al. Phase II study of PHY906 plus capecitabine (CAP) in patients with gemcitabine-refractory advanced pancreatic cancer (APC). 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 246.
- Nakamori S, Tsujie M, Miyamoto A, Kurokawa Y, Yasui M, Ikenaga M, et al. Impact of the combination of S-1 administration prior to gemcitabine as a second-line therapy for unresectable/recurrent pancreatic cancer. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 241.
- Breysacher G, Kaatz O, Lemarignier C, Chiappa P, Roncalez D, Denis B; et al. Safety and clinical effectiveness of FOLFIRINOX in metastatic pancreas cancer (MPC) after first-line chemotherapy. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 269.
- Dakik HK, Moskovic DJ, Carlson PJ, Qiao W, Ho L, Tamm E, et al. Evaluation of gemcitabine, docetaxel, capecitabine (GTX) in previously treated pancreatic cancer. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 221.
- Nallapareddy S, Arcaroli J, Touban B, Tan A, Foster NR, Erlichman C, et al. A phase II trial of saracatinib (AZD0530), an oral Src inhibitor, in previously treated metastatic pancreatic cancer. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 165.
- HoseinPJ, PastoriniVH, Gomez CM, Macintyre J, Merchan JR, Ferrell A, et al. A phase II trial of nab-paclitaxel (NP) in patients with advanced pancreatic cancer (PC) who have progressed on gemcitabine-based therapy. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 214.
- Iyer RV, Khushalani NI, Tan W, Litwin A, Starostik P, Levea C, et al. A phase II study of erlotinib in patients (pts) with advanced pancreatic cancer (APC) who are refractory to gemcitabine (G). 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 258.
- Bai W, He AR, PishvaianMJ, Slack R, Marshall J, Ley L, et al. Pemetrexed as second-line treatment in patients with advanced pancreatic cancer progressing after gemcitabine. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 276.
- Von Hoff DD, Ramanathan R, Borad M, Laheru D, Smith L, Wood T, et al. SPARC correlation with response to gemcitabine (G) plus nab-paclitaxel (nab-P) in patients with advanced metastatic pancreatic cancer: A phase I/II study. J ClinOncol 2009; 27(15 Suppl):Abstract 4525.
- Rajeshkumar NV, Tan AC, De Oliveira E, Womack C, Wombwell H, Morgan S, et al. Antitumor effects and biomarkers of activity of AZD0530, a Src inhibitor, in pancreatic cancer. Clin Cancer Res 2009; 15:4138-46. [PMID 19509160]

