Yohei Kitano1, Kakuya Matsumoto1, Kenji Chisaka1, Masako Imazawa1, Kenji Takahashi1, Yukiomi Nakade1, Mituyoshi Okada1, Kazunobu Aso1, Kazunori Yokoyama2, Masahiro Yamamoto3, Masumi Yoshie3, Katsuhiro Ogawa3, Masakazu Haneda1
1Second Department of Medicine, Asahikawa Medical College; 2National Hospital Organization,
Dohoku National Hospital; 3Department of Pathology, Asahikawa Medical College.
Asahikawa, Japan
- *Corresponding Author:
- Yohei Kitano
Second Department of Medicine
Asahikawa Medical College
Midorigaoka Higashi 2-1-1-1
Asahikawa 078-8510
Japan
Phone: +81-166.682.454
Fax: +81-166.682.459
E-mail: kitano@asahikawa-med.ac.jp
Received May 15th, 2007 - Accepted June 5th,
2007
Keywords
Autoimmune Diseases; Autopsy; Pancreatitis, Chronic
INTRODUCTION
Autoimmune pancreatitis is an increasingly recognized type of chronic pancreatitis, characterized by the following unique clinical, diagnostic imaging and pathological features: high incidence in middle to advanced aged men, pancreatic enlargement, irregularly narrowed pancreatic duct and bile duct stricture on endoscopic retrograde cholangiopancreatography (ERCP) images, increased levels of serum IgG and IgG4, presence of serum autoantibodies, and lymphoplasmacytic infiltration with fibrosis in the pancreas [1, 2]. Little is known about the long-term outcome of autoimmune pancreatitis. Nishino et al. [3] reported on the long-term outcome of autoimmune pancreatitis after prednisolone therapy. They found that the pancreatic enlargement and pancreatic duct narrowing improved in all cases, and that pancreatic atrophy developed in some. Bile duct stricture also improved in all patients but recurred in one. There are other follow-up reports about morphological or functional changes [4, 5, 6, 7, 8] but very few reports about pathological changes. The pathological findings of autoimmune pancreatitis in the inactive state are not well-known. We experienced a case of autoimmune pancreatitis and followed its natural course until death. We herein present the changes in clinical manifestation and the autopsy findings.
CASE REPORT
The patient was an 81-year-old Japanese male. He noticed general pruritus and malaise in January 1996 and was admitted to our Department with jaundice on February 23rd, 1996. He was not a habitual drinker and did not smoke. Past history and family history were not contributory. Physical examination on admission revealed jaundice of the bulbar conjunctiva, slight resistance in the right hypochondrium, and normal body temperature. Laboratory data showed the following values: 20.6 mg/dL total bilirubin, 16.4 mg/dL direct bilirubin, 1,604 IU/L alkaline phosphatase, 48 IU/L serum amylase, 0.89 mg/dL C-reactive protein, 9.0 g/dL total protein, and 3.3 g/dL serum albumin (Table 1). Abdominal CT showed diffuse enlargement of the pancreas (Figure 1). ERCP images revealed a severe stricture of the distal common bile duct, and cholangiography via a nasobiliary drainage tube showed irregularity of the intrahepatic and hilar bile ducts (Figures 2a, 2b). Endoscopic retrograde pancreatography revealed irregular narrowing of the main pancreatic duct and swelling of the papilla of Vater (Figures 2c, 2d). Following ERCP, we performed a transpapillary forceps biopsy.
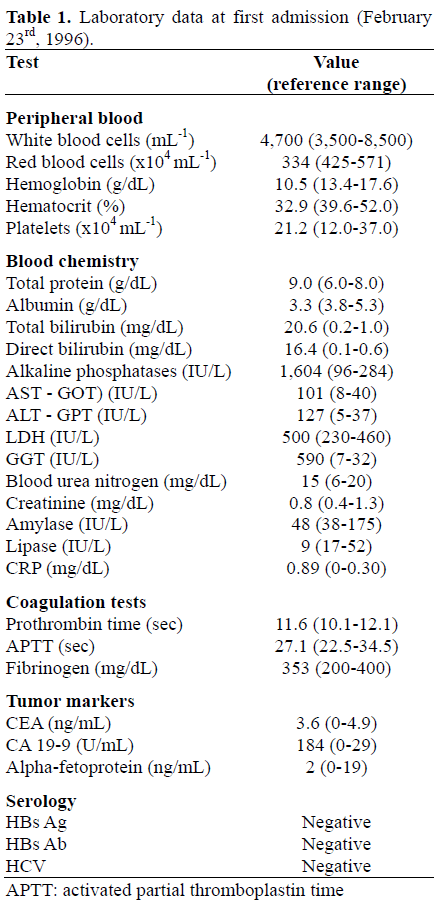
Figure 1. a. b. c. Abdominal computed tomography
findings at first admission (February 1996). Note the
diffuse enlargement of the pancreas and dilatation of
the biliary tract.
Figure 2. Findings at first admission (February 1996): a. endoscopic retrograde cholangiography; b. cholangiography via nasobiliary drainage tube; c. d. endoscopic retrograde pancreatography. a. Note the
severe stricture of the distal bile duct. b. Irregularity of
intrahepatic bile ducts (arrows). c. Irregular narrowing
of the main pancreatic duct. d. Swelling of the papilla
of Vater.
Although the biopsy specimen did not reveal malignancy, cholangiocarcinoma was thought to be the most likely diagnosis. Surgery was not performed due to the advanced age of the patient. The patient was discharged after endoscopic biliary drainage was performed . A plastic stent, 12 Fr in diameter, was used for the endoscopic biliary drainage. At his second admission in November 1998, enlargement of the pancreas, narrowing of the main pancreatic duct and a stricture of the common bile duct had improved on CT and ERCP (Figure 3) without steroid therapy. The serum IgG level was elevated (2,490 mg/dL; reference range: 607-1,621 mg/dL). The antinuclear antibody (ANA) was positive and the titer was x320. After these investigations, he was diagnosed conclusively as having chronic pancreatitis, and the biliary stent was removed. The stent had never been exchanged until this time because he had temporarily dropped out from follow-up from 1996 to 1998. A Gallium scintigraphy in January 1999 revealed no abnormal uptake, except in the bilateral lower lung fields, which was suspected to be interstitial pneumonia (Figure 4). On follow-up ERCP, 4 years after onset (November 2000), the common bile duct stricture had not recurred, and the papilla of Vater swelling had improved (Figures 5a, 5b). The narrowing of the main pancreatic duct had improved further (Figure 5c). Abdominal CT in January 2002 showed atrophy of the pancreas (Figure 6). The serum IgG level was higher than the upper reference limit throughout the course after 1998, although it was not determined at the first admission. The serum IgG4 level was checked once in October 2001 (264 mg/dL; reference range 6-140 mg/dL). On two occasions, the N-benzoyl-L-tyrosyl-para-aminobenzoic acid (BT-PAVA) excretion value showed abnormally low levels (27% and 28%, respectively; reference range 73.4-90.4%). The hemoglobin A1c (HbA1c) level was within the reference range.
Figure 3. Endoscopic retrograde cholangiopancreatography
findings (a. cholangiogram; b. pancreatogram)
at second admission (November 1998). Bile duct
stricture and narrowing of the main pancreatic duct
obviously improved.
Figure 4. Gallium scintigraphy findings (January
1999). Abnormal uptake was seen in the bilateral lower
lung fields. No hilar adenopathy or sialadenitis was
found.
Figure 5. Endoscopic retrograde cholangiopancreatography
findings on third admission (November 2000). a. No stricture was seen on cholangiography. b. Swelling of the papilla of Vater had improved. c. Pancreatography findings improved further. Only a
slight irregularity of the main pancreatic duct
remained.
Figure 6. a. b. c. Abdominal computed tomography
findings 6 years after onset (January 2002). Note that
atrophy of the pancreas has become evident.
He died on June 2nd, 2003 from interstitial pneumonia and congestive heart failure. There had been no steroid administration during the entire period. At autopsy, fibrosis was found in the periductal, interlobular and intralobular parts of the pancreas, and atrophy of the acinar cells was identified (Figure 7). There was very little periductal lymphoplasmacytic infiltration.
Figure 7. Histology of the autopsy specimens of the pancreas. a. b. Atrophy of the acinar cells and fibrosis. Very little
infiltration of inflammatory cells (H&E x40). c. Periductal and interlobular fibrosis clearly seen (Masson x40). d. Immunohistostaining revealed no IgG4 positive plasmacytes (x40).
IgG4 positive plasmacyte infiltration was not identified on immunohistostaining. There was no obliterative phlebitis, and neither pseudocysts nor calculi were seen in the pancreas. Examination of the kidneys revealed partial necrosis of the glomeruli with mild interstitial lymphocyte infiltration. There was interstitial nephritis but no IgG4 positive plasmacyte infiltration. There was periductal fibrosis of both the intrahepatic and the extrahepatic bile ducts, but very little infiltration by inflammatory cells (Figure 8). Severe fibrosis and severe inflammatory cell infiltration were found in the alveolar walls and the alveoli of the lungs.
Figure 8. a. Histology of the intrapancreatic bile duct
(H&E x40). Periductal fibrosis is obvious and there is
minor inflammatory cell infiltration. b. Histology of
the intrahepatic bile duct (H&E x40). Periductal
fibrosis can be clearly seen. Minor infiltration of the
inflammatory cells. Hepatic sinusoids dilated due to
congestion.
DISCUSSION
The number of reported cases of autoimmune pancreatitis is increasing and, recently, it has been widely recognized as a clinical entity of chronic pancreatitis. Many groups have cited the diagnostic criteria proposed by the Japan Pancreas Society [9], which include serological, imaging and pathological findings. American and Korean groups suggested other diagnostic criteria in 2006, which also include the response to steroid therapy [10, 11]. Our case showed diffuse enlargement of the gland, irregular narrowing of the main pancreatic duct, and abnormal levels of serum IgG, IgG4 and ANA. These findings fulfill all three diagnostic criteria for autoimmune pancreatitis. Swelling of the papilla of Vater is also sometimes found [12]. These imaging findings improved spontaneously in this case without steroid therapy, which has also been described in other reports [4, 8], and is compatible with autoimmune pancreatitis. Reduced pancreatic exocrine function is also compatible with autoimmune pancreatitis [7].
In this case there were no co-existing collagen diseases, and no clear extrapancreatic lesions such as hilar adenopathy, sialadenitis or retroperitoneal fibrosis. It is not known why the serum IgG levels remained high.
Histopathological findings of autoimmune pancreatitis have been reported as follows: infiltration of inflammatory cells around large and medium sized pancreatic ducts, IgG4 positive plasma cell infiltration, fibrotic changes, atrophy of acinar cells and obliterated phlebitis [13, 14, 15]. At autopsy, very few inflammatory cells and IgG4 positive plasma cells were found in the pancreas, but fibrotic changes and acinar cell atrophy were detected. There have only been two reports in the English literature about histological changes in autoimmune pancreatitis after steroid therapy [16, 17]. These reports describe histological improvement including amelioration of the fibrosis and inflammatory cell infiltration, and a substantial increase in the number of pancreatic acinar cells. These findings may support reversibility of the histological findings if autoimmune pancreatitis patients are treated with steroids, but the follow-up period seems short in these reports. Other reports on the long-term outcome of autoimmune pancreatitis after steroid therapy described pancreatic atrophy and stone formation in some cases [3, 8, 18]. It is not clear whether histological and morphological findings improve or deteriorate after steroid therapy in the long term.
In our case, there was no steroid administration through the course because the patient had had no symptoms of autoimmune pancreatitis after the second admission in 1998. The pathological findings and atrophy of the pancreas on CT images seemed more compatible with ‘conventional’ chronic pancreatitis than with autoimmune pancreatitis. This implies that some autoimmune pancreatitis cases may change into ‘conventional’ chronic pancreatitis without steroid therapy and that a diagnosis of autoimmune pancreatitis should be made in an early phase of the disease. It is also possible that IgG4 positive plasma cell infiltration is of use in diagnosis only in an early phase of autoimmune pancreatitis. In the late phase, the diagnosis of autoimmune pancreatitis may be made difficult by other pathological findings. To our knowledge, this is the first autopsy case of autoimmune pancreatitis which has evolved according to its natural history. Additional experience is needed to clarify whether some autoimmune pancreatitis cases change to ‘conventional’ chronic pancreatitis or not.
Conflict of interest
The authors have no potential conflicts of interest
References
- Okazaki K, Chiba T. Autoimmune related
pancreatitis. Gut 2002; 51:1-4. [PMID 12077078]
- Kim KP, Kim MH, Song MH, Lee SS, Seo DW,
Lee SK. Autoimmune chronic pancreatitis. Am J
Gastroenterol 2004; 99:1605-16. [PMID 15307882]
- Nishino T, Toki F, Oyama H, Shimizu K, Shiratori
K. Long-term outcome of autoimmune pancreatitis
after oral prednisolone therapy. Intern Med 2006;
45:497-501. [PMID 16702740]
- Fujii T, Chiba A. Chronic pancreatitis with diffuse
irregular narrowing of the main pancreatic duct: follow
up study. J Jpn Pan Soc 2002; 17:655-64.
- Nishimori I, Suda K, Oi I, Ogawa M. Research on
the clinical state of autoimmune pancreatitis. J Jpn Pan
Soc 2002; 17:619-27.
- Czakó L, Hegyközi E, Pálinkás A, Lonovics J.
Autoimmune pancreatitis: functional and
morphological recovery after steroid therapy. World J
Gastroenterol 2006; 12:1810-2. [PMID 16586561]
- Kamisawa T, Egawa N, Inokuma S, Tsuruta K,
Okamoto A, Kamata N, et al. Pancreatic endocrine and
exocrine function and salivary gland function in
autoimmune pancreatitis before and after steroid
therapy. Pancreas 2003; 27:235-8. [PMID 14508128]
- Kamisawa T, Yoshiike M, Egawa N, Nakajima H,
Tsuruta K, Okamoto A. Treating patients with
autoimmune pancreatitis: results from a long-term
follow-up study. Pancreatology 2005; 5:234-8. [PMID
15855821]
- Members of the Criteria Committee for
Autoimmune pancreatitis of the Japan pancreas society.
Diagnostic criteria for autoimmune pancreatitis by the
Japan Pancreas Society (2002). J Jpn Pan Soc 2002;
17:585-7.
- Kim KP, Kim MH, Kim JC, Lee SS, Seo DW, Lee
SK. Diagnostic criteria for autoimmune chronic
pancreatitis revisited. World J Gastroenterol 2006;
12:2487-96. [PMID 16688792]
- Chari ST, Smyrk TC, Levy MJ, Topazian MD,
Takahashi N, Zhang L, et al. Diagnosis of autoimmune
pancreatitis: the Mayo Clinic experience. Clin
Gastroenterol Hepatol 2006; 4:1010-6. [PMID
16843735]
- Sahin P, Pozsár J, Simon K, Illyés G, László F,
Topa L. Autoimmune pancreatitis associated with
immune-mediated inflammation of the papilla of Vater:
report on two cases. Pancreas 2004; 29:162-6. [PMID
15257109]
- Klöppel G, Lüttges J, Sipos B, Capelli P, Zamboni
G. Autoimmune pancreatitis: Pathological Findings.
JOP. J Pancreas (Online) 2005; 6(1 Suppl.):97-101.
[PMID 15650292]
- Zhang L, Notohara K, Levy M, Chari ST, Smyrk
TC. IgG4-positive plasma cell infiltration in the
diagnosis of autoimmune pancreatitis. Mod Pathol
2007; 20:23-8. [PMID 16980948]
- Kawaguchi K, Koike M, Tsuruta K, Okamoto A,
Tabata I, Fujita N. Lymphoplasmacytic sclerosing
pancreatitis with cholangitis: a variant of primary
sclerosing cholangitis extensively involving pancreas.
Hum Pathol 1991; 22:387-95. [PMID 2050373]
- Saito T, Tanaka S, Yoshida H, Imamura T,
Ukegawa J, Seki T, et al. A case of autoimmune
pancreatitis responding to steroid therapy. Evidence of
histologic recovery. Pancreatology 2002; 2:550-6.
[PMID 12435868]
- Song MH, Kim MH, Lee SK, Seo DW, Lee SS,
Han J, et al. Regression of pancreatic fibrosis after
steroid therapy in patients with autoimmune chronic
pancreatitis. Pancreas 2005; 30:83-6. [PMID
15632704]
- Takayama M, Hamano H, Ochi Y, Saegusa H,
Komatsu K, Muraki T, et al. Recurrent attacks of
autoimmune pancreatitis result in pancreatic stone
formation. Am J Gastroenterol 2004; 99:932-7. [PMID
15128363]









