Keywords
Bone Diseases, Metabolic; Exocrine Pancreatic Insufficiency; Osteoporosis; Pancreatitis, Chronic
Abbreviations
PEI Pancreatic exocrine insufficiency DXA Dual-energy X-ray absorption PERT Pancreatic enzyme replacement therapy TSH Thyroid-stimulating hormone
INTRODUCTION
In chronic pancreatitis, progressive ongoing inflammation destroys the exocrine pancreatic tissue and produces pancreatic exocrine insufficiency. Because the pancreas has a large functional reserve capacity, the effects of this destruction of exocrine pancreatic tissue becomes clinically apparent only after about 90% of the acinar parenchyma has been lost [1]. The severe decrease in secretion of digestive enzymes means that patients lose the ability to absorb macronutrients adequately. This has a negative impact on the absorption of trace elements and vitamins as well, especially the fat-soluble vitamins (A, D, E, K). Deficiencies of essential nutrients increase health risks and produce serious symptoms. Vitamin D (cholecalciferol) deficiency has attracted attention because it increases the risk of impaired bone metabolism that can lead to decreased bone mineral density and subsequent bone disorders, such as osteopenia and osteoporosis. Guideline recommendations have been published for managing the decrease in vitamin D absorption seen in other gastrointestinal diseases associated with malabsorption, such as Crohn’s disease, celiac disease, and cystic fibrosis [2]. While there are recommendations related to vitamin D in the current guidelines for management of chronic pancreatitis [3-6], prospective studies are need to evaluate the extent of the problem and determine the effectiveness of different treatment strategies.
The current prospective study investigated bone mass and bone metabolism in a well-defined group of patients with chronic pancreatitis who had varying degrees of pancreatic exocrine insufficiency.
PATIENTS AND METHODS
In this prospective cohort study, a total of 50 male patients with confirmed chronic pancreatitis were recruited from the pancreas outpatient clinic. The diagnosis of chronic pancreatitis was based on clinical symptoms and morphology (imaging). Pancreatic function was evaluated using the fecal elastase-1 test as described previously [7]. Only male patients were recruited in order to avoid the hormonal variations found in women and the effects these variations could have on bone metabolism. Patients with other malabsorption conditions (e.g. celiac disease, Crohn’s disease) or other diseases known to affect bone metabolism (e.g. kidney disease, hyperparathyroidism, rheumatoid arthritis) were excluded from the study. Patients taking drugs known to influence bone metabolism (e.g. steroids or hormone therapy for prostate cancer) were also excluded. The study was approved by the local ethics committee. All patients gave informed consent prior to inclusion in the study.
Clinical Data
Were collected concerning alcohol intake, smoking, and other life style factors. Alcohol intake was assessed with the self-reported alcohol intake questionnaire (SRAI) [8]. Patient history of previous injuries, particularly broken bones, was recorded. Current and previous medications were recorded, especially pancreatic enzymes. A standardized questionnaire for osteoporosis was given [9].
Laboratory Parameters
Laboratory parameters were measured in samples obtained during routine blood draws. Pancreatitis was assessed through measurement of white blood cell counts, C-reactive protein, amylase, and lipase. Total protein, albumin, and vitamin K were measured to assess nutritional status. Endocrine status was evaluated by measuring parathyroid hormone, thyroid-stimulating hormone (TSH), and testosterone. Bone metabolism was assessed through measurement of serum calcium, phosphate, bonespecific alkaline phosphatase, and 25-OH-cholecalciferol. Calcium and deoxypyridinoline were determined in 24h urine samples.
Bone Density
It was determined using dual-energy X-ray absorption (DXA; QDR-1000, Hologic Instruments) at the standard measurement sites in the lumbar spine and the femur. Results are presented as T scores and Z scores as previously described [10]. Classification of bone density was done according to the WHO standard [11]. Patients were advised about the added radiation risk when asked to volunteer to undergo conventional vertebral X-rays. All of the patients who were asked agreed to the X-rays. The BMD on the conventional X-ray was graded semi-quantitatively, as described: normal = 0, mild = 1, moderate = 2, and severe = 3. Once a reduction is clearly seen, this can be considered already substantial (scored 2) [12]. Complete demineralisation, i.e. osteoporosis was scored 3.
Statistical Analysis
It was done using SPSS software (version 10.0). U tests were used for two independent analytes. The Kruskal-Wallis test was used for more than two independent analytes. Values are reported as medians ± standard deviation. P<0.05 was considered statistically significant.
RESULTS
Patient Characteristics
Alcohol abuse (SRAI 25 – 900 g/day) was identified in 36 of the 50 patients. Forty-two patients were smokers (5-70 pack years) (Table 1). Twenty-eight patients met the criterion for pancreatic exocrine insufficiency (fecal elastase < 200 μg/g) and were receiving pancreatic enzyme replacement therapy (PERT) (Tables 1 and 2). Patient BMI values were between 15-35 kg/m2 (<20: n=10; 20-25: n=32; >25: n=8). The duration of chronic pancreatitis was 1-23 years (median: 12).
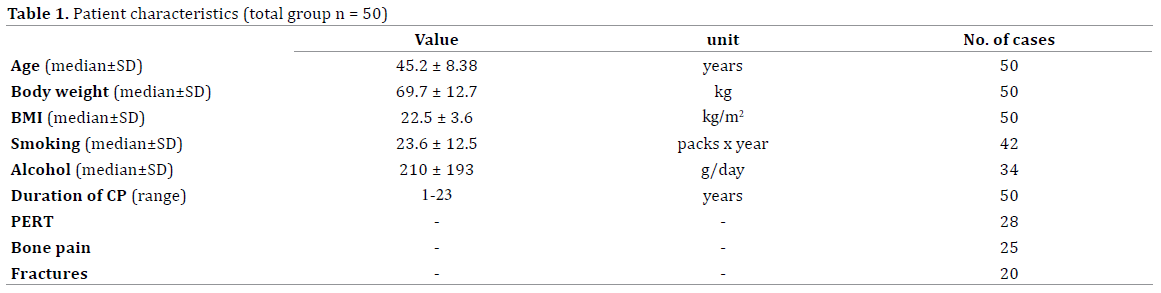

Half of the patients reported regular pain in the bones. Twenty patients reported fractures in response to low trauma [13]. One patient also reported a fracture without trauma.
Bone Metabolism
Urine calcium, deoxypyridinoline, and vitamin D (25-OH cholecalciferol) were significantly decreased whereas serum calcium, phosphate, bone-specific alkaline phosphatase, and parathyroid hormone were normal (Table 2). Nutritional parameters were also normal for the entire group.
Pancreatic Function
In relation to bone metabolism. There was no correlation between three classes of fecal elastase-1 (< 100 μg/g: n = 22; 100-200 μg/g: n = 8; > 200 μg/g: n = 17) and serum calcium, 25-OH-cholecalciferol, or deoxypyridinoline (Figure 1).
Figure 1. Bone mineral density (BMD), as measured by conventional X-ray, in correlation with fecal elastase-1 (FE-1). BMD 0 = normal, 1 = mild, 2 =
moderate, 3 = severe (complete demineralization)[11, 12]. Note that datapoints can be superimposed.
Bone Density
Fifteen patients underwent DXA. The median T score was -1.1. Five patients had normal bone density (T score > -1), nine had osteopenia (T score -1 to – 2.5), and one patient had osteoporosis (T score < -2.5) (Table 3). There was a trend toward a correlation between patients with low fecal elastase-1 and low T scores (p = 0.065). When patients receiving PERT (n = 9) were compared to those not receiving enzymes (n = 5), the patients receiving PERT had significantly higher DXA scores (-0.80 ± 0.6 vs. -1.51 ± 0.55; p < 0.05).

Conventional vertebral X-rays showed normal bone mineral density (BMD) in 3 of the 42 patients tested, mildly-reduced density in 32, moderately-reduced density in 6, and severely-reduced density with a fracture in one patient. All ten patients whose bone density was assessed as reduced by DXA also had assessments of reduced BMD by conventional X-ray. Reduced BMD measurement by conventional X-ray correlated with low fecal elastase-1 (p < 0.05; Figure 1). Patients who had fecal elastase-1 concentrations greater than 200 μg/g FE-1 (394 ± 99) had DXA scores of -0.44 ± 0.2 and X-ray BMD scores of 0.93 ± 0.23 in contrast to patients with pancreatic exocrine insufficiency (FE-1 < 200 μg/g; 38 ± 48), who had DXA scores of -1.76 ± 0.5 and X-ray BMD scores of 1.2 ± 0.31 (p = 0.04 for FE-1 and BMD scores).
DISCUSSION
Normal bone mineral density and bone metabolism require adequate concentrations of vitamin D. The absorption of vitamin D in turn depends on the uptake of lipids, something that can only occur if sufficient pancreatic enzymes are available at the right time and place in the intestine [14]. In the current study, a significant decrease was seen in serum vitamin D (25-OH cholecalciferol), along with a significant increase in deoxypyridinoline in urine. Bone mineral density was reduced in the majority of patients with chronic pancreatitis. There was a correlation between pancreatic exocrine function and bone mineral density (Figure 1).
The current study differs from previous studies in that it is the only prospective study in males. Only male patients were recruited in order to avoid the hormonal variations found in women. Concern about hormonal variations and associated effects on bone metabolism was raised in a study that included both women and men with PEI due to cystic fibrosis [15]. However, in a more recent study no differences were found between male and female patients [16]. The results of the current prospective study are consistent with the significant decrease in bone mineral density seen in other European and non-European cohorts using DXA [10, 17] and conventional X-ray [17]. Vitamin D deficiency has been found in a number of studies of patients with chronic pancreatitis [10, 15, 17]. Some studies found a correlation between PEI and decreased BMD [18] but did not find a correlation between vitamin D levels or supplementation and decreased BMD [16, 17-19]. Haaber and colleagues did not find significant differences in BMD between pancreatitis patients with and without PEI [10], however, BMD as measured with DXA was significantly lower in the PEI group, as in our study. The percentage of patients with decreased bone mineral density (osteopathy) ranged from 34% to 100% in previous studies (Table 4) and did correlate with the severity of chronic pancreatitis in at least one study [18]. Although DXA is routinely used in endocrinology and is considered the gold standard for assessing reduction of bone mineral density, the current study showed that conventional X-ray, which is more accessible, may be sufficient. The fact that osteopathy is common in older cystic fibrosis patients has been firmly established [2], but osteopathy in chronic pancreatitis has only recently begun to receive attention.

The way clinicians and investigators view pancreatic exocrine insufficiency has been changing. Elegant studies using the C13 mixed-triglyceride breath test have made it clear that malnutrition persists even after the symptoms of chronic pancreatitis-induced pancreatic exocrine insufficiency have been treated [20]. (Persistent) nutritional deficiency can be measured easily by using serum parameters such as prealbumin, vitamin D, retinol binding protein, zinc and magnesium [21]. Although we could correlate low fecal elastase-1 to low bone mineral density, in our patients, in our study, nutritional parameters were remarkably normal. However, we did not measure all of the recommended parameters and the majority of our patients was on pancreatic enzyme replacement therapy.
Fecal elastase-1 is not helpful in detecting mild to moderate pancreatic exocrine insufficiency [7]. However, according to published guidelines, a fecal elastase-1 value below 200 μg/g is considered reliable in establishing the diagnosis of PEI [3-6]. A very low level of fecal elastase-1 can, therefore, be considered to be a valid indication of pancreatic exocrine insufficiency [22, 23]. In agreement with the current study, several previous investigations have shown a link between significant secondary disease, osteoporosis (decreased bone mineral density), nutritional deficiency (low vitamin D), and pancreatic exocrine insufficiency (low fecal elastase-1). A recent systematic review showed that one out of four patients with chronic pancreatitis had osteoporosis and two-thirds had either osteoporosis or osteopenia [24] (Table 4). As a result, these patients had a high prevalence of low-trauma fractures, and their risk of fracture was greater than that seen in patients with Crohn’s disease [13].
The treatment of pancreatic exocrine insufficiency should aim to correct malnutrition and prevent secondary damage outside the pancreas. Rather than simply relieve symptoms. A prospective cohort study is needed to determine whether intervention that corrects pancreatic exocrine insufficiency results in an improvement of osteopathy in patients with chronic pancreatitis.
Acknowledgement
The authors thank Margery Herrington, PhD, for reading the manuscript and helpful advice.
Conflict of Interest
There are no conflicts of interest to declare.
References
- DiMagno EP, Malagelada JR, Taylor WF, et al. A prospective comparison of current diagnostic tests for pancreatic cancer. N Engl J Med 1977; 297: 737-42. [PMID: 895803]
- Parkins MD, Parkins VM, Rendall JC, et al. Changing epidemiology and clinical issues arising in an ageing cystic fibrosis population. Therapeutic advances in respiratory disease 2011; 5: 105-19. [PMID: 21078692]
- Hoffmeister A, Mayerle J, Beglinger C, et al. S3-Leitlinie ChronischePankreatitis: Definition, Ätiologie, Diagnostik, konservative, interventionellendoskopische und operative Therapie der chronischenPankreatitis. Leitlinie der DeutschenGesellschaftfürVerdauungs- und Stoffwechselkrankheiten (DGVS). Z Gastroenterol 2012; 50: 1176-1224.
- Toouli J, Biankin AV, Oliver MR, et al. Management of pancreatic exocrine insufficiency: Australasian Pancreatic Club recommendations. The Medical Journal of Australia 2010; 193: 461-7. [PMID: 20955123]
- Frulloni L, Falconi M, Gabbrielli A, et al. Italian consensus guidelines for chronic pancreatitis. Digestive and Liver Disease 2010; 42 Suppl 6: S381-406. [PMID: 21078490]
- Martinez J, Abad-Gonzalez A, Aparicio JR, et al. The Spanish Pancreatic Club recommendations for the diagnosis and treatment of chronic pancreatitis: part 1 (diagnosis). Pancreatology 2013; 13: 8-17. [PMID: 23395565]
- Lankisch PG, Schmidt I, Konig H, et al. Faecalelastase 1: not helpful in diagnosing chronic pancreatitis associated with mild to moderate exocrine pancreatic insufficiency. Gut 1998; 42: 551-4. [PMID: 9616319]
- Parker DR, Derby CA, Usner DW, et al. Self-reported alcohol intake using two different question formats in southeastern New England. International Journal of Epidemiology 1996; 25: 770-4. [PMID: 8921455]
- Schroder G, Knauerhase A, Kundt G, et al. Effects of physical therapy on quality of life in osteoporosis patients - a randomized clinical trial. Health Qual Life Outcomes 2012; 10: 101. [PMID: 22920839]
- Haaber AB, Rosenfalck AM, Hansen B, et al. Bone mineral metabolism, bone mineral density, and body composition in patients with chronic pancreatitis and pancreatic exocrine insufficiency. International Journal of Pancreatology 2000; 27: 21-7. [PMID: 10811020]
- Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser 1994; 843: 1-129. [PMID: 7941614]
- Jergas M, Uffmann M, Escher H, et al. Interobserver variation in the detection of osteopenia by radiography and comparison with dual X-ray absorptiometry of the lumbar spine. Skeletal Radiol 1994; 23: 195-9. [PMID: 8016671]
- Tignor AS, Wu BU, Whitlock TL, et al. High prevalence of low-trauma fracture in chronic pancreatitis. The American Journal of Gastroenterology 2010; 105: 2680-6. [PMID: 20736937]
- Keller J, Layer P. Human pancreatic exocrine response to nutrients in health and disease. Gut 2005; 54 Suppl 6:vi1-28. [PMC: 1867805]
- Moran CE, Sosa EG, Martinez SM, et al. Bone mineral density in patients with pancreatic insufficiency and steatorrhea. The American Journal of Gastroenterology 1997; 92: 867-71. [PMID: 9149203]
- Duggan SN, O'Sullivan M, Hamilton S, et al. Patients with chronic pancreatitis are at increased risk for osteoporosis. Pancreas 2012; 41: 1119-24. [PMID: 22836855]
- Sudeep K, Chacko A, Thomas N, et al. Predictors of osteodystrophy in patients with chronic nonalcoholic pancreatitis with or without diabetes. Endocrine Practice 2011; 17: 897-905. [PMID: 21742614]
- Mann ST, Stracke H, Lange U, et al. Alterations of bone mineral density and bone metabolism in patients with various grades of chronic pancreatitis. Metabolism: clinical and experimental 2003; 52: 579-85. 19. Sikkens EC, Cahen DL, Koch AD, et al. The prevalence of fat-soluble vitamin deficiencies and a decreased bone mass in patients with chronic pancreatitis. Pancreatology 2013; 13: 238-42. [PMID: 23719594]
- Sikkens EC, Cahen DL, Koch AD, et al. The prevalence of fat-soluble
vitamin deficiencies and a decreased bone mass in patients with chronic
pancreatitis. Pancreatology 2013; 13: 238-42. [PMID: 23719594]
- Dominguez-Munoz JE, Iglesias-Garcia J, Vilarino-Insua M, et al.
13C-mixed triglyceride breath test to assess oral enzyme substitution
therapy in patients with chronic pancreatitis. Clin Gastroenterol Hepatol
2007; 5: 484-8. [PMID: 17445754]
- Lindkvist B, Dominguez-Munoz JE, Luaces-Regueira M, et al. Serum
nutritional markers for prediction of pancreatic exocrine insufficiency in
chronic pancreatitis. Pancreatology 2012; 12: 305-10. [PMID: 22898630]
- Benini L, Amodio A, Campagnola P, et al. Fecal elastase-1 is useful
in the detection of steatorrhea in patients with pancreatic diseases but
not after pancreatic resection. Pancreatology 2013; 13: 38-42. [PMID:
23395568]
- Löhr JM, Oliver MR, Frulloni L. Synopsis of recent guidelines on
pancreatic exocrine insufficiency. United European Gastroenterology
Journal 2013; 1: 79-83. [PMID: 24917944]
- Duggan SN, Smyth ND, Murphy A, et al. High prevalence of osteoporosis
in patients with chronic pancreatitis: a systematic review and metaanalysis.
Clin Gastroenterol Hepatol 2014; 12: 219-28. [PMID: 23856359]
- Dujsikova H, Dite P, Tomandl J, et al. Occurrence of metabolic
osteopathy in patients with chronic pancreatitis. Pancreatology 2008; 8: 583-6. [PMID: 18824882]


