Keywords
Diabetes Mellitus, Type 2; Diabetic Nephropathies; Diabetic Neuropathies; Hemoglobin A, Glycosylated; Wound Healing
Abbreviations
T2DM type 2 diabetes mellitus; WBV whole body vibration;
INTRODUCTION
Diabetes is the fifth leading cause of death in the US, and according to the National Diabetes Statistics Report in 2014 approximately 29 million Americans are living with diabetes mellitus with the majority being type 2 diabetes mellitus (T2DM) [1]. It is reported that every 10 seconds a person dies worldwide secondary to a diabetesrelated pathology [2]. The prevalence of childhood obesity continues to rise dramatically, going hand in hand with the increased incidence of T2DM. According to recent studies, 25% of children and adolescents are overweight or obese [3]. The prevalence of T2DM in adolescents 12 to 19 years rose from 9% in 1999/2000 to a staggering 23% in 2007/2008 according to the 2008 National Health and Nutrition Examination Survey (NHANES) [4, 5]. Excess caloric intake combined with decreased physical activity and energy expenditure as a result of a more sedentary lifestyle has led to this inevitable increase in T2DM and obesity. These lifestyle trends have resulted in a staggering rise of Lifestyle-Related Chronic Diseases including diabetes, obesity, hypertension, and cardiovascular disease [6]. With the increasing prevalence of T2DM, there is increasing economical burden worldwide as a result of secondary health complications [2].
Central obesity, impaired insulin secretion from pancreatic B-cells, and decreased insulin sensitivity of peripheral tissues contribute to insulin resistance which results in hyperglycemia and ultimately T2DM as a result of a progressive imbalance in glucose homeostasis. Recent studies have reported pancreatic beta cells as regulators of rhythmic transcription genes controlling insulin secretion, revealing an essential role of the circadian timing system in diabetes [7, 8]. Excess visceral adipose tissue is independently associated with the development of diabetes secondary to increased insulin resistance [4, 9]. Impaired insulin-induced signal transduction results in peripheral insulin resistance via impairment of membrane translocation of glucose transporters [1, 10]. Pharmacologic treatment has focused on improving tissue sensitivity, increasing insulin levels, and reducing carbohydrate absorption from the gastrointestinal tract [2]. In short, the pathogenesis behind T2DM is multifactorial and requires evolving treatment modalities to improve management of this complex disease process.
Nutrition and exercise are the number one recommendations for treatment of T2DM. With regular exercise there is an increase in energy expenditure with the expectation of decreasing peripheral adipose tissue. With resistance training and aerobic exercise there is generally a reduction in HbA1c, fasting glucose, hyperlipidemia, and hypertension [11]. Exercise may also improve glycemic control in T2DM due to anti-inflammatory properties as demonstrated in animal models [1, 12-14]. Although this approach is the most recommended, there is low compliance long term with strenuous and time-consuming exercise regimens. Thus, there is the need for developing new and novel treatment strategies. Like exercise, whole body vibration (WBV) exerts mechanical stresses on the skeleton, which could potentially indicate a novel exercise modification. It may allow the health benefits of exercise without the intensity and duration of standard sustained exercise programs. This review will detail specific findings involving the effects of standard high frequency, low-amplitude WBV on factors related to T2DM such as body mass composition, glycemic control, renal function, inflammation, peripheral neuropathy, and wound healing.
WHAT IS WHOLE BODY VIBRATION (WBV)?
Whole Body Vibration (WBV) is a relatively new area of interest in medicine with increasing focus on the effects WBV has on various systems. It has demonstrated promise as a new modality in therapy for a number of different disease processes. Utilizing specific frequencies and amplitudes, WBV transmits vibration via vertical (synchronous) or side-alternating (oscillating) platforms to the body while standing on the delivering platform [15, 16]. Frequencies and amplitudes delivered through the vibrating platforms range between 5-90 Hz and up to 10mm respectively [17]. During WBV treatment with low magnitude/high frequency vibration, mechanical stimuli are transmitted throughout the body, loading bone and stimulating sensory receptors and muscle spindles, which in turn causes contractions that lead to tonic vibration reflexes [15-17]. This ultimately elicits a warm-up effect, which can improve muscle power and strength [16].
Many studies utilizing WBV have been performed on patients with neurologic disorders such as Parkinson’s, Cerebral palsy, stroke, etc. to evaluate the benefits on spasticity, rigidity, tremor, balance, and muscle weakness [15]. WBV has also been a major area of focus in athletic conditioning and rehabilitation. More recent studies have focused on vibration exercises to prevent osteoporosis and muscular atrophy, to improve muscle strength and balance, to improve skin blood flow, and to improve glycemic control [18-21]. Although not as extensively studied, more recent research is focusing on the application of WBV therapy in T2DM as discussed below. The beauty of utilizing WBV as an exercise modality is the reduced time and effort required of individuals when compared with standard exercise regimens, thus representing a potentially new and novel adjunctive therapy in T2DM.
WHOLE BODY VIBRATION THERAPY AND TYPE 2 DIABETES MELLITUS
Effects of WBV on Glucose Metabolism
Glycemic control is the cornerstone of treatment of diabetes and the degree of glycemic control is directly related to the risk for diabetic complications [2]. Therefore, treatment is aimed at reducing hyperglycemia to minimize these complications. Many studies have demonstrated improved glucose control with the use of WBV therapy. Studies have been performed in murine and human models to evaluate the effects of WBV on glucose control. A clinical report from Germany in 2007 demonstrated superior glycemic control in elderly patients with T2DM treated with WBV when compared to the control [20]. This study utilized a daily horizontal swing administering WBV at 2mm maximum amplitude and a frequency of 30 Hz for three weeks, reporting a decrease in peak fasting glucose concentrations of 6% following oral glucose tolerance testing [20].
Yin et al. studied the effects of WBV therapy on diabetic (db/db) and non-diabetic (db/m) mice. This study demonstrated a reduced HbA1c (~22 %; p <0.05) in the vibrated diabetic mice when compared with nonvibrated diabetic mice; however, WBV did not affect HbA1c levels in the non-diabetic mice (Figure 1) [1]. The authors of this study prompted further speculation that an osteocyte-dependent process may be a likely contributor to the regulation of glucose. The reasoning behind this postulation lies in the bone’s role as an endocrine organ secreting osteocalcin which leads to an increase in B-cell mass, insulin secretion, and insulin sensitivity, which ultimately will lower blood glucose [1, 22]. The skeleton undergoes stress secondary to muscle contractions and gravitation during exercise, creating fluid flow within the lacuna-canalicular systems of the bone [1, 23]. This results in osteocyte stimulation to signal for osteoblast synthesis and release of osteocalcin [1, 24]. Therefore, osteocalcin could potentially cause the exercise-induced improvement in insulin sensitivity and glucose control secondary to the exercise stimulated increased release of osteocalcin by bone (Figure 2) [1, 25]. Although the reason for improved glycemic control is unclear, the data from the mouse model strongly suggests that WBV has beneficial effects on glucose metabolism [1].
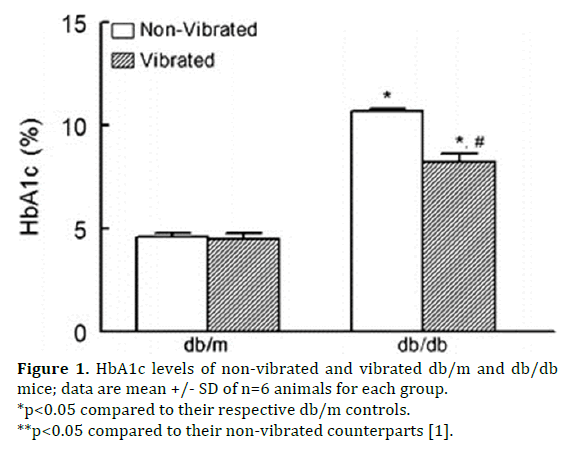
Figure 1. HbA1c levels of non-vibrated and vibrated db/m and db/db mice; data are mean +/- SD of n=6 animals for each group.
*p<0.05 compared to their respective db/m controls.
**p<0.05 compared to their non-vibrated counterparts [1].
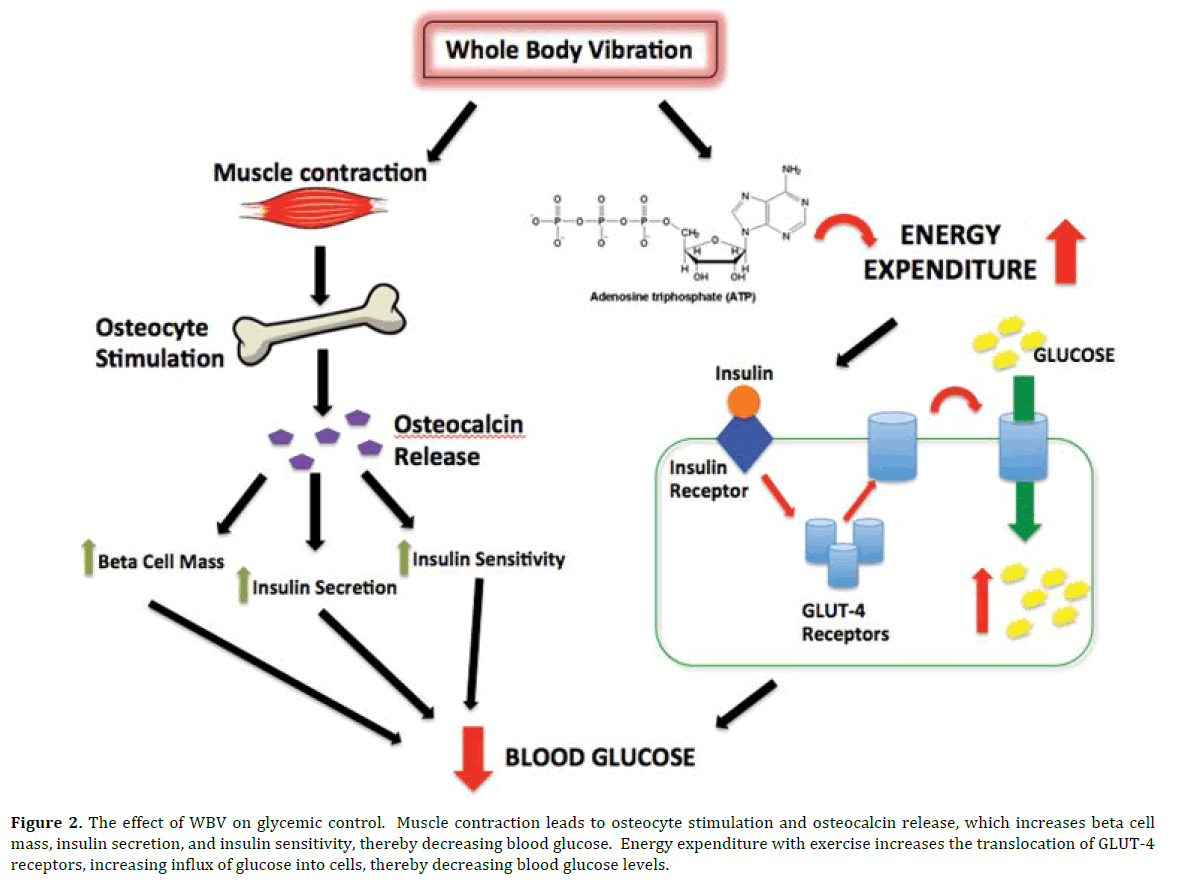
Figure 2. The effect of WBV on glycemic control. Muscle contraction leads to osteocyte stimulation and osteocalcin release, which increases beta cell mass, insulin secretion, and insulin sensitivity, thereby decreasing blood glucose. Energy expenditure with exercise increases the translocation of GLUT-4 receptors, increasing influx of glucose into cells, thereby decreasing blood glucose levels.
Glut-4 is a specific glucose transporter found in adipocytes and skeletal muscle that facilitates movement of glucose into the cell following insulin stimulation which is of particular interest in this topic as resistance training increases energy expenditure as well as insulin-induced membrane translocation of GLUT-4 [1, 10]. If WBV does indeed mimic resistance training and achieves the same physiologic effects, it could stimulate this insulin-induced membrane translocation of GLUT-4, providing an additional logical reason behind the improved glycemic control seen in subjects following WBV therapy (Figure 2).
Pozo-Cruz et al. performed a study on the feasibility and safety of utilizing WBV treatment for 12 weeks to reduce cardiovascular risk factors in T2DM patients with a sedentary lifestyle [11]. They demonstrated a reduction in HbA1c and fasting glucose in patients with T2DM in a primary care setting [11]. Alfonso-Rosa et al. further described the cost-utility of a 12-wk WBV treatment in patients with T2DM, demonstrating that WBV in comparison to standard care is indeed cost-effective [26].
There is great promise with WBV as a treatment modality in patients with T2DM to improve glycemic control. WBV may simulate actual exercise in a manner that stimulates similar pathways thus causing improvement in glucose metabolism. More extensive studies are needed to further evaluate the effects of WBV on glycemic control.
Effects of WBV on Renal Function
Diabetic nephropathy is a major complication affecting approximately 40% of patients worldwide and has been reported as one of the leading causes of renal failure in the United States [2]. The cause of diabetic nephropathy is a result of progressive microvascular disease resulting from a chronic hyperglycemic state. Very few studies have been performed that focus on the effects of WBV on renal function with virtually no discussion of the effect in humans. However, this is a critical system to study secondary to the natural disease process of diabetes largely impacting the renal system. A few select studies exist utilizing murine models that demonstrate promise for improvement in renal function following WBV therapy.
Lin et al. studied WBV benefits on diet-induced obese middle-aged mice to evaluate body composition, exercise performance, and physical fatigue-related and biochemical responses [27]. This study utilized both high frequency WBV (13 Hz, 2mm, 0.68g) and low frequency WBV (5.6 Hz, 2 mm, 0.13 g), reporting a dose-dependent decrease in creatinine that was seen in mice treated with WBV compared to controls (p=0.0020) [27].
In an investigation of diabetic nephropathy performed by Mozaffari et al. there was a reported increase in immunostaining of gamma-H2AX (a marker of cell injury) in renal tissue in diabetic mice when compared with nondiabetic mice [28]. In another study by Baban et al. renal cells prepared from kidneys of diabetic mice demonstrated an increase in IL-17 (pro-inflammatory marker) in diabetic mice when compared to non-diabetic mice [29]. Yin et al. reported a statistically significant decrease in IL- 17 and gamma-H2AX in diabetic mice treated with WBV when compared to unvibrated diabetic mice. This could demonstrate a significant impact on renal function.
Yin et al. further addressed renal function in terms of measuring water intake, urine excretion, and urine osmolality in adolescent diabetic and non-diabetic mice [1]. In this study, WBV did not affect urine osmolality or urine output but did stimulate an increase in fluid intake in the non-diabetic mice [1]. However, the diabetic mice demonstrated reduced fluid intake by 25%, decreased urine excretion, and increased urine osmolality by 28%, consistent with improved urinary concentrating abilities [1].
If whole body vibration can improve creatinine and decrease cellular damage to kidneys, one could postulate that this could have a significant impact on the treatment and prevention of diabetic nephropathy. Additional research is needed in this area to evaluate the effects of WBV on the renal system.
Effects of WBV on Body Mass Composition
If WBV is considered a modification of resistance training exercise then one would expect that it should help decrease body fat, increase lean mass, and improve bone density. In an obese subject, one would expect a decrease in weight following WBV therapy. Unfortunately, current research results that focus on this area are controversial as to the true effect of WBV on body composition.
In a murine model, Yin et al. did not demonstrate a significant difference in weight between vibrated and non-vibrated mice in both the diabetic group and nondiabetic group of mice [1]. However, specific lean mass versus adipose tissue was not evaluated in this model. Lin et al. studied body composition in their research of WBV in diet induced, middle aged mice [27]. This study again demonstrated no difference in body weight; however, they did report a significant decrease in the absolute and relative weight of the liver as well as a frequency dosedependent increase in the absolute and relative weight of brown adipose tissue [27].
With regards to human research, Gonzalez-Aguero et al. studied the effect of WBV on body composition in adolescents with Down syndrome. After measuring upper and lower limb body fat and lean body mass, they reported a reduction in body fat of the upper limbs (p<0.05) and an increase in whole body lean mass following 20 weeks of WBV therapy [30]. Conversely, Pitukcheewanont et al. and Söderpalm et al. reported no difference in femoral fat mass following WBV treatment as measured by Computed Tomography and Dual energy X-ray modalities respectively [31, 32]. Pitukcheewanont et al. did, however, report significant increases of 6.2% in cancellous bone density, 2.1% in cortical bone density, and 6.1% in muscle mass [31]. Pozo-Cruz et al. reported no significant difference in weight in T2DM following a 12-wk WBV regimen, although they did demonstrate a significant reduction in lipidrelated cardiovascular risk factors such as cholesterol, triglycerides, and atherogenic index [11].
Animal models with osteoporosis have been studied and demonstrated improved bone density and bone strength following treatment with short-term lowintensity, high frequency mechanical stimulation [31]. As previously stated, Pitukcheewanont et al. demonstrated an increase in bone density in children, though it was studied in children with pre-existing low bone density [31]. Söderpalm et al. reported no significant change in bone mass, muscle strength, or bone density when studying the effect of WBV therapy in patients with Duchene Muscular Dystrophy but did report an increase in a marker for bone formation: bone-specific alkaline phosphate [32]. Ruck et al. studied WBV therapy in children with cerebral palsy and actually found an increase in areal bone mineral density at the lumbar spine but a decrease in bone density in the diaphysis of the femur in the WBV group [33].
Much controversy exists regarding the effects of WBV on body composition. Although WBV has not been reported to have a significant impact on weight, it may affect individual aspects to overall improve body composition. If WBV can reduce body fat while increasing lean body mass and bone density, it would again demonstrate a possible alternative or adjunctive treatment option for obesity and T2DM. Further research focusing on individual aspects of body composition will be helpful to determine the effects of WBV on fat mass, lean muscle mass, and bone density.
Effects of WBV on Inflammatory Indices
Recent studies have reported that the pathology of diabetes involves chronic inflammatory processes, necessitating treatment of inflammatory events in this patient population [2]. Mozaffari et al. described multiple studies focusing on the interplay of systemic and tissue specific inflammatory events involved in the “diabetesassociated immune response” [2]. Insulin resistance and islet beta-cell dysfunction in T2DM has been reported to be secondary to oxidative stress, endoplasmic reticulum stress, lipid deposition in muscle, liver, and pancreas, amyloid deposition in the pancreas, and more [34]. Donath et al. reported immunological changes altered in obesity and T2DM such as specific cytokines and chemokines, leukocyte populations, tissue fibrosis, and apoptosis, suggesting the relationship between inflammation and the pathogenesis of T2DM [34]. Teixeira-Lemos described the anti-oxidant and anti-inflammatory effects of regular exercise as treatment and prevention of T2DM, recognizing this crucial interplay between inflammation and diabetes [12].
WBV has reportedly exerted beneficial effects on indices of inflammation and cell injury [1]. Yin et al. demonstrated a reduced pro-inflammatory profile and less cytotoxicity in mice treated with WBV by analyzing the whole blood of experimental animals for IL17 (a pro-inflammatory cytokine and marker of T helper cells) and Foxp3 (an antiinflammatory marker of regulatory T cells) expression [1, 35, 36]. IL-17 positive cells and Foxp3 positive cells were significantly reduced and increased respectively in the vibrated diabetic mice when compared to non-vibrated diabetic mice (Figure 3) [1].

Figure 3. FACS analysis of IL-17 (a) and Foxp3 (b) positive cells of peripheral blood obtained from vibrated and non-vibrated db/m and db/db mice; data are mean +/- SD of percent of CD4+ cells of n=6 mice/group.
*p<0.05 compared to their respective controls.
**p<0.05 compared to their non-vibrated counterparts [1].
Further evaluation of the expression of gamma-H2AX (a marker of DNA injury) demonstrated a markedly reduced percent of whole blood cells testing positive for gamma- H2AX in the vibrated db/db mice when compared to nonvibrated db/db mice (Figure 4) [1, 28, 37].
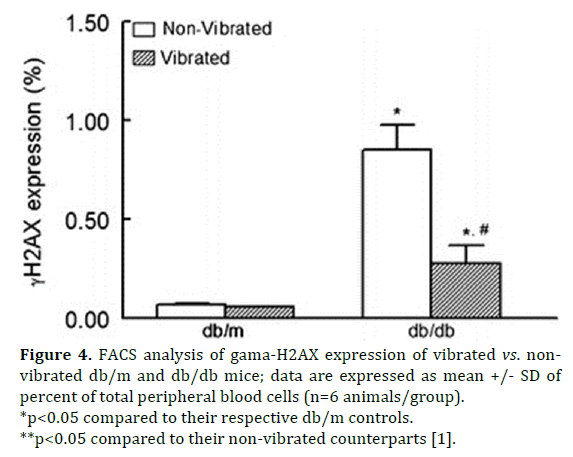
Figure 4. FACS analysis of gama-H2AX expression of vibrated vs. nonvibrated db/m and db/db mice; data are expressed as mean +/- SD of percent of total peripheral blood cells (n=6 animals/group).
*p<0.05 compared to their respective db/m controls.
**p<0.05 compared to their non-vibrated counterparts [1].
Overall these studies demonstrated improvement in inflammatory parameters with a decrease in cellular injury following WBV therapy. With inflammation identified as an integral factor in the pathogenesis of T2DM it is necessary to focus on treatments that will affect the inflammatory profile. If these studies can be translated to humans, WBV may indeed improve inflammatory parameter and in turn contribute to the treatment of T2DM.
Effects of WBV on Peripheral Neuropathy in Patients with Type 2 Diabetes
Peripheral neuropathy is commonly found in patients with long-standing diabetes mellitus as a result of progressive microvascular disease causing decreased blood flow to the skin and ultimately peripheral somatosensory deficits. In fact, neuropathies are one of the most common complications of diabetes mellitus, representing roughly 60% of non-traumatic amputations in the United States [19, 38].
Recent research has demonstrated the positive impact WBV has on balance in patients with peripheral neuropathy. Yoosefinejad et al. performed a study evaluating the short-term effects of WBV on the balance and muscle strength of patients with T2DM and pre-existing peripheral neuropathy. They reported significantly increased strength of the tibialis anterior (p=0.004) and quadriceps muscles (p=0.05) after only 6 weeks of WBV therapy [39]. This study also demonstrated a significant decrease in the “Timed Up & Go Test” (p=0.001), a measure of balance, when compared with the control [39]. Johnson et al. reported improved skin blood flow in subjects treated with lowfrequency, low-amplitude WBV [19].
The application for WBV in the treatment of diabetic peripheral neuropathy is multifactorial. Improving distal extremity strength will likely improve balance control, an important consequence of peripheral neuropathy. More importantly, if WBV may be applied in the treatment of T2DM, it could be postulated that if it results in improved skin blood flow then it could potentially prevent, or at least slow the progression, of the microvascular disease effects causing this neurologic sequela.
Effects of WBV on Wound Healing
Yet another significant cause of morbidity and mortality in patients with T2DM are diabetic ulcers and poor wound healing. Approximately 25% of diabetics worldwide develop a foot ulcer, and greater than half of these wounds are unhealed after longterm treatment [40, 41]. Wound healing is intricate and involves multiple cell types and cellular processes such as clot formation, inflammation, epithelialization, angiogenesis, granulation tissue formation, wound contraction, and tissue remodeling [41]. With sustained nutrient and caloric excess there is a dysregulation of energy metabolism, which causes further detrimental effects [2]. Obesity and hyperglycemia cause apoptosis, necrosis, ischemia, hypoxia, cellular swelling, microangiopathy, neuropathy, persistent inflammation, and eventually tissue breakdown and chronic wounds [2]. If WBV can affect the steps of wound healing on a cellular level, one could expect an alteration in wound healing as a result (Figure 5).
Figure 5. WBV effects on factors influencing wound healing.
Weinheimer-Haus et al. described improved angiogenesis and wound healing in diabetic mice. This study evaluated delayed wound healing in diabetic mice receiving excisional cutaneous wounds with the experimental group receiving low-intensity vibration therapy for 30 min/d. At 7 and 15 days wound tissue was collected and evaluated with the vibrated group demonstrating increased angiogenesis and granulation tissue after 7 days of treatment and accelerated wound closure and re-epithelialization at days 7 and 15 of treatment [40].
Yet another important factor impacting wound healing is blood flow to the skin. As discussed earlier, Johnson et al. reported a significant increase in skin blood flow in diabetic patients with peripheral neuropathy receiving WBV when compared to the sham (p=0.115) [19]. Not only would improving skin blood flow likely improve peripheral neuropathy frequently found in diabetes as discussed above, but one would also expect to see an improvement in diabetic foot ulcers and delayed wound healing with improved skin blood flow (Figure 5).
CONCLUSION
With diabetic complications currently one of the leading healthcare problems in the United States and worldwide, it is necessary to continue the search for treatment modifications. WBV therapy is a potentially new and novel adjunctive therapy that could be beneficial in patients with T2DM. Improvement of weight and glycemic control will have a huge impact clinically for this patient population. Improvement in renal function would highly impact transplant medicine as it stands now with diabetic nephropathy a major factor contributing to the high demand for kidney transplants. Treatment altering the inflammatory pathologic basis of this disease could potentially impact multiple factors and secondary complications seen in this population. Improvement in peripheral neuropathy would not only improve quality of life but could also potentially decrease the incidence of non-healing wounds or injuries as a result of decreased sensation to the lower extremities. Lastly, improvement in wound healing would have a huge impact on the morbidity and mortality of this population.
Subsequent studies are necessary to evaluate the extent of benefits that WBV therapy could provide as an adjunctive treatment modality in T2DM. This subject needs to be further explored with randomized clinical trials of significance focusing on the various pathologic processes behind this multifactorial disease. There have not been any reported negative effects of WBV therapy, and as this could be a potential new and novel therapy, we believe it is not unreasonable to incorporate this treatment modality into the primary care setting.
Acknowledgements
We would like to acknowledge Michelle Barnes and Edwina Terrell for their administrative help and support, and Jeanene Pihkala at GRU flow cytometry core facility.
Conflicts of Interest
None of the authors have potential or existing conflicts of interest.
References
- Yin H, Berdel H, Moore D, Davis F, Liu H, Mozaffari M, Yu JC, et al. Whole Body Vibration Therapy: A Novel Potential Treatment for Type 2 Diabetes Mellitus. Springerplus 2015; 4:578. [PMID: 26543713]
- Mahmood S Mozaffari. New Strategies to Advance Pre/Diabetes Care: Integrative Approach by PPPM. New York London: Springer, 2013. Print.
- Sabin M, Kiess W. Childhood Obesity: Current and Novel Approaches. Best Pract Res ClinEndocrinolMetab 2015; 29:327-338. [PMID: 26051294]
- Onge E, Miller S, Motycka C, DeBerry A. A Review of the Treatment of Type 2 Diabetes in Children. J PediatrPharmacolTher 2015; 20:4-16. [PMID: 25859165]
- May AL, Kuklina EV, Yoon PW. Prevalence of cardiovascular disease risk factors among US adolescents, 1999-2008. Pediatrics 2012;6:1035-1041. [PMID: 22614778]
- Eaton SB, Konner M, Shostak M. Stone agers in the fast lane: chronic degenerative diseases in evolutionary perspective. Am J Med 1988; 84:739-749. [PMID: 3135745]
- Perelis M, Marcheva B, Ramsey KM, Schipma MJ, Hutchison AL, Taguchi A, Peek CB, et al. Pancreatic Beta Cell Enhancers Regulate Rhythmic Transcription of Genes Controlling Insulin Secretion. Science 2015; 350:650. [PMID: 26542580]
- Dibner C, Schibler U. A pancreatic clock times insulin release: Circadian oscillators of beta cells control insulin secretion and glucose homeostasis. Science 2015; 350: 628-629.
- Neeland IJ, Turer AT, Ayers CR, Powell-Wiley TM, Vega GL, Farzaneh-Far R, Grundy SM, et al. Dysfunctional adiposity and the risk of predia- betes and type 2 diabetes in obese adults. JAMA 2012; 308:1150-1159. ? [PMID: 22990274]
- Hughes VA, Fiatarone MA, Fielding RA, Kahn BB, Ferrara CM, Shepherd P, Fisher EC, et al. Exercise increases muscle GLUT-4 levels and insulin action in subjects with impaired glucose tolerance. Am J Phys 1993; 264:E855-E862. [PMID: 8333511]
- Pozo-Cruz BD, Alfonso-Rosa RM, Pozo-Cruz JD, Sanudo B, Rogers ME. Effects of a 12-wk whole body vibration based intervention to improve type 2 diabetes. Maturitas 2014; 77:52-58. [PMID: 24094494]
- Teixeira-Lemos E, Nunes S, Teixeira F, Reis F. Regular physical exercise training assists in preventing type 2 diabetes development: focus on its antioxidant and anti-inflammatory properties. CardiovascDiabetol 2011; 28:12. [PMID: 21276212]
- de Lemos ET, Reis F, Baptista S, Pinto R, Sepodes B, Vala H, Rocha-Pereira P, et al. Exercise training is associated with improved levels of C-reactive protein and adiponectin in ZDF (type 2) diabetic rats. Med SciMonit 2007; 13(8):BR168-BR174. [PMID: 17660720]
- de Lemos ET, Reis F, Baptista S, Pinto R, Sepodes B, Vala H, Rocha-Pereira P,et al. Exercise training decreases proinflammatory profile in Zucker diabetic (type 2) fatty rats. Nutrition 2009; 25:330-339. [PMID: 19062255]
- Kantele S, Karinkanta S, Sievanen H. Effects of long-term whole-body vibration training on mobility in patients with multiple sclerosis: A meta-analysis of randomized controlled trials. J NeurolSci2015; 358:31-37. [PMID: 26421830]
- Rittweger J. Vibration as an exercise modality: how it may work, and what its potential might be. Eur. J. Appl. Physiol 2010; 108:877-904. [PMID: 20012646]
- Matute-Llorente A, Gonzalez-Aguero A, Gomez-Cabello A, Vicente-Rodriguez G, Mallen JAC. Effect of Whole Body Vibration Therapy on Health Related Physical Fitness in Children and Adolescents with Disabilities: A Systematic Review. J Adolesc Health 2014; 54:385-396. [PMID: 24388109]
- Tankisheva E, Bogaerts A, Boonen S, Feys H, Verschueren S. Effects of Intensive Whole-Body Vibration Training on Muscle Strength and Balance in Adults with Chronic Stroke: A Randomized Controlled Pilot Study. Arch Phys Med Rehabil2014; 95:439-46. [PMID: 24067865]
- Johnson PK, Feland JB, Johnson AW, Mack GW, Mitchell UH. Effect of Whole Body Vibration on Skin Blood Flow and Nitric Oxide Production. J Diabetes SciTechnol2014; 8:889-894. [PMID: 24876449]
- Baum K, Votteler T, Schiab J. Efficiency of vibration exercise for glycemic control in type 2 diabetes patients. Int J Med Sci 2007; 4:159-163. [PMID: 17554399]
- Rittweger J, Ehrig J, Just K. Mutschelknauss M, Kirsch KA, Felsenberg D. Oxygen Uptake in Whole-Body Vibration Exercise: Influence of Vi bration Frequency, Amplitude, and External Load. Int J Sports Med 2002; 23:428-32. [PMID: 12215962]
- Lee NK, Sowa H, Hinoi E, Ferron M, Ahn JD, Confavreux C, et al. Endocrine regulation of energy metabolism by the skeleton. Cell 2007; 130:456-469. [PMID: 17693256]
- Burger EH, Klein-Nulen J. Responses of bone cells to biomechanical forces in vitro. Adv Dent Res 1999; 13:93-98. [PMID: 11276754]
- Nomura S, Takano-Yamamoto T. Molecular events caused by mechanical stress in bone. Matrix Biol 2000; 19:91-96. [PMID: 10842092]
- Fernandez-Real JM, Izquierdo M, Ortega F, Gorostiaga E, Gomez-Ambrosi J, Moreno-Navarrete JM, Frühbeck G, et al. The relationship of serum osteocalcin concentration to insulin secretion, sensitivity, and disposal with hypocaloric diet and resistance training. J ClinEndocrinolMetab 2009; 94:237-245. [PMID: 18854399]
- Alfonso-Rosa RM, del Pozo-Cruz J, del Pozo-Cruz B, Sanudo B, Abellan-Perpinan JM. Cost-utility analysis of a 12-week whole-body vibration based treatment for people with type 2 diabetes: reanalysis of a RCT in a primary care context. Public Health 2015; 129:993-995. [PMID: 25834930]
- Lin CI, Huang WC, Chen WC, Kan NW, Wei L, Chiu YS, Huang CC. Effect of whole-body vibration training on body composition, exercise performance, and biochemical responses in middle-aged mice. Metabolism 2015; 64:1146-56. [PMID: 26045298]
- Mozaffari MS, Baban B, Abdelsayed R, Liu JY, Wimborne H, Rodriguez N, Abebe W. Renal and glycemic effects of high-dose chromium picolinate in db/db mice: assessment of DNA damage. J NutrBiochem 2012; 23:977-985. [PMID: 21959055]
- Baban B, Liu JY, Mozaffari MS. Endoplasmic reticulum stress response and inflammatory cytokines in type 2 diabetic nephropathy: role of indoleamine 2,3-dioxygenase and programmed death-1. ExpMolPathol 2013; 94:343-351. [PMID: 23219834]
- González-Agüero A, Matute-Llorente A, Gómez-Cabello A, Casajus JA, Vicente-Rodriquez G. Effects of whole body vibration training on body composition in adolescents with Down syndrome. Res Dev Disabil 2013; 34:1426e33. [PMID: 23474995]
- Pitukcheewanont P, Safani D. Extremely low-level, short-term mechanical stimulation increases cancellous and cortical bone density and muscle mass of children with low bone density: A pilot study. Endocrinologist 2006;16:128e32.
- Söderpalm AC, Kroksmark AK, Magnusson P, Karlsson J, Tulinius M, Swolin-Eide D. Whole body vibration therapy in patients with Duchenne muscular dystrophy: A prospective observational study. J Musculoskelet Neuronal Interact 2013; 13:13e8. [PMID: 23445910]
- Ruck J, Chabot G, Rauch F. Vibration treatment in cerebral palsy: A randomized controlled pilot study. J Musculoskelet Neuronal Interact 2010; 10:77-83. [PMID: 20190383]
- Donath MY, Shoelson SE. Type 2 diabetes as an inflammatory disease. Nat Rev Immunol 2011; 11:98-107. [PMID: 21233852]
- Aarvak T, Chabaud M, Miossec P, Natvig JB. IL-17 is produced by some proinflammatory Th1/Th0 cells but not by Th2 cells. J Immunol 1999; 162:1246-1251. [PMID: 21233852]
- Zhang L, Zhao Y. The regulation of Foxp3 expression in regulatory CD4(+)CD25(+)T cells: multiple pathways on the road. J Cell Physiol 2007; 211:590-597. [PMID: 17311282]
- Kuo LJ, Yang LX. Gamma-H2AX - a novel biomarker for DNA double-strand breaks. In Vivo 2008; 22:305-309. [PMID: 18610740]
- Li YF, Burrows N, Gregg E, Geiss L. Declining trends in hospitalizations for non-traumatic lower extremity amputation in the diabetic population: United States, 1988-2006. Diabetes 2010; 59:A50.
- Yoosefinejad AK, Shadmehr A, Olyaei G, Talebian S, Bagheri H, Mohajeri-Tehrani MR. Short-term effects of the whole-body vibration on the balance and muscle strength of type 2 diabetic patients with peripheral neuropathy: a quasi-randomized-controlled trial study. J Diabetes MetabDisord 2015;14:45. [PMID: 26052508]
- Weinheimer-Haus EM, Judex S, Ennis WJ, Koh TJ. Low-Intensity Vibration Improves Angiogenesis and Wound Healing in Diabetic Mice. PLoS One 2014; 9:1-8. [PMID: 24618702]
- Blakytny R, Jude E. The molecular biology of chronic wounds and delayed healing in diabetes. Diabet Med 2006; 23:594–608. [PMID: 16759300]

