Keywords
access, evaluation, healthcare quality, immigrants, parturition, postnatal depression, pregnancy
Introduction
Canada is currently experiencing large-scale immigration and increasing ethnocultural diversity. The country’s population increased by 5.9% between the 2006 and 2011 censuses, compared with a 5.4% increase during the previous 5-year period; this increase in growth rate was attributable to slightly higher fertility and to an increase in the number of non-permanent residents and immigrants (see Box 1) (Statistics Canada, 2012). Some provincial growth rates for this period were much higher than this national average. For example, that in Alberta was 10.8%, which probably reflects (although data have not yet been published) a higher level of ethnocultural diversity.
During the first 70 years of the twentieth century the majority of immigrants were of European origin. The 1980s signalled a turning point, with more people arriving from Asia and the Middle East, followed by Europe, the Caribbean and Central America, Africa, the USA, Oceania and other countries (Statistics Canada, 2008). Since 1999, Canada has admitted approximately 250 000 immigrants (including refugees) per year. In 2008, the top source countries were China, India, the Philippines, the USA and the UK (Citizenship and Immigration Canada, 2009). Specific to refugees, the top source countries in recent years include Hungary, China, Colombia, Pakistan, Namibia, Nigeria, St Vincent, Sri Lanka and India (Human Rights Research and Education Centre, 2012). Indeed, a report of population projections from Statistics Canada predicts that members of visible minority groups will represent between 29%and 32% of Canada’s population in 2031 (Statistics Canada, 2010).
Box 1: Definition of terms
In a country founded upon a dual-language system, and where approximately 47% of the population have ethnic origins other than British, French or Canadian, immigration in official policy may be seen as a mechanism for developing and enhancing national identity and prosperity (Kymlicka, 2003). Canada has often been considered to be an exemplar of multiculturalism, with policies that require public institutions to reflect diversity and reduce barriers to immigrant inclusion tending to receive broad public support (Kymlicka, 2003). In recognition of the growing needs of recent immigrant groups, some provincial governments have formulated immigration support policy frameworks in order to facilitate resettlement, including ‘resolving personal health issues in a system with which they are unfamiliar’ (Alberta Government, 2005, p. 6). However, the relationship between immigration and health transitions is highly complex, involving not only socioeconomic, cultural, behavioural, environmental and biological factors, but also pre-immigration history (Hyman, 2001).
Maternity care services in Canada
In Canada, compliance with the Canada Health Act is required by provinces to receive federal transfer payments, but constitutional division of regulatory powers among levels of government creates considerable diversity in the constellation of maternity services. The majority of prenatal care (88%) and deliveries (98%) are undertaken by family physicians and obstetricians in clinic and hospital settings. Midwives provide only 3% and 2.5% of prenatal and hospital delivery care, respectively (Canadian Institute for Health Information, 2004). Midwifery as a separate profession is fairly new; regulation was first introduced in Ontario in 1992, and currently nine of the 13 provinces and territories regulate and only six have provincial and territorial health plans that fund midwifery (Canadian Midwifery Regulators Consortium, 2012). In some areas, care may also be available from doulas, who may be qualified immigrant midwives who are not registered to practise in Canada (Meddings and Haith-Cooper, 2008; Reitmanova and Gustafson, 2008). Apart from healthcare providers, another factor that characterises maternity care in Canada is the short length of postpartum hospital stay, namely 2 days for vaginal deliveries and 4 days for Caesarean section deliveries. This length of stay is similar to that in the USA and the UK, but considerably shorter than that in other countries, such as France and Germany (Canadian Institute for Health Information, 2004).
Inequity in healthcare access and health for immigrant women
There is conflicting evidence about whether immigrant communities under- or over-utilise health services (Wang et al, 2008). Women generally may have more frequent contact than men with health services (Gagnon et al, 2009). However, language barriers, difficulties with understanding healthcare information, experiences of discrimination, and challenges in navigating the Canadian healthcare system may deter immigrants (Brar et al, 2009; Edge and Newbold, 2012; Grewal et al, 2008; Hyman, 2001). Although the design and delivery of services can undoubtedly play a key role, other important factors include wider socioeconomic, political and cultural processes, such as material disadvantage, spousal dependence, geography, racial harassment, and exclusion (Bhopal, 2009; Heaman et al, 2007; O’Mahony and Donnelly, 2012; Napoles-Springer et al, 2005). Using federal policy as a framework for assessing healthcare access for immigrant women, Oxman-Martinez et al (2005) suggest the primacy of intersectionality, that is, the multiple ways in which different axes of inequality coalesce with regard to strategic policy directorates and sociocultural factors to undermine equitable access to health for women with precarious immigrant status who are living in Canada.
Health inequities among immigrants may partly relate to the often compromised health status of refugees at the point of arrival and related factors, which include the stress of relocation (which can erode health advantage), distrust of western medicine, a preference for traditional healthcare providers, and pre-migration experiences (Hyman, 2007). Even when immigrants are healthy on arrival, their health declines as their length of stay in Canada increases (Hyman, 2007; Newbold, 2005). Facilitating the provision of appropriate healthcare for immigrant populations in Canada is therefore critical for maximising health potential and well-being. Without culturally appropriate and culturally safe healthcare delivery, a negative trajectory of events may occur, with particularly high risks during pregnancy (Reitmanova and Gustafson, 2008; Grewal et al, 2008). One way of avoiding this is to listen to the experiences of immigrant women and respond with appropriate strategies.
Objective
The aim of this integrative review was to identify and descriptively synthesise current empirical literature on immigrants’ experiences of maternity healthcare services in Canada, to outline practice implications and/ or to offer recommendations for future research.
Methods
A comprehensive review of both qualitative and quantitative literature related to immigrant women’s maternal experiences in Canada was undertaken. The review drew upon established integrative review methodology (Russell, 2005).
Search strategy
A comprehensive search strategy was developed, in consultation with an information scientist, for key electronic bibliographic databases covering immigrant and maternal health literature, namely CINAHL, MEDline, Cochrane, Scopus and Web of Science. The reference lists of key papers were checked for add itional sources, and citation searches were conducted on key authors. The emphasis was on searching Canadian literature as it pertained to immigrant women and their maternal health experiences in Canada. The database searches used Boolean logic [AND and OR] to combine different search terms together. Truncations [$ or *] were also used to expand the search from root forms of the search words as needed.
Since this review aimed to map the state of current knowledge rather than to answer a specific research question, controlled vocabulary and keyword terms for immigrant women and maternal health were used, rather than adopting rigid inclusion criteria. The words migrant, refugee, emigration, immigration, transient were used to capture immigrant women, and pregnancy, birth, labour, maternal, maternal–child, sexual, women’s, reproductive health were used for maternity services. Letters, editorials, commentaries and review papers were excluded. The review only included publications in English, due to the lack of availability of a translator for papers in French. Two people independently screened the citations (abstracts) for potential inclusion using the following criteria:
1. article was published between January 2000 and March 2010
2. article described empirical research, including systematic review
3. article described a sample living in Canada or studies completed in Canada
4. article appeared to focus on maternal health services or outcomes for immigrants.
The final selection of papers for inclusion was determined by full article review and agreement by the same two reviewers.
Quality assessment
The checklists developed by the Critical Appraisal Skills Programme (www.phru.nhs.uk/pages/PHD/ CASP. htm) were used to assess the methodological quality of the included articles and to gain an understanding of the relative strengths and weaknesses of the body of evidence. No studies were excluded on the basis of quality alone.
Data storage and extraction, and thematic analysis
Articles were stored in RefWorks (Bethesda, Maryland, USA), a web-based citation management programme. Information about the aim, sampling, methodology and findings of each study was extracted from RefWorks into a table using Microsoft Word (abbreviated version in Table 1 which is available online at www.radcliffehealth.com/shop/diversity-and-equality-in-health-and-care. After thematic analysis, the findings from all papers were grouped into themes for summary, integration and discussion.
Results
The database searches resulted in 1491 hits, and two articles were located from additional searches of the reference lists. After duplicates had been removed, 253 abstracts were screened for eligibility and 71 full articles were read, of which 30 were retained (see Figure 1). Primary reasons for exclusion from full article review were immigrant health articles that did not have a maternal health focus, maternal and reproductive health articles that did not focus on immigrant women, and non-empirical basis. The study findings were grouped into six themes as follows:
• barriers to accessing healthcare
ethnoculturally determined perinatal customs and support
• breastfeeding support and experiences
• environmental factors
• postpartum care and mental health
• pregnancy and birth outcomes.
Barriers in access to healthcare
Studies have examined immigrants’ access to health services generally, but issues relating to maternal health services have not been examined thoroughly.
Multiple factors are associated with immigrants’ difficulties in accessing immediate and routine firstcontact healthcare services. The 2003 Health Services Access Survey, whichwas conducted by StatisticsCanada as part of the cross-sectional Canadian Community Health Survey and represented 98% of the Canadian residential population over 15 years of age, revealed that 15% of recent immigrants surveyed reported difficulty in accessing routine care, while 23% claimed to have difficulty accessing immediate care (Sanmartin and Ross, 2006). However, a major critique of the survey’s methodological approach is that it is based on the need for fluency in English or French. Consequently, the survey may have excluded some immigrants and the perspectives of highly marginalised individuals. Physician and/or service availability (54.0%), long wait times (43.3%), and personal reasons (3.2%) were cited as hindering immigrants’ access to healthcare services. Personal reasons included lack of transport, language, information and finance. Women reported significantly more difficulties than men (OR, 1.38; P<0.05); 17.0% of women reported difficulties accessing routine care, compared with 14.3% of men, and 26.3% of women encountered trouble with access to immediate care, compared with 21.9% of men. Women’s economic and emotional dependence on spouses and their lack of other sources of social support may be additional factors (O’Mahony and Donnelly, 2012;Ng et al, 2011). The strong association with language skills also intersects here, as women may have less proficiency in English or French if they are not the main wage earner in the family (Redwood- Campbell et al, 2008).
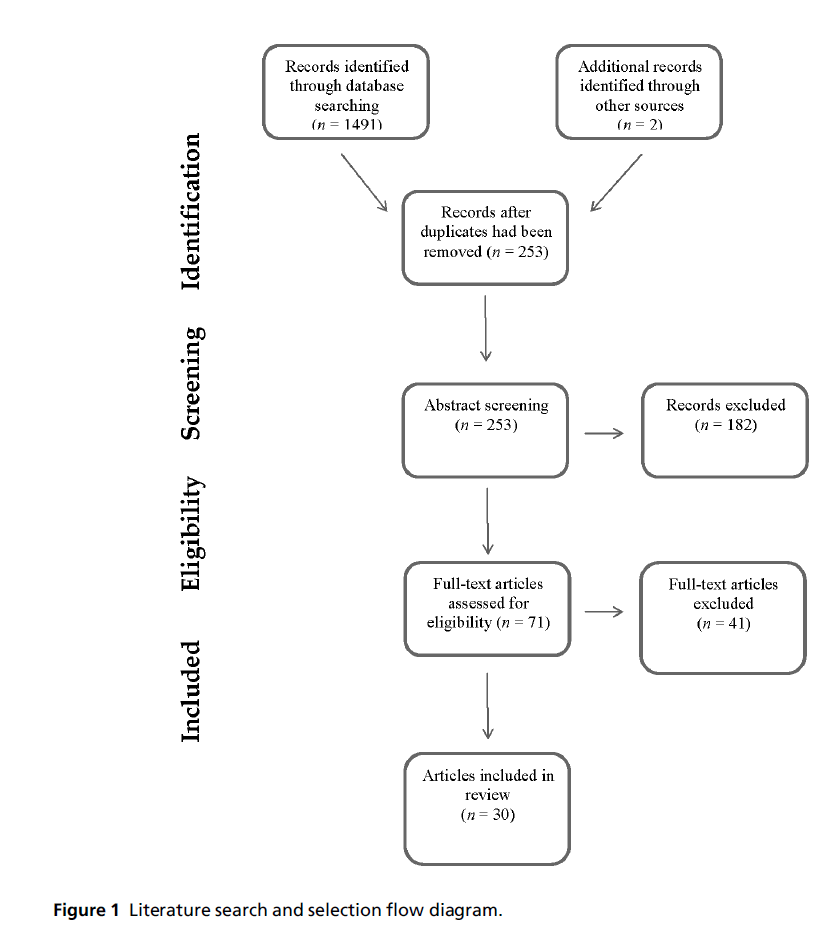
Figure 1: Literature search and selection flow diagram.
In terms of access to routine services, immigrants were identified as being an at-risk group generally (Sanmartin and Ross, 2006). Those who had lived in Canada for less than 5 years were 2.5 times more likely than Canadian-born people to experience difficulties in accessing care, but there were no differences between the two groups in terms of accessing immediate care. Overall, new immigrants reported personal barriers at a rate tenfold higher than that of their Canadian-born counterparts (Sanmartin and Ross, 2006). These findings appear to concur with the notion of the healthy immigrant effect, which suggests that, on arrival, immigrants are healthier than their Canadian-born counterparts but that, over time (approximately 10 years), their health declines towards the national average (Hyman, 2007; Newbold, 2005). Difficulties in accessing and navigating health services, including maternity care, may be contributory factors.
A few small-scale studies have looked at maternity care. For example, Brar et al (2009) conducted telephone surveys with 30 South Asian immigrantwomen and 30 Canadian-born women (of any ethnicity) who delivered at a major hospital in Calgary, Alberta. Most of the women were satisfied with the medical care that they received while they were pregnant (93% and 97%, respectively) and during the birth of their child (97% and 87%, respectively). The satisfaction of the South Asian immigrant women may have been influenced by the fact that, generally speaking, more services are available in Canada than in India. In other words, immigrant women may have lower expectations due to their previous experiences or knowledge. Their stated satisfaction may also be due to fear arising from lack of familiarity with the rights and obligations afforded by the norms and values of Canadian society.
Language (both written and spoken) was the most prevalent barrier to perinatal care in the study by Brar et al (2009). More immigrant than Canadian-born women reported language barriers to receiving medical care during pregnancy, delivery and the postpartum period (43% vs. 0% for during pregnancy and delivery; P < 0.001). In addition, some women were given written material in English which they could not read, and others were given material published in their native spoken language even though they were illiterate in their mother tongue. This finding suggests that other mechanisms and more innovative forms of communication that move beyond the written word may be required. Although the respective provincial health authority provides translation services, these services were said to be underutilised by all ethnicities except for Cantonese-speaking immigrants. Family members were often used as interpreters throughout the province. However, evidence suggests that this may not be ideal, as the family member may deliver their own version of the intended message, and thus important information may be lost in translation (Bowen, 2001). In Sweden there is legislation about the provision of interpreting services, but this is not the case in Canada. The lack of a Canadian national interpretation strategy may in part be related to the devolved provincial healthcare legislation and provision, which means that healthcare in each province is uniquely configured. However, even where interpreting services are provided, they are not readily available or easily accessible outside acute-care hospital settings (Brar et al, 2009). The main conclusion from this small study was that language barriers may be overcome by wider availability of multilingual staff and provision of educational materials in written as well as other formats, including illustrated books and videos.
These findings with regard to language and communication difficulties are consistent with the results of other studies relating to immigrant women’s healthcare (Newbold andWillinsky, 2009;Redwood-Campbell et al, 2008; Reitmanova and Gustafson, 2008). One possible contributor, noted by Redwood-Campbell et al (2008) when reporting on a self-administered survey completed by 85 refugee Kosovar women about women’s health issues and experiences of health services, is that often English-as-a-second-language (ESL) classes were not a priority for the women; in general, men attended these classes while the women opted to stay at home. Patriarchal relationships may have a role in the attendance of women at antenatal class, and we have found some evidence for this in an ongoing study (Higginbottom et al, 2011). Moreover, access to professional translators and/or multilingual staff who speak a woman’s primary language is inconsistent and often non-existent (Brar et al, 2009;Newbold and Willinsky, 2009; Redwood-Campbell et al, 2008). Professional interpretation, especially for complex and detailed information, such as family planning or explanation of group B streptococcus testing, was valued by healthcare providers, even when patients and their families had some command of English, in order to maximise understanding. In Canada, service providers are not obliged to take non-English-speaking patients on to their caseloads. Finding clinics that are willing to see non-English-speaking clients can be a challenge (Newbold and Willinsky, 2009). Urban clinics in high-density immigrant areas are more likely to accept such patients than are clinics in small towns (Newbold and Willinsky, 2009; Redwood-Campbell et al, 2008; Reitmanova and Gustafson, 2008).
Additional barriers to accessing perinatal healthcare services include physician gender and systemic institutional issues (Brar et al, 2009; Reitmanova and Gustafson, 2008; Newbold and Willinsky, 2009).Gender preference for healthcare providers and translators created tensions and challenges for some immigrant women (Brar et al, 2009; Reitmanova and Gustafson, 2008; Redwood-Campbell et al, 2008). Brar et al (2009) noted that there was a significant preference for female physicians among South Asian immigrant women compared with Canadian-born women (P < 0.001), and the reasons cited included modesty and/or religion. Preferences for female doctors were also voiced strongly by the immigrant Muslimwomen (n=6)who were interviewed in a qualitative study by Reitmanova and Gustafson (2008). Major systemic institutional issues include physician availability and appointment waiting times, especially at clinics that specialise in immigrant care. According to a qualitative exploratory study of healthcare professionals (n = 6), immigrant women had to wait for 8 weeks to discuss family planning with a physician, compared with 4 to 6 weeks at other centres that did not provide medical care specifically targeted to immigrants (Newbold and Willinsky, 2009). The reasons for this are unclear, but institutional racism could play a role in this delayed access to treatment. However, waiting times for obstetric services can be long for any woman living in Canada, and there has been a consistent reduction in the number of family physicians who provide maternity care services (Canadian Institute for Health Information, 2004).
Kreiner (2009) highlights the need for midwifery services in Manitoba, Canada to address the national challenges within the public maternity care system. One of the priorities outlined in this qualitative embedded case study, with data collected from five stakeholder groups, was to provide and assess a service for women and families who are inadequately served by the current maternity care services, including those of varying socioeconomic status, age, language and culture. The authors discuss the Midwifery Implementation Council communications testing and language upgrading programme. This is a bridging programme to encourage immigrants with midwifery qualifications to become registered. It enabled 11 immigrant midwives to register, so that more immigrant women could access culturally sensitive and responsive care in their first language.
Using cross-sectional survey data from 1250 immigrant and Canadian-born women, Sword et al (2006) examined their access to services and their learning and support needs during the early postpartum period. They found that immigrant women received less social support, had unmet postpartum learning needs, and experienced overall lower self-reported health at 4 weeks postpartum. Reduced access to social support is not surprising given the relocation to a new ethnocultural context and the dislocation from extended family members; many immigrant women in Canada are members of transnational families spanning several continents. Therewas no difference between immigrant and Canadian-born women in their ability to access care for physical or emotional health, or help with breastfeeding. In fact immigrant women were significantly more likely to seek services from an obstetrician or public healthcare provider. However, in hospital, more immigrant than Canadian-born women (76% vs. 56.3%) reported having unmet learning needs.
Immigrant Muslim women’s (n = 6) service and support needs were unmet throughout their pregnancy and postpartum period (Reitmanova and Gustafson, 2008). In-depth interviews revealed that although the need for emotional support and help is common to all new mothers, this need may be more acute for immigrants, who experience a greater degree of loneliness and isolation. These authors suggest that a diversity-responsive healthcare system would have formal and/or informal buddy mechanisms to ensure that the women are informed about the available services, and possibly to provide direct support.
Katz and Gagnon (2002) have speculated that various factors, including culturally responsive care, communication and literacy, may prevent immigrant women from receiving postpartum community care. Their pilot study of hospital and community chart reviews (n = 22) revealed a paucity of health record data to support adequate care for specific health and social concerns identified among immigrant women. They found that 40–100% of problems were not recorded as having been resolved and 30–100% of families were not recorded as receiving optimal care. Even when health and social concerns were identified, there were significant disparities in the quality of care in both hospital and community maternity services, which may have increased the risk of postpartum complications. For instance, one woman who presented with breastfeeding difficulties developed a breast abscess 1 month postpartum, and a visit to the Emergency Department and follow-up wound care was required to treat abscess-related sequelae (Katz and Gagnon, 2002).
Ethnoculturally determined perinatal customs and support
Grewal et al (2008) conducted a qualitative descriptive study and asked women who had emigrated to Canada from Indiawithin the previous 5 years to describe their perinatal experiences in a Canadian healthcare setting. This study revealed the importance of traditional Punjabi beliefs and practices associated with the perinatal period. The social expectations of getting married and becoming pregnant are validated when the women share the news of pregnancy with their families. This news is often followed by advice regarding diet, lifestyle and rituals, most often from female elders. Although the participants in this study were encouraged by their healthcare provider to attend prenatal classes, only one out of 15 women did so. This was due in part to the belief that their female family members would be able to provide them with the information necessary to endure a safe and health pregnancy, labour and delivery. However, the women were also discouraged from attending the classes by feeling too tired, lack of transport and language barriers. Moving to Canada had brought changes in the rituals traditionally followed in Punjabi culture in that the practice of baby showers had been adopted. This is not surprising, as acculturation is bound to have an impact on adherence to traditional practices; as immigrant women become integrated into Canadian society, ethnocultural practices may fuse, resulting in a degree of hybridity. Consistent with these findings are the results of an ethnographic qualitative study in which professional Chinese Canadian women described a decline after immigration in their adherence to many of their traditional beliefs and rituals (Brathwaite and Williams, 2004).
Grewal et al (2008) also noted the importance of involving the family, and reported that, in Punjabi culture, various family members are assigned specific roles relating to the pregnant woman. In the Canadian setting, husbands have taken on a more active role in their wife’s pregnancy, often providing transport to prenatal visits and acting as interpreters during the consultation. This active role also included attendance in the delivery room and the provision of emotional and physical support during active labour, which may indicate changing conjugal roles. The women’s expectations during the immediate postpartum period were not consistent with what some of them actually experienced. Whereas their traditional cultural practices led to expectations that their babies would be fully cared for (by family members), allowing them to rest, the reality of immediately taking on the care of their child resulted in feelings of abandonment.
One study reported positive interactions with healthcare providers in the Canadian healthcare system (Grewal et al, 2008). Physicians were seen as the most important professionals during pregnancy, whereas obstetric nurses were perceived as most important during labour and delivery, and reduced the women’s feelings of anxiety and fear. However, the women also felt that their pain and fatigue were not validated by the nursing staff during the immediate postpartum period (Grewal et al, 2008). Chinese Canadian women also reported incongruence between their values and expectations and those of the Canadian healthcare system (Brathwaite and Williams, 2004). These participants did not support medical intervention during labour and delivery, and specifically expressed a desire to avoid using technology or pain medication during this time. Moreover, the Chinese women expressed a preference for their babies to be delivered by female physicians (Brathwaite and Williams, 2004).
Many of these findings also applied to Somali women who had given birth in Canada after earlier female genital mutilation. In their survey study of 432 Somali women, Chalmers and Hashi (2000) found that, for many women, their expectations about labour and delivery were not met in Canada. Less than 1% of the women wanted a Caesarean section, yet 50% of them underwent this procedure. However, it is not clear from this paper whether this was due to the woman’s female genital mutilation or the inability of the physicians to undertake de-infibulation, or both. Many women would have preferred much less intervention during their delivery, yet they reported having little say in or discussion about their treatment during labour and delivery. They reported doctors’ apparent surprise (in 75% of cases) or disgust (55%), and hurtful comments (87%) made by caregivers. Many felt that they were handled roughly and that their privacy was not respected during procedures. Lack of cultural sensitivity was also evident from the descriptions of obstetric nurses who were perceived as believing that the women were ‘lazy’ (85%) or reluctant to cooperate (80%). Traditional customs whereby women are present as supporters during labour were often not possible, and many of the women reported feeling pressured to have their spouses present.
Finally, specialised social support has been shown to be of great value for minority women (in a metropolitan city with a high immigrant population) while their newborns are intensive care. In a study that evaluated a culturally sensitive individual peer support intervention for mothers with preterm infants using self-reported indices of maternal ratings, Preyde (2007) found that mothers who received peer support from a trained volunteer, matched for language, ethnicity and culture, felt more confident in their parenting, better understood the medical condition of their child, experienced better quality of support, and were able to share their experience. Having a pool of buddies would help to meet the needs of the highly diverse populations in many Canadian cities. This echoes the discussion by Reitmanova and Gustafson (2008) of their smaller city setting with limited yet increasing diversity.
Although this social support appears promising, the new economy of care may hinder progress. It has already influenced obstetric nurses’ ability to provide much needed culturally competent care, and many visible minority patients may be left feeling invisible (Spitzer, 2004). In her qualitative study employing interviews of visible minority women from diverse ethnocultural groups and nurses, Spitzer found that obstetric nurses:
felt compelled to avoid interactions with patients deemed too costly in terms of time. Overwhelmingly, these patients were members of culturally marginalised populations whose bodies were read by nurses as potentially problematic and time consuming. As their calls for assistance go unanswered, visible minority women complained of feeling invisible. Taken in context of historical and contemporary interethnic relations, these women regarded such avoidance patterns as evidence of racism.
(Spitzer, 2004, p. 490)
Breastfeeding support and experiences
Loiselle et al (2001) explored perceptions of breastfeeding information and support among 108 firsttime mothers in an ethnically diverse community using a telephone survey. Even though immigrant mothers found professional support for their breastfeeding practices generally positive, there were some significant differences compared with Canadian-born women. Canadian-born mothers agreed more strongly than immigrant women that community care nurses valued breastfeeding (P = 0.007), that there was sufficient breastfeeding support available when it was needed (P = 0.023), and that they felt comfortable asking providers for breastfeeding assistance (P = 0.01).
There were differences in the uptake of community care nurses and other identified sources of breastfeeding information. Of the mothers who received postpartum follow-up services (n = 90), immigrant mothers were more likely to be directly assisted by a community care nurse (P = 0.004), whereas their Canadian-born counterparts were more likely to be provided with information about breastfeeding support groups or breastfeeding specialists (P = 0.005), and/or to utilise pamphlets or information sheets (P = 0.006) and the Internet (P = 0.007). Immigrant mothers more often valued professional information about the advantages of breastfeeding (33% of immigrant mothers vs. 10% of Canadian-born mothers), whereas Canadian-born mothers placed higher value on breastfeeding positioning (40% of Canadian-born women vs. 19% of immigrant mothers) (Loiselle et al, 2001). In both groups, mothers relied on informal sources of information such as friends or colleagues (63%) and family members (56%), rather than obstetricians or family physicians (33%) and paediatricians (43%).
Groleau et al (2006) conducted a qualitative study informed by interpretive and critical approaches from medical anthropology, to provide focused insights into the impact of the social and spatial organisation of cultural practices on breastfeeding among Vietnamese immigrant women (n = 19). None of the women breastfed exclusively, and those who did breastfeed (5 of 19, all of whom weremultiparous) only did so for an average duration of 2.2 months (Groleau et al, 2006). Decisions to bottle-feed revolved around the constraints of their lives in Canada, which hindered traditional postnatal rituals, dietary regimes and social support from older women. Multiparous women understood that breast milk was of superior quality to commercial formula, but they felt that they could not produce fresh breast milk in their Canadian environment. Primiparous women talked of considerable distress related to the absence of their mothers and childbirth support. They complained of fatigue, loss of appetite, health problems and sadness that they tried to hide from family members. Multiparous motherswho breastfed were better educated, assertive, critical thinkers and perhaps more independent, which may have had a protective effect.
Environmental factors
Associations between birth outcomes and socioeconomic indicators such as level of education, employment, income and neighbourhood have been shown to be modified by maternal birthplace or immigrant status. For example, when analysing crosssectional survey data using stratification based on income, social support and a universally administered hospital postpartum risk screen, Kurtz Landy et al (2008) found that socioeconomically disadvantaged (SED) women had a lower level of education and were more likely to be born outside Canada, to have a partner, to use English as the main language at home or to describe their ethnicity as Canadian. Maternal outcomes of SED women were noted at 4 weeks post discharge; they were significantly less likely to report health as very good or excellent (OR, 0.48; 95% CI, 0.35–0.67) and more likely to experience symptoms of postpartum depression compared with more advantaged women (OR, 2.7; 95% CI, 1.64–4.4). SED women were less likely than advantaged women to receive the mandatory phone call from the public health nurse within 48 hours of discharge (OR, 0.31; 95% CI, 0.13– 0.77) and were more likely to have continued involvementwith a public health nurse 4weeks post discharge (OR, 2.5; 95% CI, 1.49–4.21). SED immigrant women had lived in Canada for a shorter time period than advantaged women, which may reflect resettlement challenges such as social isolation, financial hardships and maternity leave issues.
The findings of Auger et al (2009) relating birth outcome measures of small for gestational age (SGA) and preterm birth (PTB) to area characteristics, such as income, immigrant density and income inequality, show a complex distribution pattern. Linking Montreal live births during 1999–2003 (n = 353 120) using the Quebec Birth File to 2001 census data, there was a positive relationship in the unadjusted models with PTB and immigrant density amongst foreign-born mothers (P = 0.0002), as well as SGA in foreign-born mothers on all three social markers, namely area income (P = 0.0009), immigrant density (P = 0.0006) and income inequality (P = 0.008). Stratified analyses indicated that area poverty was associated with PTB (OR, 1.07; 95% CI, 1.00–1.140) and SGA (OR, 1.13; 95% CI, 1.06–1.20) birth among Canadian-born mothers but not foreign-born mothers, possibly reflecting the healthy, resilient nature of foreign-born women as a result of the selective immigration process compared with less favourable health-related behaviours among socioeconomically vulnerable Canadianborn women (Auger et al, 2009). In a previous study, Auger et al (2008) found that SGA rates were lower (7.8%) where the neighbourhood security perception index (NPI) was most favourable, and higher (10.5%) where the NPI was least favourable and where immigrant proportions were highest (10.5%). The NPI data were taken from a random-digit telephone survey conducted with 14 132 Montreal residents.
Postpartum care and mental health
Several research studies contained findings pertaining to postpartum depression/mental health that encompassed the views of both healthcare providers and women. Stewart et al (2008) and Mechakra-Tahiri et al (2007) found a higher prevalence of postpartumdepressive symptoms among immigrant women compared with Canadian-born women. Using questionnaires about depression, social support, interpersonal violence and demographic information, newcomer women (immigrant, 35.1%; asylum seekers, 31.1%; refugees, 25.7%) sampled from three Canadian cities were significantly more likely to score � 10 (P = 0.008) on the Edinburgh Postnatal Depression Scale (EPDS) than Canadian-born women (Stewart et al, 2008). Scores of � 10 on the EPDS were almost five times more common among refugees compared with Canadian-born women (OR, 4.80; 95% CI, 1.57– 14.69), almost four times more common for immigrant women (OR, 4.58; 95% CI, 1.61–13.02) and three times more common for asylum seekers (OR, 3.06; 95% CI, 1.06–8.82). Visible minority status was also shown to be associated with increased risk of an EPDS score of ≥ 10, although this did not reach the level of statistical significance (Stewart et al, 2008).
In Quebec, Mechakra-Tahiri et al (2007) also found higher levels of depressive symptoms among immigrant mothers compared with Canadian-born mothers. Baseline health record and questionnaire data from this large cohort study showed a higher prevalence of depressive symptoms among immigrants from minority groups (24.7%) compared with immigrants from majority groups (8.3%) and Canadian-born mothers (11.2%). Self-rated health was strongly associated with depressive symptoms in Canadian-born mothers (OR, 3.46; 95%, CI 2.54–4.72) but not in minority immigrant mothers, suggesting the influence of other factors.
When developing amultifactorial predictive model of depressive symptomatology at 1 week postpartum (n = 594), Dennis et al (2004) found that the first 5- year period after immigration was a significant sociodemographic predictor (OR, 4.94; 95% CI, 0.99–24.8) of maternal mental health. Although recent immigration can be considered a significant stressor, further research is warranted to examine the interplay between postpartum depressive symptomatology and traditional postpartum customs. When assessing the mental health of 45 women at the first postnatal visit, Minde et al (2001) found that women who were recent immigrants were over-represented among those who were insecurely attached to their infants (8 of the 9 mothers in this subgroup). These authors acknowledge that their Working Model of the Child Interview (WMCI) may be culturally biased, as it is based on respondents’ verbal responses to questions that may not be acceptable to mothers from non-western cultures (i.e. a mother’s reluctance to share her inner thoughts about her infant may place her in an insecure attachment category of the WMCI).
The reasons for depressive symptoms among immigrant women are multiple. Two qualitative studies delved into the experiences of postpartum depression from the viewpoint of immigrant women. Ahmed et al (2008) found that ethnically diverse women with less than 5 years of residency attributed their depressive symptoms to social isolation, physical changes, feeling overwhelmed in a new environment, and financial problems. Morrow et al (2008) revealed some nuanced information from their first-generation Punjabi-, Cantonese-, and Mandarin-speaking participants in Vancouver, British Columbia. Those who most often spoke out about psychosocial stressors were from mainland China; their socioeconomic status was lower than that of the South Asian and Hong Kong women. Lack of an established social network, job deskilling, a lack of stable housing and financial difficulties were all mentioned. The type of family presence made a difference for immigrant women who were experiencing depressive symptoms. In-law support is not necessarily equivalent to immediate familial support; women felt more comfortable asking their own mothers. They indicated that mothers-in-law tended to focus their attention on their son and the baby; their loyalty was to their husband’s family.
From the viewpoint of professionals, practical barriers to care for immigrant women with postpartum depression included lack of fluency in English, lack of understanding of a new healthcare system, a complex referral process, difficulty in working with interpreters when trying to assess sensitive information, transport difficulties and childcare problems (Teng et al, 2007). Culturally determined barriers to care included lack of knowledge and understanding about postpartum depression, stigma associated with depression and mental illness (particularly if this extended to other female members of the family), the patriarchal structure of extended families and tension in the relationship with mothers-in-law. Immigrant women’s reluctance to disclose depressive symptoms was felt to be related to a fear of losing their baby to child welfare services, compounded by the women’s lack of understanding of health and social services systems. Professionals also reflected on challenges in their practice which had an impact on the quality of care. Fear of incompetence, language barriers, culturally inadequate assessment tools, and uncertainties about cultural differences were some of the limitations and social/cultural barriers reported.
Pregnancy and birth outcomes
Maternal characteristics, including migration history, number of years for which the woman had lived in Canada, and acculturation, predict both positive and negative maternal experiences, including pregnancy and birth outcomes. Preliminary studies indicate that infant mortality and low birth weight (LBW) are less likely in infants born to immigrants; ‘however, data on obstetric outcomes are lacking’ (Ray et al, 2007, p. 1419). The findings of Urquia et al (2007) partly support this suggestion. In their study examining associations between non-fatal birth outcomes, neighbourhood income and recent immigration status using hospital discharge records, the good birth outcomes of recent immigrants appeared to partly mask the deleterious effects of neighbourhood income.
Maternal placental syndrome, that is, ‘a diagnosis of pre-eclampsia or eclampsia ... placental abruption or placental infarction during the index admission for obstetric delivery’ (Ray et al, 2007, p. 1420), was the primary outcome examined in a population-based retrospective cohort study (n = 796 105) in Ontario, which is Canada’s most populated province. Women (n = 5920) who had arrived in Canada less than 3 months prior to delivery displayed the lowest risk of placental disorders (3.8%). The risk increased with length of residence in Canada, such that those who had lived in Canada for at least 5 years had a risk of 6.0%. The gradient was limited to those women who were living in urban areas.
In a qualitative study examining health behaviours, social support and stress in pregnant South-East Asian immigrant women with varying degrees of acculturation, this last factor was found to have negative consequences for this population (Hyman and Dussault, 2000). None of the women used alcohol or smoked before or during pregnancy. They reported diets similar to those that they followed in their home countries, but observed Canadian women to be more preoccupied with being thin, even during pregnancy. Stress during pregnancy was also investigated. It was found that the more acculturated the women were, the more likely they were to reveal that they were dealing with stress. Financial pressures were the most frequently cited sources of stress. The women felt that, as South-East Asian women living in Canada, they were obliged to continue to work in strenuous jobs during pregnancy. Social support was noted as the second most frequently cited source of stress, with immigrant women reporting that they had few people with whom to share their problems. They worried about not having enough assistance at home after the baby was born.
In a meta-analysis of routinely collected data in a national and regional perinatal data set, pregnancy outcomes in Somali-born women post-migration were compared with those of women from six other receiving countries, namely Australia, Belgium, Canada, Finland, Norway and Sweden (Small et al, 2008). Somali women gave no cause for concern, as they were significantly less likely to give birth to preterm infants (OR, 0.72; 95% CI, 0.64–0.81) or to have LBW babies (OR, 0.89; 95% CI, 0.82–0.98). Caesarean sections were more common, especially with first births (OR, 1.41; 95% CI, 1.25–1.59), as were stillbirths among Somali-born women (OR, 1.86; 95% CI, 1.38–2.51). The pooled odds for neonatal deaths showed no significant difference.
Discussion
Our findings indicate that new immigrants are ten times more likely than their Canadian-born counterparts to experience personal barriers when accessing healthcare. Language is a particular problem for many new immigrants, and current interpreting services are either underutilised or unavailable. More multilingual staff and provision of educational materials in written as well as other formats, including illustrated books and videos, might help to overcome this problem, particularly in hospital settings (Brar et al, 2009; Sword et al, 2006).
Many immigrants did report positive experiences (Grewal et al, 2008; Brar et al, 2009), but others reported many unmet needs, and discriminatory and degrading experiences (Reitmanova and Gustafson, 2008; Chalmers and Hashi, 2000). Health record data identifying the extent to which health and social needs are met suggest that, for immigrant women, there are significant disparities in quality of care in both hospital and community maternity services (Katz and Gagnon, 2002).
Lack of social support and separation from the family network were important stressors for women, given their new environmental context. Diversityresponsive healthcare systems may benefit from having formal and/or informal ‘buddy’ mechanisms to ensure that women are informed of the available services and offered direct support (Reitmanova and Gustafson, 2008). Culturally sensitive individual peersupport interventions (Preyde, 2007) seem to have promise, if they prove to be feasible in this era of economy of care (Spitzer, 2004). Professionals attributed the most important barriers to care to a combination of cultural and practice-related factors, including lack of knowledge and understanding of postpartum depression among immigrants, as well as their own limitations, which were largely due to lack of resources. Culturally competent care provision requires that professionals receive education and resources, including appropriate professional interpreting services.
Caution is necessary not to impose western concepts about maternal health, particularly mental health, across diverse ethnocultural backgrounds. The challenge for service providers is to explore descriptions of health phenomena given by patients. Programme and service development should be shaped through collaborative interactions with service users and move away from the tendency to stereotype ethnocultural groups with regard to their beliefs and practices. Adherence to traditional beliefs and rituals declines over time. Family roles during maternity may also change as husbands take a more active role in helping and supporting their wives during pregnancy and delivery (Grewal et al, 2008; Brathwaite andWilliams, 2003). This change in roles may sometimes be perceived as forced and undesirable, as was the case for many of the Somali women (Chalmers and Hashi, 2000).
Although immigrants’ access to health services in general has been studied, access to maternal health services by immigrant women has not been examined thoroughly. Further research is needed to address language and literacy difficulties in order to create optimal standards for provision of interpreter services in all settings. Mechanisms to enhance social care, including emotional support for immigrants during pregnancy and after childbirth, should be supported by further intersectoral research collaborations, which include examination of how funds can be allocated adequately and appropriately to meet these unmet needs. Further research is also warranted in relation to the interplay between postpartum depressive symptomatology and traditional postpartum customs. All areas of research need to reach both urban and rural communities.
Limitations of the study
This study has some limitations. Although the scope of the database search strategy was comprehensive, we only searched back to 2000 and for publications in English, due to time and resource constraints. We did not search the grey literature, which could provide additional insight into the phenomenon, particularly from a policy-making perspective. Producers of grey literature report that policy makers are their primary targeted audience, and three of the most important topic areas are access to healthcare, maternal and child health, and minority health (AcademyHealth, 2006).
Conclusion
This integrative review revealed not only the difficulties experienced by immigrant women with regard to accessing health services, but also the potential reasons for these challenges, as well as real and disparate maternal–infant outcomes that may in part be attributed to access. The numbers of immigrant women seeking out maternal care and childbearing families have increased. If they cannot access and benefit from appropriate existing services, their health may suffer in both the short and long term, as may that of their families.
ACKNOWLEDGEMENTS
The first author (GH) holds a Canada Research Chair funded by the Canadian Institutes for Health Research, which also supports a portion of JP’s salary. Institutional support (Faculty of Nursing, University of Alberta) was provided for the salaries of AB and JA.
References
- Academy Health (2006) Health Services Research and Health Policy Grey Literature Project: summary report. www. nlm.nih.gov/nichsr/greylitreport_06.html (accessed 4 July 2012).
- Ahmed A, Stewart DE, Teng L et al (2008) Experiences of immigrant new mothers with symptoms of depression. Archives of Women’s Mental Health 11:295–303.
- Alberta Government (2005) Supporting Immigrants and Immigration to Alberta: an overview. https://employment. alberta.ca/documents/WIA/WIA-IM_framework_overview. pdf (accessed 4 July 2012).
- Auger N, Daniel M, Platt RW et al (2008) Association between perceivedsecurity of the neighbourhood and small-for-gestational-age birth. Paediatric and PerinatalEpidemiology 22:467–77.
- Auger N, Giruad J and Daniel M (2009) The joint influence of area income, incomeinequality, and immigrant density on adverse birth outcomes: a population-based study. BMC Public Health 9:237.
- Bhopal R (2009) Ethnicity, Race and Health in MulticulturalSocieties. Oxford: Oxford University Press.
- Bowen S (2001) LanguageBarriers in Access to Health Care. Ottawa, Ontario: Health Canada. www.hc-sc.gc.ca/hcssss/ alt_formats/hpb-dgps/pdf/pubs/2001-lang-acces/ 2001-lang-acces-eng.pdf (accessed 4 July 2012).
- Brar S, Tang S, Drummond N et al (2009) Perinatal care for South Asian immigrant women and women born in Canada: telephonesurveys of users. Journal of Obstetrics and Gynaecology Canada 31:708–16.
- Brathwaite AC and Williams CC (2004) Childbirthexperiences of professionalChinese Canadian women. Journal of Obstetric, Gynecologic and Neonatal Nursing 33:748–55.
- Canadian Council for Refugees (2010) Refugees and Immigrants: aglossary. https://ccrweb.ca/en/glossary (accessed 12 September 2012).
- Canadian Institute for Health Information (2004) Giving Birth in Canada: providers of maternity and infant care. Ottawa, Ontario: Canadian Institute for Health Information.
- Canadian MidwiferyRegulators Consortium (2012) Home page. www.cmrc-ccosf.ca/node/2 (accessed 12 October 2012).
- ChalmersB and Hashi KO (2000) Somali women’s birth experiences in Canada afterearlierfemalegenital mutilation. Birth 27:227–34.
- Citizenship and Immigration Canada (2009) Facts and Figures. Immigration overview: permanent and temporaryresidents 2008. www.cic.gc.ca/english/pdf/research-stats/ facts2008.pdf (accessed 15 September 2012).
- Dennis CE, Janssen PA and Singer J (2004) Identifying women at risk for postpartum depression in the immediate postpartum period. Acta PsychiatricaScandinavica 110:338–46.
- Edge S and Newbold B (2012) Discrimination and the health of immigrants and refugees: exploringCanada’sevidence base and directions for future research in newcomer receiving countries. Journal of Immigrant and Minority Health, online May 22.
- Gagnon AJ, Zimbeck M, Zeitlin J et al (2009) Migration to western industrialized countries and perinatal health: asystematicreview. Social Science and Medicine 69:934–46.
- Grewal SK, Bhagat R and Balneaves LG (2008) Perinatalbeliefs and practices of immigrant Punjabi women living in Canada. Journal of Obstetric, Gynecologic and Neonatal Nursing 37:290–300.
- Groleau D, Souliere M and Kirmayer LJ (2006) Breastfeeding and the cultural configuration of social space among Vietnamese immigrant women. Health and Place 12:516–26.
- Heaman M, Green C, Newburn-Cook C et al (2007) Social inequalities in use of prenatal care in Manitoba. Journal of Obstetrics and Gynaecology Canada 29: 806–16.
- Higginbottom GMA, O’Brien B, Mumtaz Z et al (2011) International migration and maternity: perspectives from interdisciplinary qualitative research. International Journal of Qualitative Methodology 10:537.
- Human Rights Research and Education Centre (2012) By the Numbers: refugeestatistics. Ottawa, Ontario: University of Ottawa. www.cdp-hrc.uottawa.ca/projects/refugee-forum/ projects/Statistics.php (accessed 11 October 2012).
- Hyman I (2001) Immigration and Health. WorkingPaper 01–05. Ottawa, Ontario: Health Canada.
- Hyman I (2007) Immigration and Health: reviewingevidence of the healthy immigrant effect in Canada. CERIS WorkingPaper # 55. Toronto, Ontario: Joint Centre of Excellence for Research on Immigration and Settlement. https:// ceris.metropolis.net/wp-content/uploads/pdf/research_ publication/working_papers/wp55.pdf (accessed 4 July 2012).
- Hyman I and Dussault G (2000) Negativeconsequences of acculturation on health behaviour, social support and stress among pregnantSoutheastAsian immigrant women in Montreal: an exploratory study. Canadian Journal of Public Health 91:357–60.
- Katz D and Gagnon AJ (2002) Evidence of adequacy of postpartum care for immigrant women. Canadian Journal of Nursing Research 34:71–81.
- Kreiner M (2009) Delivering diversity: newlyregulatedmidwiferyreturns to Manitoba, Canada, one community at a time. Journal of Midwifery and Women’s Health 54:e1– 10.
- Kurtz Landy C, Sword W and Ciliska D (2008) Urban women’ssocioeconomicstatus, health service needs and utilization in the four weeksafter postpartum hospitaldischarge: findings of a Canadian cross-sectional survey. BMC Health Services Research 8:1–9.
- Kymlicka W (2003) Immigration, citizenship, multiculturalism: exploring the links. PoliticalQuarterly 74(S1): 195–208.
- Loiselle CG, Semenic SE, Cote B et al (2001) Impressions of breastfeeding information and support among first-time motherswithin a multiethnic community. Canadian Journal of Nursing Research 33:31–46.
- Mechakra-Tahiri S, Zunzunegui MV and Seguin L (2007) Self-rated health and postnatal depressive symptoms among immigrant mothers in Quebec. Women and Health 45:1– 17.
- Meddings F and Haith-Cooper M (2008) Culture and communication in ethically appropriate care. Nursing Ethics 15:52–61.
- Minde K, Tidmarsh L and Hughes S (2001) Nurses’ and physicians’ assessment of mother–infant mental health at the first postnatal visits. Journal of the American Academy of Childhood and Adolescent Psychiatry 40:803–10.
- Morrow M, Smith JE, Lai Y et al (2008) Shiftinglandscapes: immigrant women and postpartum depression. Health Care for Women International 29:593–617.
- Napoles-Springer AM, Santoyo J, Houston K et al (2005) Patients’ perceptions of cultural factors affecting the quality of their medical encounters. Health Expectations 8:4–17.
- Newbold KB (2005) Self-rated health within the Canadian immigrant population: risk and the healthy immigrant effect. Social Science and Medicine 60:1359–70.
- Newbold KB and Willinsky J (2009) Providing family planning and reproductive healthcare to Canadian immigrants: perceptions of healthcare providers. Culture, Health, and Sexuality 11:369–82.
- Ng G, Pottie K, Spitzer D (2011) Official languageproficiency and self-reported health among immigrants to Canada. Health Reports 22:15–23.
- O’Mahony J and Donnelly T (2012) How doesgender influence immigrant and refugeewomen’s postpartum depression help-seekingexperiences? Journal of Psychiatric and Mental Health Nursing Online September 11 doi: 10.1111/jpm.12005.
- Oxman-Martinez J, Hanley J, Lach L et al (2005) Intersection of Canadian policy parametersaffecting women with precarious immigration status: a baseline for understandingbarriers to health. Journal of Immigrant Health 7:247– 58.
- Preyde M (2007) Mothers of verypreterm infants: perspectives on their situation and a culturally sensitive intervention. Social Work in Health Care 44:65–83.
- Ray JG, Vermeulen MJ, Schull MJ et al (2007) Results of the Recent Immigrant Pregnancy and Perinatal Long-term Evaluation Study (RIPPLES). Canadian Medical Association Journal 176:1419–26.
- Redwood-Campbell L, Thind H, Howard M et al (2008) Understanding the health of refugee women in host countries: lessons from the Kosovar re-settlement in Canada. Prehospital and Disaster Medicine 23:322–7.
- Reitmanova S and Gustafson DL (2008) ‘Theycan’t understand it’: maternity health and care needs of immigrant Muslim women in St John’s, Newfoundland. Maternal and Child Health 12:101–11.
- Russell C (2005) An overview of the integrative research review. Progress in Transplantation 15:8–13.
- Sanmartin C and Ross N (2006) Experiencingdifficultiesaccessing first-contact health services in Canada. Healthcare Policy 1:103–19.
- Small R, Gagnon A, Gissler M et al (2008) Somali women and theirpregnancyoutcomespostmigration: data from six receiving countries. BJOG An International Journal of Obstetrics and Gynaecology 115:1630–40.
- Spitzer DL (2004) In visible bodies: minority women, nurses, time, and the new economy of care. Medical AnthropologyQuarterly 18:490–508.
- Statistics Canada (2008) Canada’sEthnoculturalMosaic, 2006 Census. Censusyear 2006. www12.statcan.ca/censusrecensement/ 2006/as-sa/97–562/pdf/97–562- XIE2006001.pdf (accessed 12 October 2012).
- Statistics Canada (2010) Projections of the Diversity of the Canadian Population. www.statcan.gc.ca/pub/91–551-x/ 91–551-x2010001-eng.pdf (accessed 4 July 2012).
- Statistics Canada (2012) Alberta (Code 48) and Canada (Code 01) (table). Census Profile. 2011 Census. www12. statcan.ca/census-recensement/2011/dp-pd/prof/index. cfm?Lang=E (accessed 4 July 2012).
- Stewart DE, Gagnon A, Saucier JF et al (2008) Postpartum depression symptoms in newcomers. Canadian Journal of Psychiatry 53:121–4.
- Sword W, Watt S and Krueger P (2006) Postpartum health, service needs, and access to care experiences of immigrant and Canadian-born women. Journal of Obstetric, Gynecologic and Neonatal Nursing 35:717–27.
- Teng L, Blackmore ER and Stewart DE (2007) Healthcareworkers’ perceptions of barriers to care by immigrantwomen with postpartum depression: an exploratory qualitative study. Archive of Women’s Mental Health 10:93–101.
- Urquia M and Gagnon AJ (2011) Glossary: migration and health. Journal of Epidemiology and Community Health 65:467–72.
- Urquia M, Frank JW, GlazierRHet al (2007) Birth outcomes by neighbourhoodincome and recent immigration in Toronto. Health Reports 18:21–32.
- Wang L, Rosenburg M and Lo L (2008) Ethnicity and utilization of familyphysicians: a case study of Mainland Chinese immigrants in Toronto, Canada. Social Science and Medicine 67:1410–22.

