Keywords
Clinical Trials as Topic; Disease-Free Survival; erlotinib; gemcitabine; Pancreatic Neoplasms; Survival
Abbreviations
CONKO: Charité Onkologie; LMWH: low molecular weight heparin
INTRODUCTION
American Cancer Society has estimated in 2009, there will be 21,050 new pancreatic cancer cases in men and 21,420 in women, while 35,240 (about 83%) will die of pancreatic cancer in 2009 [1]. Pancreatic cancer remains the 4th cause of death by cancer after lung, prostate (breast in women), colorectal cancer since 1970s in the USA, although it represents only 2-3% of all cancers. Endless effort has been put on this aggressive disease; however, surgical resection remains the only curative option. Locally advanced or metastatic diseases are considered non-curable, palliative chemotherapies are often administered for alleviating symptoms. Fluorouracil (5-FU) had been the only active drug in pancreatic cancer for over decades until the emerging of gemcitabine in 1997 [2]. A significantly higher clinical benefit response associated with gemcitabine treatment was observed (23.8% vs. 4% in 5-FU arm) although the overall objective response rate remained modest [2]. Based on these results, FDA approved gemcitabine as the first line therapy for advanced pancreatic cancer in 1997. Since then, various combinations using gemcitabine as a backbone were designed and tested in clinical trials. Unfortunately, none of the combinations is proved to be superior to gemcitabine monotherapy.
With the advances in molecular biology, newer biologic agents such as erlotinib, cetuximab and bevacizumab are adding some benefit to the conventional cytotoxic agents. Unfortunately, these agents all failed to show any significant superiority over gemcitabine except the combination of erlotinib plus gemcitabine [3]; however, the clinical impact of this combination remains very controversial until now. The disappointing results did not discourage investigators but stimulated them to look for more pharmaceutical agents or combinations. We have gladly seen over 80 abstracts presented in the 2009 annual meeting of the American Society of Clinical Oncology (ASCO) in the field of pancreatic cancer. In this highlight article, we will focus on the management of advanced (locally advanced and metastatic) pancreatic cancer.
Since the approval of gemcitabine, true progress in the management of pancreatic cancer has been very minimal. There has been persistent effort in the field of medical oncology regards to explore novel agents based on better understanding of the diseases.
1. First-Line Therapies
Current standard first-line therapies for advanced pancreatic cancer are gemcitabine or gemcitabine plus erlotinib. A number of abstracts are exploring further first-line options. Interestingly, gemcitabine remains the core of the combinations.
1.1 Phase III Trials
Three large trials were presented (Table 1) [4, 5, 6]; unfortunately, two large trials (Abstracts #4504 and #4601) failed to prove any additional benefit of a second cytotoxic agent or a vaccine. The third trial (Abstract #4604) comparing erlotinib plus capecitabine with erlotinib plus gemcitabine only presented interim toxicity data from 127 patients, efficacy data are pending. To think beyond the gemcitabine box and search for novel agents have become crucially urgent in order to conquer this very aggressive disease.
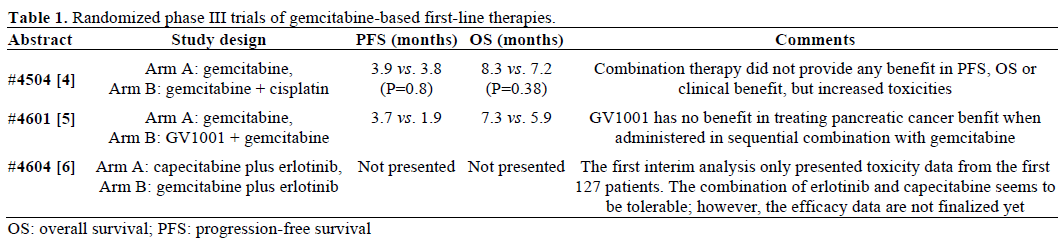
1.1.1 Gemcitabine vs. Gemcitabine plus Cisplatin
The “Gruppo Oncologico dell’Italia Meridionale” conducted a phase III trial to compare gemcitabine with or without oxaliplatin, the benefit was only observed in progression-free survival but not overall survival, however later pooled- and meta-analysis proved that the addition of platinum to gemcitabine did offer survival benefit in selected patients [7, 8, 9]. The “Gruppo Italiano Pancreas” (GIP) conducted another superiority study to compare gemcitabine monotherapy with gemcitabine plus cisplatin in advanced pancreatic cancer patients [4]. The data were presented in this annual meeting. A total of 400 patients were enrolled from 46 Italian institutions. One-hundred and ninetynine patients received gemcitabine single agent (1,000 mg/m2 weekly x 7, then weekly x 3 every 4 weeks), whereas the other 201 patients received combination therapy of gemcitabine plus cisplatin (in addition to gemcitabine administered as above, cisplatin was given at 25 mg/m2 weekly). Surprisingly, this large trial did not demonstrate any survival benefit by adding cisplatin to gemcitabine. The results not only confirmed a previously published negative phase III trial, but also warned all clinicians to carefully interpret pooled or meta-analyses.
1.1.2 Gemcitabine vs. GV1001 plus Gemcitabine
GV1001 is a telomerase peptide vaccine which showed a median overall survival of 8.6 months in nonresectable pancreatic cancer [10]. In order to compare the efficacy of a combination therapy of GV1001 and gemcitabine with gemcitabine monotherapy, a phase III trial was designed [5]. A total of 520 patients were planned. Patients were randomly assigned to either gemcitabine monotherapy (1,000 mg/m2 over 30 min weekly x 7, then weekly x 3 every 4 weeks) or a sequential combination of GV1001 and gemcitabine (GV1001 0.56 mg subcutaneous plus granulocytemacrophage colony-stimulating factor as immune adjuvant on days 1, 3, 5, 8, 15, 22, 36, then every 4 weeks, gemcitabine was added when disease progressed on GV1001). Unfortunately, after 365 patients were enrolled, a preliminary analysis indicated no survival benefit by giving GV1001. Thus this trial was prematurely terminated.
1.1.3 Erlotinib plus Capecitabine vs. Erlotinib plus Gemcitabine
Erlotinib has been proved to have effect in combination with gemcitabine for advanced pancreatic cancer. Whether erlotinib can be combined with other cytotoxic agents such as capecitabine in treating advanced pancreatic cancer was investigated in a phase III trial conducted by the “Arbeitsgemeinschaft Internistische Onkologie” (AIO) group [6]. Twohundred and eighty-one patients randomly received either capecitabine (200 mg/m2/day, days 1-14 every 3 weeks) plus erlotinib (150 mg/day) or gemcitabine (1,000 mg/m2 over 30 min weekly x 7, then weekly x 3 every 4 weeks) plus erlotinib. The first interim analysis was reported on the meeting. Sixty patients received capecitabine plus erlotinib, 67 patients received gemcitabine plus erlotinib. Toxicity data indicated that erlotinib can be safely combined with capecitabine; however, the efficacy data are not completed yet. Whether this combination could achieve similar efficacy in terms of progression free survival and/or overall survival as the combination of erlotinib with gemcitabine, we will have to wait for the final results.
1.2 Phase I/II Trials
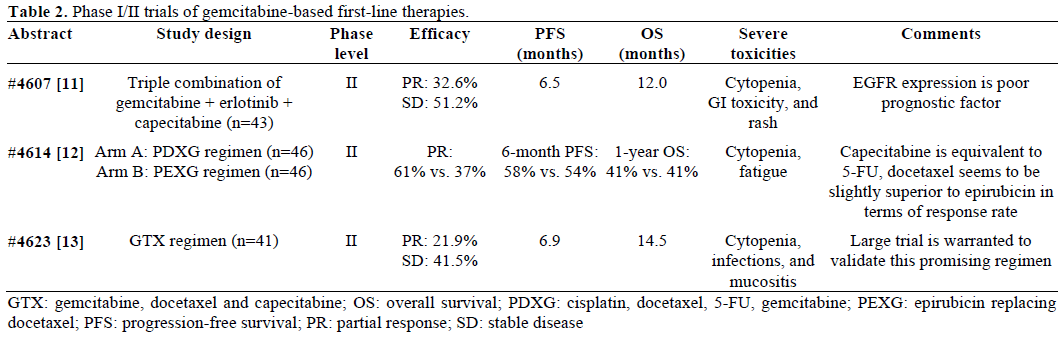
Several phase I/II trials studied more combinations, including four novel agents which will be discussed in more details in next section (Tables 2 and 3).

2. Second-Line Therapies
Lack of attention to second line treatment strategy in advanced pancreatic cancer is due to the fact that we still do not have first line option that renders true survival benefit; therefore, development of novel therapeutic agents should be an obvious area of our focus in the future. However, there is growing evidence supporting benefit of chemotherapy after gemcitabine failure in selected patients with good performance status [14].
Few clinical trials investigating second-line options in patients with advanced pancreatic cancer after failure of gemcitabine were presented at the meeting. One study aimed at exploring folinic acid plus 5-FU plus oxaliplatin (FOLFOX) and 5-fluorouracil plus leucovorin plus irinotecan (FOLFIRI.3), two commonly used regimens in colorectal cancer in this setting (Aabstract #4618) [15]. Sixty patients were randomly assigned to either FOLFOX (oxaliplatin 85 mg/m2 over 120 min on day 1, leucovorin 400 mg/m2 on day 1, 5-FU 2,000 mg/m2 over 46 hours every two weeks) or FOLFIRI.3 (irinotecan 70 mg/m2 over 60 min on day 1, leucovorin 400 mg/m2 over 2 hours on day 1, 5-FU 2,000 mg/m2 over 46 hours from day 1, then irinotecan 70 mg/m2 over 60 min at the end of the 5-FU infusion every two weeks). Six-month overall survival rate in both arms were 25% and 20%, respectively. Based on patients’ overall performance status, and prior chemotherapy toxicities, these two regimens can certainly be considered as second-line option; however, the clinical benefit needs to be validated in larger trials.
Current standard dose of erlotinib is 100 mg/day in combination with gemcitabine [3]. Skin acne-like rash has been proposed to be a “surrogate” marker for response to biologic agents such as erlotinib and cetuximab. In the 2007 ASCO Gastrointestinal Cancers Symposium (Orlando, FL, U.S.A.; January 20th, 2007), Van Cutsem et al. presented a dose-escalation study of cetuximab in colorectal cancer (EVEREST). The higher grade of skin rash correlating with increased response rate was observed [17]. Whether this “surrogate” marker can be used to maximize the benefit from erlotinib was studied by Tang et al. in a phase II trial [16]. Fifty patients with gemcitabinerefractory pancreatic cancer were orally administered erlotinib starting at 150 mg/day, dose-escalating by 50 mg every two weeks until rash more than grade 1 or maximum dose of 300 mg/day (Figure 1). Twenty-five percent of eligible patients achieved stable disease for more than 8 weeks which met the primary end-point of this trial. This trial certainly revolutionized our understanding of erlotinib. It is worthwhile to perform a large trial to validate these results and re-compare gemcitabine with or without erlotinib in which the dose of erlotinib should be based on skin rash.
Figure 1. Schema of phase II erlotinib single agent as second-line
therapy.
3. Novel Agents
Development of novel therapeutic agents is an obvious area of focus of research in pancreatic cancer. Several novel agents either new biologic target agents (AMG655 and masitinib) or newly formulated conventional cytotoxic agents (endoTAG-1 and nabpaclitaxel) are tested and results are promising (Table 3)
4. Supportive Therapy
Palliative care represents an important aspect of care in patient with pancreatic malignancy. Identifying and treating disease related symptomatology are priorities [22]
The incidence of venous thromboembolism in pancreatic cancer patients ranges from 17% to 57%. Clinical data also suggest that the occurrence of venous thromboembolism may be associated with poorer prognosis in such patients. Recent data suggest that anticoagulant treatments may improve cancer patient survival by decreasing thromboembolic complications as well as by anticancer effects [23]. Riess et al. conducted the “Charité Onkologie” (CONKO-004) trial to investigate whether the addition of enoxaparin, a low molecular weight heparin (LMWH) improves overall survival (Abstract #LBA4506) [24]. Safety and feasibility of adding enoxaparin to chemotherapy have been completed in their previously published pilot study “Prospective, Randomized trial Of Simultaneous Pancreatic cancer treatment with Enoxaparin” (PROSPEC-CONKO-004) [25]. The primary endpoint was to decrease the incidence of symptomatic venous thromboembolic events. Three-hundred and twelve patients were enrolled, 160 patients were treated with chemotherapy plus enoxaparin. The occurrence of venous thromboembolic events were 8/160 (5.0%) compared with 14.5% in the non-LMWH arm (Table 4). Clearly, enoxaparin is effective and safe for prevention of symptomatic venous thromboembolic events; however, whether the low incidence of venous thromboembolic events is associated with some survival benefit is still unclear. CONKO-004 preliminary data showed no difference in median overall survival with or without exnoxaparin. We are looking forward to their final results.

Future Directions
Options for pancreatic cancer in advanced/metastatic setting are still very limited. Gemcitabine remains the standard of care despite so many combinations were examined. The two large phase III trials failed to show any benefit beyond gemcitabine monotherapy by adding a second cytotoxic agent such as cisplatin or a vaccine GV1001. These combinations were promising in early phase trials or pooled/meta-analysis. Again, we should be careful when interpreting results from early phase trials. Many promising results from phase II trials were unable to be translated into phase III trials. Over the last 12 years, we have extensively and intensively explored all possible agents to combine with gemcitabine, it is the time to think out of the gemcitabine box and put more effort on novel agents. Nab-paclitaxel, “an old drug in a new bottle”, seems to be very promising when combined with gemcitabine. We are looking forward to the phase III results. New biologic target agent such as AMG655, a monoclonal antibody against human death receptor-5, also achieved encouraging results. However, the current designs of clinical trials in advanced pancreatic cancer still rely on gemcitabine, even for the aforementioned novel agents. Nevertheless, gemcitabine is the only cytotoxic agent providing significant clinical benefit for pancreatic cancer. We encourage more novel agents should be tested in second-line setting.
Conflict of interest
The authors have no potential conflicts of interest
References
- National Cancer Institute, Surveillance Epidemiology and End Results. Pancreas. SEER Stat Fact Sheets (https://seer.cancer.gov/statfacts/html/pancreas.html).
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997; 15:2403-13. [PMID 9196156]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007; 25:1960-6. [PMID 17452677]
- Colucci G, Labianca R, Di Costanzo F, Gebbia V, Cartenì G, Massidda B, et al. A randomized trial of gemcitabine (G) versus G plus cisplatin in chemotherapy-naive advanced pancreatic adenocarcinoma: The GIP-1 (Gruppo Italiano Pancreas- GOIM/GISCAD/GOIRC) study. J Clin Oncol 2009; 27(15 Suppl.): Abstract 4504.
- Buanes T, Maurel J, Liauw W, Hebbar M, Nemunaitis J. A randomized phase III study of gemcitabine (G) versus GV1001 in sequential combination with G in patients with unresectable and metastatic pancreatic cancer (PC). J Clin Oncol 2009; 27(15 Suppl.): Abstract 4601.
- Heinemann V, Vehling-Kaiser U, Waldschmidt D, Kettner E, Marten A, Winkelmann, et al. Gemcitabine plus erlotinib followed by capecitabine versus capecitabine plus erlotinib followed by gemcitabine: Interim toxicity analysis of a multicenter, randomized, cross-over phase III trial of the Arbeitsgemeinschaft Internistische Onkologie (AIO). J Clin Oncol 2009; 27(15 Suppl.): Abstract 4604.
- Louvet C, Labianca R, Hammel P, Lledo G, Zampino MG, André T, et al. Gemcitabine in combination with oxaliplatin compared with gemcitabine alone in locally advanced or metastatic pancreatic cancer: results of a GERCOR and GISCAD phase III trial. J Clin Oncol 2005; 23:3509-16. [PMID 15908661]
- Heinemann V, Labianca R, Hinke A, Louvet C. Increased survival using platinum analog combined with gemcitabine as compared to single-agent gemcitabine in advanced pancreatic cancer: pooled analysis of two randomized trials, the GERCOR/GISCAD intergroup study and a German multicenter study. Ann Oncol 2007; 18:1652-9. [PMID 17660491]
- Heinemann V, Boeck S, Hinke A, Labianca R, Louvet C. Metaanalysis of randomized trials: evaluation of benefit from gemcitabine-based combination chemotherapy applied in advanced pancreatic cancer. BMC Cancer 2008; 8:82. [PMID 18373843]
- Bernhardt SL, Gjertsen MK, Trachsel S, Møller M, Eriksen JA, Meo M, et al. Telomerase peptide vaccination of patients with nonresectable pancreatic cancer: A dose escalating phase I/II study. Br J Cancer 2006; 95:1474-82. [PMID 17060934]
- Oh D, Lee K, Lee K, Sohn C, Park Y, Zang D, et al. A phase II trial of erlotinib in combination with gemcitabine and capecitabine in previously untreated metastatic/recurrent pancreatic cancer: Combined analysis with translational research. J Clin Oncol 2009; 27(15 Suppl.): Abstract 4607.
- Cereda S, Rognone A, Ghidini M, Rezzonico S, Passoni P, Mazza E, et al. A randomized phase II trial of two different four-drug combinations in advanced pancreatic adenocarcinoma: Cisplatin, capecitabine, gemcitabine plus either epirubicin or docetaxel. J Clin Oncol 2009; 27(15 Suppl.): Abstract 4614.
- Fine R, Moorer G, Sherman W, Chu, Maurer KM, Chabot J, et al. Phase II trial of GTX chemotherapy in metastatic pancreatic cancer. J Clin Oncol 2009; 27(15 Suppl.): Abstract 4623.
- Kang SP, Saif MW. Optimal second line treatment options for gemcitabine refractory advanced pancreatic cancer patients. Can we establish standard of care with available data? JOP. J Pancreas (Online) 2008; 9:83-90. [PMID 18326918]
- Hwang JY, Yoo C, Kim T, Lee J, Park D, Seo D, et al. A randomized phase II study of FOLFOX or FOLFIRI.3 as second-line therapy in patients with advanced pancreatic cancer previously treated with gemcitabine-based chemotherapy. J Clin Oncol 2009; 27(15 Suppl.): Abstract 4618.
- Tang P, Gill S, Au HJ, Chen EX, Hedley D, Leroux M, et al. Phase II trial of erlotinib in advanced pancreatic cancer (PC). J Clin Oncol 2009; 27(15 Suppl.): Abstract 4609.
- Van Cutsem E, Humblet Y, Gelderblom H, Vermorken JB, Vire Ft, Glimelius B, et al. Cetuximab dose-escalation study in patients with metastatic colorectal cancer (mCRC) with no or slight skin reactions on cetuximab standard dose treatment (EVEREST): Pharmacokinetic and efficacy data of a randomized study. 2007 ASCO Gastrointestinal Cancers Symposium. Abstract #237.
- Kindler HL, Garbo L, Stephenson J, Wiezorek J, Sabin T, Hsu M, et al. A phase Ib study to evaluate the safety and efficacy of AMG 655 in combination with gemcitabine (G) in patients (pts) with metastatic pancreatic cancer (PC). J Clin Oncol 2009; 27(15 Suppl.): Abstract 4501.
- Von Hoff DD, Ramanathan R, Borad M, Laheru D, Smith L, Wood T, et al. SPARC correlation with response to gemcitabine (G) plus nab-paclitaxel (nab-P) in patients with advanced metastatic pancreatic cancer: A phase I/II study. J Clin Oncol 2009; 27(15 Suppl.): Abstract 4525.
- Loehr M, Bodoky G, Fölsch U, Märten A, Karrasch M, Lilla C, et al. Cationic liposomal paclitaxel in combination with gemcitabine in patients with advanced pancreatic cancer: A phase II trial. J Clin Oncol 2009; 27(15 Suppl.): Abstract 4526.
- Hammel P, Mornex F, Deplanque G, Mitry E, Levy P, Seitz J, et al. Oral tyrosine kinase inhibitor masitinib in combination with gemcitabine in patients with advanced pancreatic cancer: A multicenter phase II study. J Clin Oncol 2009; 27(15 Suppl.): Abstract 4617.
- Fazal S, Saif MW. Supportive and palliative care of pancreatic cancer. JOP. J Pancreas (Online) 2007; 8:240-53. [PMID 17356251]
- Sohail MA, Saif MW. Role of anticoagulation in the management of pancreatic cancer. JOP. J Pancreas (Online) 2009; 10:82-7. [PMID 19287098]
- Riess H, Pelzer U, Deutschinoff G, Opitz B, Stauch M, Reitzig P, et al. A prospective, randomized trial of chemotherapy with or without the low molecular weight heparin (LMWH) enoxaparin in patients (pts) with advanced pancreatic cancer (APC): Results of the CONKO 004 trial. J Clin Oncol 2009; 27(18 Suppl.): Abstract LBA4506.
- Riess H, Pelzer U, Hilbig A, Stieler J, Opitz B, Scholten T, et al. Rationale and design of PROSPECT-CONKO 004: a prospective, randomized trial of simultaneous pancreatic cancer treatment with enoxaparin and chemotherapy). BMC Cancer. 2008 Dec 5;8:361. [PMID 19055847]


