Keywords
Adenocarcinoma; Cell Proliferation; Neoplasms; Histology
Abbreviations
AgNOR: argyrophilic nucleolar organizer region; NOR: nucleolar organizer region; PCNA: proliferating cell nuclear antigen; PCNALI: proliferating cell nuclear antigen labeling index; SAPA: subjective AgNOR pattern assessment
INTRODUCTION
Various clinical and histological parameters are available for assessing the biological aggressiveness of the tumor. Clinical parameters are tumor size, lymph node involvement and distant metastases while the histological parameters are degree of pleomorphism, mitotic figure, lymphoreticular response, desmoplasia, tumor necrosis, lymphatic or vascular invasion and grade of tumor. Besides these parameters, DNA content, S phase fraction, oncogenes, Ki-67 monoclonal antibodies, PCNA (proliferating cell nuclear antigen), fibroblast growth factor receptor and AgNOR (argyrophilic nucleolar organizer regions) are some other parameters. The AgNOR is a cheap, simple, quick and reliable adjuvant to routine histopathology [1]. Its role is well-established in the diagnosis of lymphoma [2], breast cancer [3, 4], prostatic tumors [5], oral cavity tumors [6] and other tumors [7]. The AgNOR has been studied in pancreatic tumors but only a few studies are available [8, 9, 10]. The aim of this study was to study the AgNOR count and the SAPA (subjective AgNOR pattern assessment) score in carcinoma of the head of the pancreas including periampullary tumors and to correlate them with various clinicohistological parameters.
PATIENTS
The study was carried out on 24 patients admitted to our University Hospital with carcinoma of the pancreatic head (including periampullary tumors), who underwent Whipple’s pancreaticoduodenectomy for curative resection. The mean age of the patients was 54 years (range 44-68 years); 20 patients (83.3%) were males and 4 (16.7%) were females. Healthy pancreases were taken for study from the resected specimens of the pancreases; the area chosen was that which was considered to be healthy on histological examination and the AgNOR was studied as a control using this healthy tissue.
METHODS
Detailed clinical examination was carried out and findings were recorded. After resection, the tissue was fixed in formalin and embedded in paraffin wax. The slides were processed both for routine H&E staining and AgNOR staining.
AgNOR Staining
Formalin-fixed paraffin-embedded sections (4-6 mm thickness) were rinsed in xylene for 5-10 minutes three times, in ethanol (100%) for 2-5 minutes three times, then in ethanol (70%) for 2-5 minutes once. The slides were washed in running tap water for 5 minutes and were then rinsed in deionized water for 2- 3 minutes 2-3 times. The slides were incubated with 1 volume of solution A and 2 volumes of Solution B per slide. The slides were left in the dark for 60 minutes and rinsed in deionized water three times; they were then washed with 5% sodium thiosulfate solution for 5 minutes. In addition, the slides were rinsed in ethanol (100%) and xylene, and the smears were mounted with a cover slip.
Solution A (Colloid Developer Solution)
Solution A contained 100 mL of pure water, plus 2 g of gelatin, plus 1 mL formic acid. The gelatin was dissolved at 40-60°C by stirring for 10-20 minutes. This solution can be left at room temperature or at 4°C for several months.
Solution B
Solution B contained 100 mL of pure water, plus 50 g of silver nitrate. This solution has to be stored in the dark by wrapping aluminum foil around the container.
Counting of AgNOR and SAPA Score
Silver-stained slides were examined under a light microscope at 500x magnification. AgNORs appear as brown or black dots within a yellowish background of nucleus. The brown/black dots were counted in the nucleolus and also outside the nucleolus in the nucleus. The clumped dots were considered to be a single dot. The number of dots was counted in 100 cells and the average was taken for each case. The area for counting was from the periphery of the tumor and from the areas where maximum dots were visible.
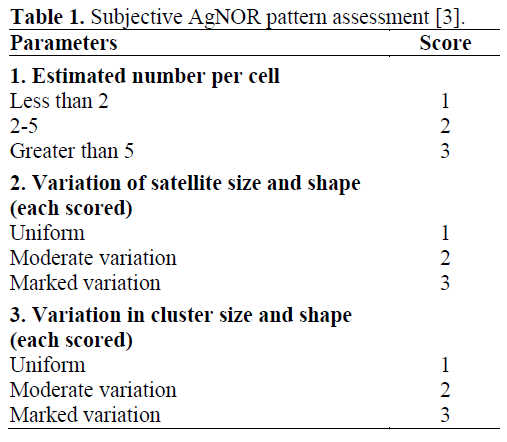
Subjective AgNOR pattern assessment scoring was done according to the scoring system proposed by Meehan et al. [3] (Table 1). Scores were assigned by the estimated number of dots, the size and shape of dots and clusters and their variation from cell to cell. For each unit, there are 5 parameters: estimated number per cell, variation of satellite size, variation of satellite shape, variation in cluster size and variation in cluster shape. Using this subjective system, the score can range from 5 to 15.
ETHICS
Written informed consent was obtained from all patients and the study protocol conformed to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004, as reflected in a priori approval by the appropriate institutional review committee.
STATISTICS
Data are reported as mean values and standard deviations. For statistical analysis, the oneway ANOVA was applied by using the posthoc Student Newman Keuls (SNK) procedure. Statistical analyses were performed by running the SPSS Version 11.0 package.
RESULTS
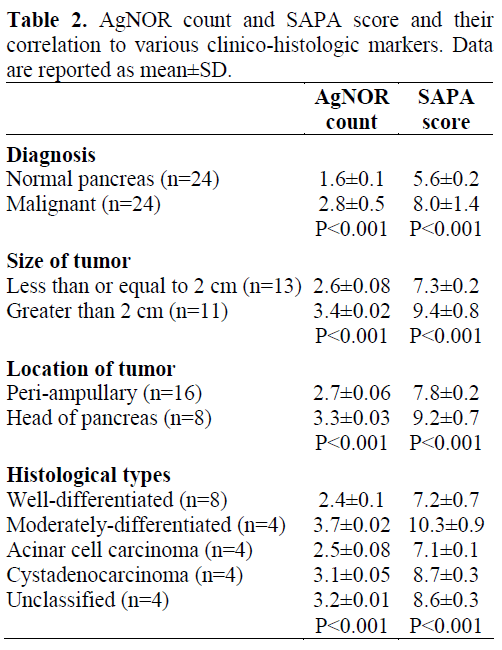
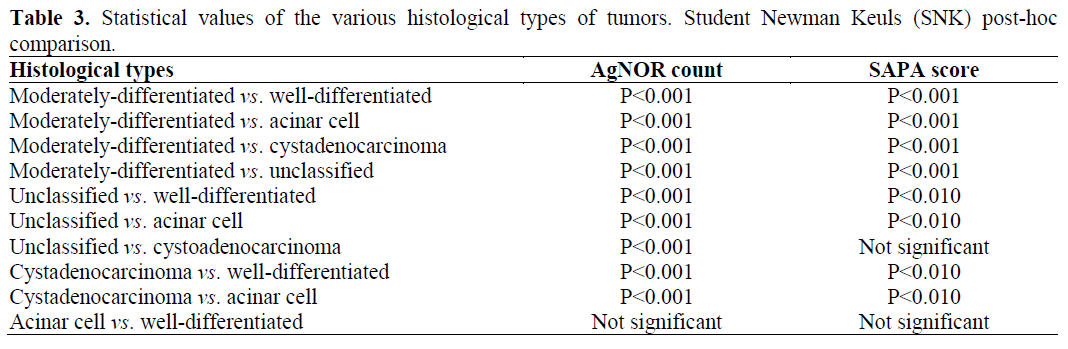
Sixteen patients had periampullary carcinoma while 8 patients had carcinoma of the head of the pancreas. The H&E stain was done specifically to see the type and the grade of tumor. Silver staining was done for the healthy-looking pancreas in the specimen and that was compared with the malignant area. The values of the AgNOR count and the SAPA score were significantly higher in malignant lesions as compared to the healthy pancreas (Table 2). On comparing the tumors less than or equal to 2 cm with those greater than 2 cm in size, there was a significant difference in both the AgNOR count and the SAPA score (P<0.001). According to the type of tumor (periampullary vs. carcinoma of the head of the pancreas), there was a significant difference (P<0.001) in the values of the AgNOR count and the SAPA score suggesting a relatively lower proliferative activity of the periampullary carcinoma; however, it is also true that most of the cases of periampullary carcinoma (10/16; 62.5%) were less than 2 cm in size. Of the 24 cases, 8 (33.3%) were well-differentiated duct cell carcinomas, 4 (16.7%) moderatelydifferentiated carcinomas, 4 (16.7%) acinar cell carcinomas, 4 (16.7%) cystadenocarcinomas and 4 (16.7%) were unclassified types. The AgNOR count and the SAPA score were significantly different among the different histological types (P<0.001). Welldifferentiated carcinomas had a significantly lower AgNOR count as compared to other types of tumors except acinar cell carcinomas since acinar cell carcinoma is also a welldifferentiated tumor. The SAPA score was also highest in moderately-differentiated tumors, and the difference between moderately-differentiated tumors and other types was significant although there were no significant differences between cystadenocarcinomas and unclassified tumors, and between acinar cell carcinomas and welldifferentiated tumors (Table 3).
DISCUSSION
Nucleolar organizer regions (NORs) are the tools used by the cytogeneticist for the study of chromosomal disorders. It was noticed that NOR patterns in malignancy are different, and after the development of the simple silver staining technique for the visualization of NORs at the optical level, it was decided that a NOR study using silver staining can be used for characterizing malignancy. The number of AgNORs, their size and heterogeneity represents proliferative cellular activity, thus, it can be used for detecting malignancy and grading of the tumor. Moreover, this technique is very simple and does not require special preservation or fixation of tissue. It can be performed on formalin-fixed paraffinembedded sections which is routine for the histopathologist. The AgNOR staining procedure is also simple and does not require any special instruments or costly reagents. In the absence of a histopathologist, AgNOR evaluation can also be done by an expert technician. Therefore, at centers where more costly methods are not available for assessing tumor aggressiveness, the study of the AgNOR may become an important parameter in order to study the aggressiveness of the disease.
In applying the AgNOR technique to tumor pathology, the AgNOR counting method appears to be important. In a study of breast lesions, the number of AgNOR clusters per nucleus, the mean number of AgNORs per cluster and the number of satellite AgNORs were evaluated in order to finally derive a total AgNOR count [11]. In a study of cytological preparations of breast lesions, a subjective AgNOR pattern assessment scoring system was developed in which scores were assigned by the estimated number of dots, the size and shape of the dots as well as clusters and their variation from cell to cell [3]. In the present study, both methods of AgNOR counting and the subjective AgNOR pattern assessment (SAPA) score were studied.
In the present study, we have tried to determine the usefulness of the AgNOR count and the SAPA score as per the various clinico-histological parameters. A total of 24 cases were studied; since only early stage tumors were resected, the value of the AgNOR could not be correlated with the lymph node status and patients with metastasis. But the correlation of the AgNOR was carried out using the size of the tumor, the type of tumor and histological grade. Our mean value for AgNORs in a healthy pancreas was 1.6±0.1 which is comparable to 1.8 with other studies [12] and the mean SAPA score for a healthy pancreas was 5.6±0.2. In malignant pancreatic lesions, the AgNOR count was 2.8±0.5 and the SAPA score was 8.0±1.4. By comparing a healthy pancreas with a malignant lesion, both the AgNOR count and the SAPA score showed significant differences. The AgNOR count and the SAPA score were significantly elevated in malignant lesions of the pancreas irrespective of the histological type. The AgNOR and the SAPA score could be correlated with the size of the tumor, type of tumor and grade of tumor. Toyota et al. [13] from Japan analyzed 38 patients with invasive ductal carcinoma and found a mean score of 3.8±0.6 in malignant tumors as compared to 1.7±0.3 in healthy pancreases; they also found that survival could be matched with the AgNOR count. Similarly, another study from Japan found the mean AgNOR count to be 1.9±0.4 in healthy pancreases, 2.1±0.5 in pancreatitis and 4.0±1.2 in malignant tissue [14].
Various authors have used the AgNOR count as a marker of proliferation in various experimental animals with pancreatic lesions [12]. Pollock [8] studied the diagnostic value and cytophysiologic correlation of NORs in the exocrine pancreas, in chronic pancreatitis and ductal adenocarcinoma, and concluded that AgNORs could differentiate between chronic pancreatitis and adenocarcinoma, and between different grades of adenocarcinoma. A correlation was also found between the number of extra-nucleolar dots and proliferation, as well as between the number of intranucleolar dots and the protein synthetic activity of the epithelial cells of the small excretory ducts of the pancreas.
Schulz [9] studied the relationship between chronic pancreatitis and the development of cancer in 16% of cases depending on the length of history, and found the point mutation of the K-ras gene, mutation or deletion of the p53 gene and an excess production of the c-erbB-2 gene to be present to a greater extent in pancreatic carcinomas. Suzuki et al. [15] compared p53, proliferating cell nuclear antigen expression and AgNORs in pancreatic duct cell carcinomas using immunohistochemical studies. Three histological indicators of malignancy were studied: tumor stage, histological grade, and lymph node status. p53 overexpression was correlated to the histological grading but not to tumor stage and lymph node involvement; the proliferating cell nuclear antigen labeling index (PCNALI) was correlated to histological malignant grading and the pathological state but was not correlated with lymph node status. Thus, expression of p53 and PCNALI do not reflect the degree of malignant development. In contrast, the AgNOR number showed significant correlation with these three indicators of malignancy in pancreatic duct cell adenocarcinoma. Thus, AgNOR is a better marker of malignant changes in pancreatic duct cell adenocarcinoma. Sato et al. [10] were able to differentiate neoplastic from atypical non-neoplastic lesions of the pancreas based on nucleolar and dispersed nucleolar organizer regions. AgNORs have been used as markers of malignancy in endocrine tumors of the pancreas [12].
We were able to correlate the AgNOR count and the SAPA score with the size of the tumor, the type of tumor and the histological grade of tumor. A large scale study is contemplated to determine more exactly the
References
- Khanna AK, Tokuda Y, Tajima T, Mitomi T, Shibuya.M, Osamura Y. Prognostic parameters in axillary node negative breast cancer. Tokai J ExpClin Med 1993; 18:17-27. [PMID 7940603]
- Crocker J, Egan MJ. Correlation between NOR sizes and numbers in non-Hodgkins lymphomas. J Pathol 1988; 156:233-9. [PMID 3060577]
- Meehan SM, Magee H, Carney DN, Dervan PA. The diagnostic value of silver nucleolar organizer region assessment in breast cytology. Am J ClinPathol 1994; 101:689-93. [PMID 7516117]
- Khanna AK, Ansari MA, Kumar M, Khanna A. Correlation between AgNOR count and subjective AgNOR pattern assessment score in cytology and histology of breast lumps. Anal Quant CytolHistol 2001; 23:388-94. [PMID 11777272]
- Contractor H, Ruschoff J, Hanisch T, Ulshofer B, Neumann K, Schultze-Seemann W, Thomas C. Silver stained structures in prostatic carcinoma: evaluation ofdiagnostic and prognostic relevance by automatedimage analysis. UrolInt 1991; 46:9-14. [PMID1708924]
- Khanna AK, Datta G, Kumar M. Correlation of AgNOR with tumor size, stage of tumor, lymphnode status and grade of tumor in oral cancer. In: Verma AK, ed. Oral Oncology IV B. Bangalore, India: MacMillan India, 1995:25-30.
- Khanna AK GiriAK ,Khanna A, Kumar M. Nucleolar organizer region count and subjective AgNOR pattern assessment (SAPA) score in skin tumors. J SurgOncol 2001; 78:273-8. [PMID 11745824]
- Pollok A. Nucleolar organizer regions in exocrine pancreas in chronic pancreatitis and ductal adenocarcinoma. Diagnostic value and cytophysiologic correlate. Gen DiagnPathol 1997; 142:199-209. [PMID 9065584]
- Schulz HJ. Lesions of the pancreatic duct epithelium and histogenesis of exocrine pancreatic carcinomas. ZetralblPathol 1994; 140:203-10. [PMID 7947629]
- Sato M, Watanabe H, Ajioka Y, Noda Y, Sakai Y. Nucleolar and dispersed nucleolarorganiser regions (NORs) in differentiating neoplastic from atypical nonneoplastic lesions of the pancreas. GastroenterolJpn 1993; 28:72-80. [PMID 8382641]
- Smith R, Crocker J. Evaluation of nucleolar organizer region: associated proteins in breast malignancy. Histopathology 1988; 12:113-25. [PMID 2452777]
- Ruschoff J, Willemer S, Brunzel M, Trautmann ME, Frank M, Arnold R, Kloppel G. Nucleolar organizer regions and glycoprotein hormone alpha chain reaction as markers of malignancy in endocrine tumors of pancreas. Histopathology 1993; 22:51-7. [PMID 7679659]
- Toyota N, Katano K, Tokahashi S, Ohtani S, Mizusawa K, Hamazoe R, Kaibara N. The argyrophilic nuclear organizer region (Ag-NOR) score in invasive ductal carcinoma of the pancreas. Surg Today 1997; 27:414-9. [PMID 9130343]
- Aimoto T, Onda M, Uchida E, Asano G. Study on proliferative potential by AgNORs staining in human pancreatic carcinoma. Nippon GekaGakkiZasshi 1993; 94:78-85. [PMID 8437556]
- Suzuki T, Takano Y. Comparative immunohistochemical studies of p53 and proliferating cell nuclear antigen and argyrophilicnucleolar organizer regions in pancreatic ductal carcinoma. Jpn J Cancer Res 1993; 84:1072-7. [PMID 7901190]

