Keywords
Carcinoma; Drug Therapy; gemcitabine; Neoplasm Metastasis; Pancreas; Pancreatic Neoplasms; Therapeutics
Abbreviations
CONKO: Charité Onkologie Clinical; EORTC: European Organization of Research and Treatment of Cancer; ESPAC: European Study Group for Pancreatic Cancer; FOLFIRINOX; 5-fluorouracil, oxaliplatin, irinotecan, leucovorin; GITSG: Gastrointestinal Study Group; JASPAC: Japanese Adjuvant Study Group of Pancreatic Cancer; hENT1: human equilibrative nucleoside transporter 1; LEAP: Low hENT1 and Adenocarcinoma of the Pancreas; RTOG: Radiation Therapy Oncology Group; SPARC: secreted protein acidic and rich in cysteine
INTRODUCTION
Pancreatic adenocarcinoma remains a treatmentrefractory cancer. Management of pancreatic cancer remains the most challenging task in oncology. The American Cancer Society’s estimates for pancreatic cancer in the United States for 2013 are [1]:
• About 45,220 people (22,740 men and 22,480 women) will be diagnosed with pancreatic cancer;
• About 38,460 people (19,480 men and 18,980 women) will die of pancreatic cancer.
Rates of pancreatic cancer have been slowly increasing over the past 10 years. The lifetime risk of developing pancreatic cancer is about 1 in 71 (1.41%). A person’s risk may be altered by certain risk factors.
Though pancreatic cancer represents only 2-3% of all cancers, it is the most lethal one accounting for the 6% of all cancer-related mortality. It remains the 4th cause of cancer-related death after lung, prostate (breast in women) and colorectal cancer since 1970s in the U.S.A. in spite of tremendous effort from clinical and experimental points. Its aggressive features include insidious presentation, unresectability due to early involvement of major vessels, debilitating symptoms at late stage, and de novo chemo-resistance.
The discouraging features of this disease did not retard the effort of investigating the disease mechanism and development of newer agents. Extensive research in the past two decades has revealed that pancreatic cancer is a genetic disease involving multiple levels of abnormalities. The interest in conquering pancreatic cancer is apparently global, from cellular biology to molecular biology, from surgery to medicine, from orthodox approaches to alternative ways. We gladly saw over 75 abstracts presented in the 2013 ASCO Gastrointestinal Cancers Symposium at San Francisco in the field of pancreatic cancer. In this editorial, I will focus on the management of pancreatic cancer in all stages.
Adjuvant Therapy of Resected Pancreatic Cancer
Substantial controversy remains regarding the optimal adjuvant treatment for patients with resectable pancreatic adenocarcinoma. Despite improvements in radiation techniques, systemic therapies, and incorporation of targeted agents, the 5-year survival rate for early stage patients remains less than 25% and the optimal adjuvant treatment approach remains unclear. The relative value of the addition of adjuvant radiation to chemotherapy is the issue of some debate as mixed data regarding adjuvant therapy for patients with early stage pancreas cancer. Current accepted standard of care is adjuvant gemcitabine following curative resection, but there have been no conclusions regarding the role or timing of adjuvant chemoradiation [2]. Although systemic disease represents the major risk for failure following resection, there are patients who would benefit from adjuvant local therapy that remain difficult to identify at present. Four randomized controlled trials investigated the role of adjuvant chemoradiation in resected pancreatic cancer:
• The Gastrointestinal Study Group (GITSG) study showed a survival benefit in patients who received bolus 5-FU with radiotherapy, but has been criticized for a sample size of 43 patients [3].
• The European Organization of Research and Treatment of Cancer (EORTC) trial did not demonstrate a survival advantage for patients treated with adjuvant chemoradiation compared to observation. There was a trend toward survival in the chemoradiotherapy arm compared to observation in the subset of patients with pancreatic ductal carcinoma. Radiation therapy in the EORTC trial was suboptimal as the dose was inadequate (40 Gy) and the radiation was delivered with a split course [4].
• The European Study Group for Pancreatic Cancer (ESPAC)-1 evaluated adjuvant concurrent chemoradiation therapy (bolus 5-FU/split-course radiation), chemotherapy alone (5-FU/leucovorin), chemoradiation therapy followed by chemotherapy, and observation. The results demonstrated that the chemotherapy-only arm had a significant benefit over the observation arm in median survival and the chemoradiation therapy arm showed worse median survival compared to the observation arm. This study was criticized for a confusing 2x2 factorial design, possible selection bias and suboptimal radiotherapy (split course/poor quality control) [5].
• The Radiation Therapy Oncology Group (RTOG) 9704, showed a benefit of adding gemcitabine to infusional 5-FU combined with radiotherapy at the cost of more grade 4 hematological toxicity [6].
On the other hand, three randomized studies underline the use of systemic chemotherapy alone in the adjuvant setting:
• The European Study Group for Pancreatic Cancer (ESPAC)-1 trial demonstrated a survival benefit for adjuvant chemotherapy but not adjuvant chemoradiotherapy and even a possible detrimental effect for adjuvant chemoradiation [5].
• The Charité Onkologie Clinical-001 (CONKO-001) study randomized patients with resected pancreatic cancer to gemcitabine for 6 months or observation. Adjuvant chemotherapy showed a trend towards improved overall survival [7].
• The use of gemcitabine versus 5-FU was further defined by the ESPAC-3 trial, which demonstrated equivalent survival for both treatments, but more favorable safety profile with gemcitabine. There was also a trend toward improved survival in the gemcitabine arm in patients with node positive disease or those with positive resection margins [8].
This year in ASCO Gastrointestinal Cancers Symposium, Uesaka et al. presented the results of a phase III randomized trial of adjuvant chemotherapy with gemcitabine versus S-1 for patients with resected pancreatic cancer (Japanese Adjuvant Study Group of Pancreatic Cancer; JASPAC-01 study) [9]. The study showed that S-1 is non-inferior to gemcitabine or may be even better with tolerable side effects profile. The two-year survival rates were 70% and 53% for S-1 and gemcitabine, respectively. Relapse rates were also lower in the S-1 arm. The two-year relapse free survival rates were 49% and 29% for S-1 and gemcitabine, respectively. S-1 was well-tolerated, with over 70% of patients completing the therapy. Based on these interim analysis findings, the safety and efficacy committee that monitors this trial recommended early reporting of the results to speed adoption of S-1 as the new standard postoperative treatment for patients with pancreatic cancer.
The results were consistent with S-1 in advanced disease and akin to ESPAC-3 study, in which onethousand and 88 patients from 16 countries were randomized in the 5-FU/leucovorin (n=551) and gemcitabine (n=537) arms. Median overall survival was 23.0 months (95% CI: 21.1-25.0 months) with 5- FU/leucovorin and it was 23.6 months (95% CI: 21.4- 26.4 months) with gemcitabine. There was no significant difference in the effect of treatment across subgroups according to R status (P=0.56). The overall survival was similar on both arms, hence showing that gemcitabine is not superior to 5-FU in adjuvant setting. However, safety and dose intensity favored gemcitabine in this study.
S-1 is a combination of three pharmacological compounds, namely tegafur, gimeracil, and oteracil potassium (Figure 1) [10]. Tegafur is a prodrug of 5- fluorouracil (5-FU), an oral fluoropyrimidine, and it has been developed as a replacement for infusional 5- FU therapy.
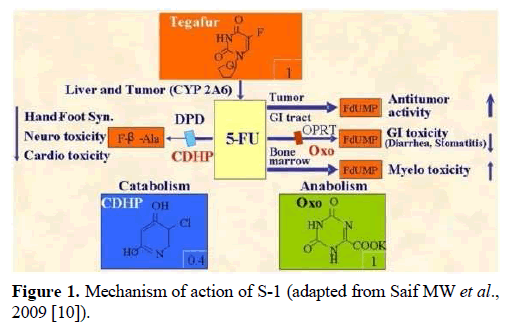
Figure 1. Mechanism of action of S-1 (adapted from Saif MW et al., 2009 [10]).
This year, S-1 has now emerged as a potential adjuvant alternative to gemcitabine in adjuvant setting for Japanese patients. The drug could also be a promising treatment option for Asian patients in other parts of the world. S-1 is currently available in several Asian countries and most of Europe, though it is not yet approved in the United States. The application of S-1 has been delayed in Western countries because of the metabolic differences between Asian and Caucasian ethnic groups; gastrointestinal side effects of S-1 are more severe among Caucasians, requiring use of lower doses of the drug for Caucasian patients. One explanation for this difference is that the pharmacokinetics of tegafur is affected by polymorphisms in cytochrome P-450 2A6, and consequently 5-FU concentrations in the plasma are more likely to be elevated in patients from Western countries [10]. For those reasons, the findings of this study are not immediately applicable to non-Asian populations, but S-1 at a reduced dose can be an appropriate replacement for infusional 5-FU therapy, even in Western countries after conducting studies in Europe and the United States among Caucasian patients, with adjustment of S-1 dose.
Locally Advanced Pancreatic Cancer
There are different treatment approaches to locally advanced pancreatic cancer management, including single or multi-agent chemotherapy, chemotherapy followed by chemoradiation, or immediate concurrent chemoradiation [11, 12, 13, 14]. A summary of several key randomized trials on locally advanced pancreatic cancer treatment which led to these different approaches is shown in Table 1.
Each of varied approaches is limited in their efficacy and carries different toxicities. At present capecitabine plus radiation therapy is the commonly used regimen followed by or gemcitabine plus/minus radiation are the most commonly used regimens in this setting.
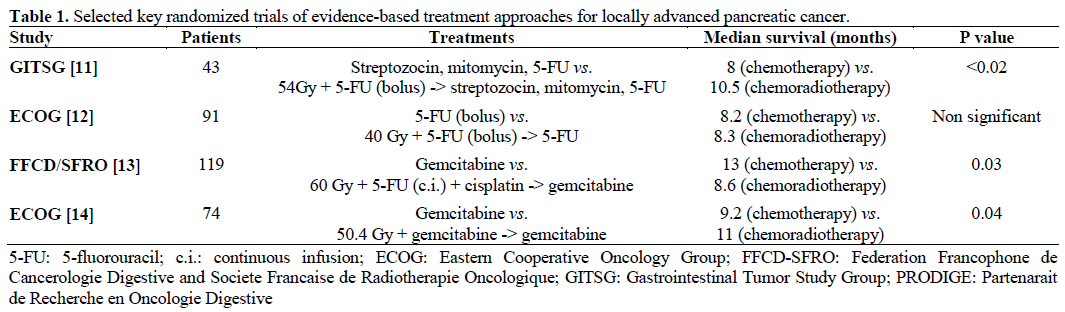
There is a strong rationale for using capecitabine in combination with concurrent radiation. Radiation has been shown to significantly increase the efficacy of capecitabine through induction of thymidine phosphorylase. Pancreatic xenograft studies from our laboratory demonstrated a synergistic antitumor effect with concomitant capecitabine and radiotherapy in both radiated and contralateral lead-shielded tumors in the same animals (abscopal effects) [15]. This led us to do the pivotal trial in pancreatic cancer followed by a phase II study (Figure 2) [16, 17]. Taken collectively, the results of these studies, and capecitabine’s favorable toxicity profile, oral administration, and, most importantly, its activity in pancreatic cancer both as a single agent as well as a radiosensitizer constitute the basis for its use in the clinic [18].
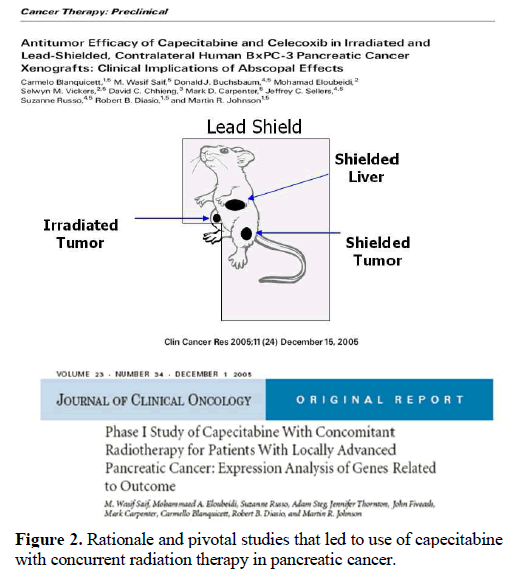
Figure 2. Rationale and pivotal studies that led to use of capecitabine with concurrent radiation therapy in pancreatic cancer.
Somnath Mukherjee et al. presented the results of the SCALOP study: a randomized phase II study of induction chemotherapy followed by gemcitabine or capecitabine based chemoradiation in locally advanced pancreatic cancer [19]. The induction chemotherapy comprising 3 cycles of gemcitabine (1,000 mg/m2 days 1,8,15 every 28 days) and capecitabine (830 mg/m2 bid days 1-21 every 28 days) followed, in responsive patients, by one cycle of gemcitabine-capecitabine and then two different schedules of chemoradiotherapy using gemcitabine (300 mg/m2 once weekly on day 1) or capecitabine (capecitabine twice daily on 5 days a week) and radiotherapy (50.4 Gy /28 fractions, 5 days a week for 5.5 weeks) in patients with locally advanced, unresectable pancreatic cancer. Overall survival was found superior for the capecitabine chemotherapy arm (15.2 vs. 13.4 months, P=0.025). Patients in the gemcitabine arm suffered more grade 3-4 hematologic (18.4% vs. 0%, P=0.007) and non-hematological toxicity (26.3% vs. 11.1%, P=0.095). As a result, capecitabine may be more effective and safer in combination with radiotherapy for treatment of locally advanced pancreatic cancer. These results further strengthen the rationale to use capecitabine as a radiosensitizer. Moreover, these results are in line with a paper published by Crane et al. showing that there is significantly higher severe toxicity rate with gemcitabine than with 5-FU in terms of myelosuppression and gastrointestinal bleeding [20] (Figure 3). Median and 1-year survivals were not significantly different with concurrent use gemcitabine vs. 5-FU (P=0.19). These possible benefits and the high rate of severe toxicity define a very narrow therapeutic index for concurrent gemcitabine-based chemo-radiotherapy given current schedule and dose of administration [20].
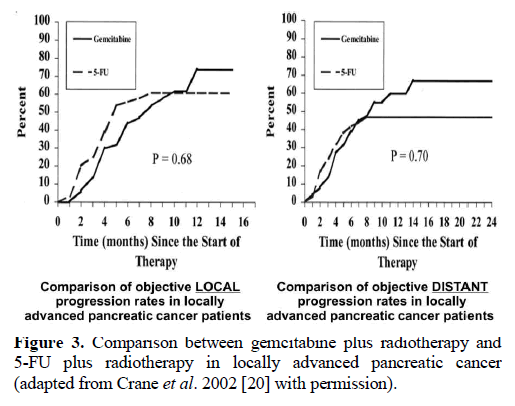
Figure 3. Comparison between gemcitabine plus radiotherapy and 5-FU plus radiotherapy in locally advanced pancreatic cancer (adapted from Crane et al. 2002 [20] with permission).
Brian A Boone et al. studied retrospectively the outcomes of patients with locally advanced pancreatic cancer that received FOLFIRINOX (5-fluorouracil, oxaliplatin, irinotecan, leucovorin) in 25 patients [21]. At the end 88% of the patients with borderline resectable cancer, and 20% of them with unresectable disease underwent R0 resection. This study suggests that FOLFIRINOX is a promising treatment in the neoadjuvant setting, to convert a patient with locally advanced pancreatic cancer to have resectable disease. Further evaluation of the use of this regimen in the neoadjuvant setting is warranted.
Advanced Pancreatic Cancer
Metastatic pancreatic cancer remains a lethal disease. The current FDA-approved cytotoxic treatment for advanced pancreatic cancer remains gemcitabine since 1997 [22]. Even though gemcitabine is tolerated well, its efficacy is marginal with median survival of 6 months. Combination chemotherapy with gemcitabine has shown no meaningful survival in metastatic pancreatic cancer [23, 24]. However, the combination of 5-fluorouracil, leucovorin, irinotecan, oxaliplatin (FOLFIRINOX) showed superiority over single agent gemcitabine in patients with Eastern Cooperative Oncology Group (ECOG) performance status 0-1. In this study, a total of 342 patients with metastatic pancreatic cancer treated in this study showed a significant improvement in median overall survival (from 6.8 months with gemcitabine to 11.1 months with FOLFIRINOX) [25]. Progression-free survival was also improved, from 3.4 to 6.4 months. The toxicity associated with FOLFIRINOX is very concerning, in particular grade 3 and 4 myelosuppression and fatigue [26]. However, prophylactic use of granulocyte colony-stimulating factors (G-CSF) seems to help. FOLFIRINOX regimen has been taken up in the U.S.A. but has also been modified by various centers, such as omitting the bolus 5-fluorouracil, decreasing the dose of irinotecan, etc. I will like to make a point here that no impact of these dose modifications on the efficacy is known at present.
On the side of targeted agents, including bevacizumab, cetuximab, and erlotinib has been dismal except a modest benefit with erlotinib. Though statistically significant, this difference was not considered clinically significant [27].
Secreted protein acidic and rich in cysteine (SPARC) is a protein involved in cell matrix interactions. SPARC plays an important role in tissue remodeling, wound repair, and cell migration. SPARC is expressed in normal human pancreatic duct and undergoes epigenetic silencing in many pancreatic cancers. Moreover, stromal fibroblasts adjacent to infiltrating pancreatic cancers frequently express SPARC [28]. Patients with SPARC expression in the stroma adjacent to their infiltrating pancreatic cancer have a poor prognosis independent of commonly used clinical parameters. The interest in nab-paclitaxel stemmed from the expression of the protein SPARC: the benefit of nab-paclitaxel is that it increases the activity of gemcitabine by depleting the stroma or increasing the concentration of gemcitabine in the tumor.
Based on the encouraging results of the preliminary data, all investigators presented the results of a phase III study of nab-paclitaxel plus gemcitabine versus gemcitabine in pancreatic cancer (MPACT) [29]. The results are summarized in Table 2 as presented at the 2013 ASCO Gastrointestinal Cancers Symposium. This regimen now offers a new option for first line treatment of advanced pancreatic cancer. Nabpaclitaxel has already been approved to treat advanced breast cancer and non-small-cell lung cancer. The correlation between SPARC expression and outcome is pending on MPACT study. However, SPARC expression evaluated by immunohistochemistry in the phase I/II study showed an association with increased median overall survival (Figure 4) [30].
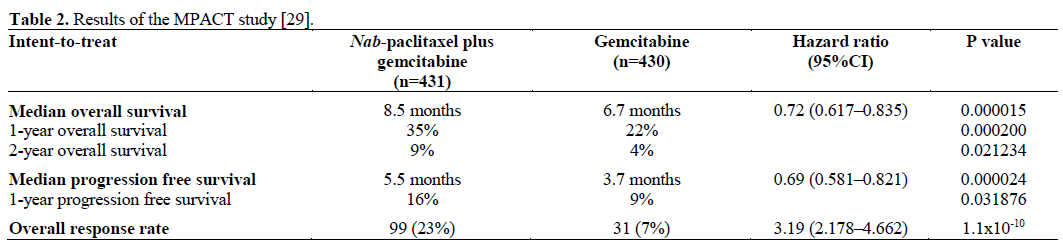
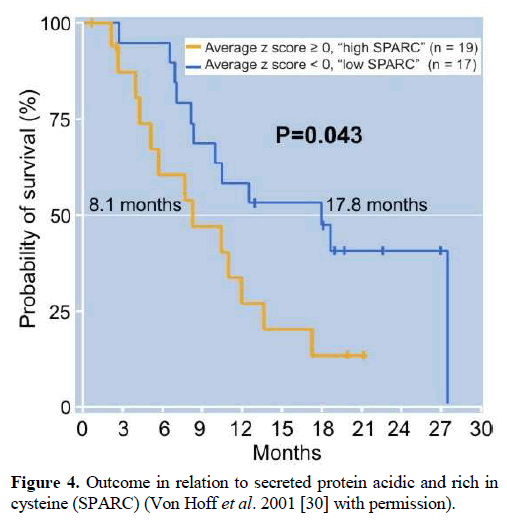
Figure 4. Outcome in relation to secreted protein acidic and rich in cysteine (SPARC) (Von Hoff et al. 2001 [30] with permission).
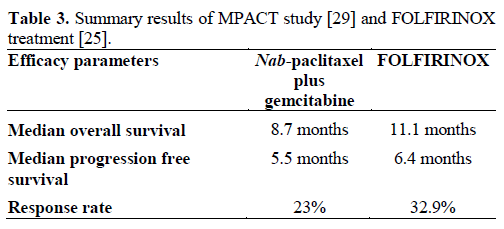
One can question that the median survival with nabpaclitaxel plus gemcitabine (8.5 months) is almost three months less than that of FOLFIRINOX (Table 3). However, it is difficult to draw any conclusions since these two regimens were not compared directly in the same trial.
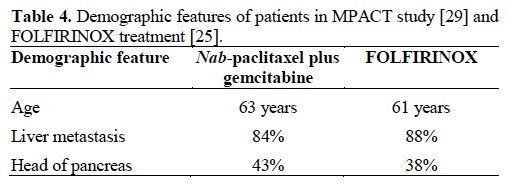
There is a need to identify which patients will ultimately benefit from one of these regimens but no demographic characteristics at present help to define so (Table 4). Though the toxicities are different (Table 5). Another important factor to consider is the financial burden. It is estimated that nab-paclitaxel will cost $6,000 to $8,000 a month for a pancreatic cancer patients, a cost likely to be more expensive than FOLFIRINOX. On the other hand, FOLFIRINOX is a toxic regimen if given in full doses and requires the patient to wear an infusion pump for 5-FU. It is my expectation that both regimens will be used by the physicians in selected patients and their preferences. There is much interest in developing new macromolecular delivery systems for cytotoxic agents in cancer therapy to improve their tumor uptake. Nabpaclitaxel offers this potential benefit. The authors definitely deserve a big applaud as this was a stepwise development from preclinical to pilot to phase III study and correlates are anxiously awaited.

A follow-on non-biologic, nanoparticle paclitaxel (NBN-Pac, Genexol-PM/IG-001; Igdrasol, Fountain Valley, CA, USA) is currently in clinical development [31]. In vitro cytotoxicity studies revealed that the mean IC50 value of NBN-Pac in four pancreatic cell lines was approximately 30-fold lower than that of gemcitabine. In preclinical studies, Genexol-PM (50 mg/kg) produced superior anti-tumor activity in the two pancreatic xenograft models tested over paclitaxel and gemcitabine at clinically equivalent doses. Recently completed phase I trial determined the maximum tolerated dose of Genexol-PM at 300 mg/m2. Of the evaluable patients, 5 out of 16 subjects (31.3%) were complete responders or partial responders with 95% exact confidence interval of 11% and 58.7%, respectively. Six out of the 18 (33.3%) subjects had tumor progression. The median progression free survival time was 5.6 months. Additional studies of Genexol-PM are therefore warranted and could yield important mechanistic information on this nanoparticle paclitaxel formulation.
Other new therapeutic agents under investigation include insulin growth factor-1 receptor antibody, and hedgehog inhibitors. IPI-926 is a small-molecule inhibitor of smoothened, a key component in the hedgehog pathway [32]. Infinity Pharmaceuticals Inc. (Cambridge, MA, USA) was testing IPI-926 with gemcitabine, in comparison to placebo with gemcitabine in a randomized phase II study to treat metastatic pancreatic cancer. In Jan 2012, Infinity Pharmaceuticals Inc. voluntarily halted this phase II study of its drug target, after early results indicated the goal endpoint of overall survival would not be met. Analysis results are not yet completed. Another agent affecting this pathway, GDC0449 is under investigation at present (NCT01195415).
Research into the cellular uptake of gemcitabine yielded clues to the possible role of human equilibrative nucleoside transporter 1 (hENT1) to enter cells and exert its cytotoxic effects. Preclinical and clinical data supported this concept. One means of enhancing gemcitabine’s efficacy in hENT1 expressing tumors is to bypass the transporter. CO-1.01 is a lipidconjugated form of gemcitabine that can diffuse across the plasma membrane without the need for hENT1 [33]. In a phase I study of CO-1.01, seven patients, including two with gemcitabine-refractory pancreatic cancer, had stable disease or tumor shrinkage [34]. hENT1 expression was not checked in this study. These findings led to two main studies: a phase IIA international study of CO-1.01 in the first-line setting for advanced pancreatic cancer, and a phase II openlabel U.S.A. study in gemcitabine-refractory advanced pancreatic cancer with low hENT1. The U.S.A. study aimed to determine whether clinical gemcitabine resistance due to low hENT1 can be overcome with CO-1.01.
Unfortunately, in late 2012 Clovis Oncology, Inc. (Boulder, CO, USA) announced the preliminary results from its Low hENT1 and Adenocarcinoma of the Pancreas (LEAP) study of CO-101 versus gemcitabine in metastatic pancreatic cancer, showing no difference in overall survival between the two arms in either the primary analysis of the hENT1-low patient population, or in the overall intent-to-treat population. Of note, this study also revealed that hENT1 status had no impact on survival for patients on gemcitabine. As a consequence of these results, Clovis Oncology, Inc. announced to suspend all development of CO-101, pending further evaluation of the LEAP data.
In a nut shell, nab-paclitaxel plus gemcitabine offers a new frontline regimen for patients with good performance status. We need to investigate this agent in earlier stages plus/minus biologics. Molecular basis of nab-paclitaxel needs to be investigated by going back to laboratory and determine the role of SPARC and other possible markers. There is an emergent need to assess novel agents and combining targeted agents with cytotoxic drugs. However, these steps must be taken concurrently with developing and assessing biomarkers.
Conflict of interest
The author has no potential conflicts of interest
References
- American Cancer Society. Cancer Facts & Figures 2013. Atlanta, Ga: American Cancer Society; 2013.
- Saif MW. Controversies in the adjuvant treatment of pancreatic adenocarcinoma. JOP. J Pancreas (Online) 2007; 8:545-52.
- Kalser MH, Ellenberg SS. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg 1985; 120:899-903.
- Klinkenbijl JH, Jeekel J, Sahmoud T, van Pel R, Couvreur ML, Veenhof CH, et al. Adjuvant radiotherapy and 5-fluorouracil after curative resection of cancer of the pancreas and periampullary region: phase III trial of the EORTC gastrointestinal tract cancer cooperative group. Ann Surg 1999; 230:776-82.
- Regine WF, Winter KA, Abrams RA, Safran H, Hoffman JP, Konski A, et al. Fluorouracil vs gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: a randomized controlled trial. JAMA. 2008 Mar 5; 299(9):1019-26. Erratum in: JAMA. 2008 Apr 23/30; 299(16):1902.
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. 2004 Mar 18; 350(12):1200-10.
- Oettle H. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer. JAMA. 2007 Jan 17; 297:267-277.
- Neoptolemos JP, Stocken DD, Bassi C, Ghaneh P, Cunningham D, Goldstein D, et al. Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: a randomized controlled trial. JAMA. 2010 Sep 8; 304(10):1073-81.
- Uesaka K, Fukutomi A, Boku N, Kanemoto H et al. Randomized phase III trial of adjuvant chemotherapy with gemcitabine versus S-1 for patients with resected pancreatic cancer (JASPAC-01 study). J Clin Oncol 30: 2012 (suppl 34; abstr 145).
- Saif MW, Syrigos KN, Katirtzoglou NA. S-1: a promising new oral fluoropyrimidine derivative. Expert Opin Investig Drugs. 2009 Mar;18(3):335-48. doi: 10.1517/13543780902729412.
- Gastrointestinal Tumor Study Group. Treatment of locally unresectable carcinoma of the pancreas: comparison of combinedmodality therapy (chemotherapy plus radiotherapy) to chemotherapy alone. J Natl Cancer Inst. 1988 Jul 20;80(10):751-5.
- Klaassen DJ, MacIntyre JM, Catton GE, et al. Treatment of locally unresectable cancer of the stomach and pancreas: A randomized comparison of 5-fluorouracil alone with radiation plus concurrent and maintenance 5-fluorouracil - an Eastern Cooperative Oncology Group study. J ClinOncol. 1985;3:373-378.
- Chauffert B, Mornex F, Bonnetain F, et al. Phase III trial comparing intensive induction chemoradiotherapy (60 Gy, infusional 5-FU and intermittent cisplatin) followed by maintenance gemcitabine with gemcitabine alone for locally advanced unresectable pancreatic cancer. Definitive resultsof the 20 Ann Oncol. 2008;19:1592-1599.
- Loehrer PJ Sr, Feng Y, Cardenes H, et al. Gemcitabine Alone Versus Gemcitabine Plus Radiotherapy in Patients With Locally JOP. J Pancreas (Online) 2013 Mar 10; 14(2):112-118. JOP. Journal of the Pancreas - https://www.serena.unina.it/index.php/jop - Vol. 14 No. 2 – March 2013. [ISSN 1590-8577] 118 Advanced Pancreatic Cancer: An Eastern Cooperative Oncology Group Trial. J ClinOncol.2011;29:4105-4112.
- Blanquicett C, Saif MW, Buchsbaum DJ, Eloubeidi M, Vickers SM, Chhieng DC, Carpenter MD, Sellers JC, Russo S, Diasio RB, Johnson MR. Antitumor efficacy of capecitabine and celecoxib in irradiated and lead-shielded, contralateral human BxPC-3 pancreatic cancer xenografts: clinical implications of abscopal effects. Clin Cancer Res. 2005 Dec 15;11(24 Pt 1):8773-81.
- Saif MW, Eloubeidi MA, Russo S, Steg A, Thornton J, Fiveash J, Carpenter M, Blanquicett C, Diasio RB, Johnson MR. Phase I study of capecitabine with concomitant radiotherapy for patients with locally advanced pancreatic cancer: expression analysis of genes related to outcome. J Clin Oncol. 2005 Dec 1;23(34):8679-87.
- Saif MW, Black G, Roy S, Bell D, Russo S, Eloubeidi MA, Steg A, Johnson MR, Zelterman D, Diasio RB. Phase II study of capecitabine with concomitant radiotherapy for patients with locally advanced pancreatic cancer: up-regulation of thymidine phosphorylase. Cancer J. 2007 Jul-Aug;13(4):247-56.
- Pancrearic Cancer. Chemoregimen.com: South Pasadena, CA, USA. www.chemoregimen.com/Pancreatic-Cancer-c-50-60.html.
- Somnath Mukherjee, et.al SCALOP: Results of a randomized phase II study of induction chemotherapy followed by gemcitabine (G) or capecitabine (Cap) based chemoradiation (CRT) in locally advanced pancreatic cancer (LANPC) J Clin Oncol 30:2012 (suppl 34;abstr LBA 146)
- Crane CH, Abbruzzese JL, Evans DB, Wolff RA, Ballo MT, Delclos M, Milas L, Mason K, Charnsangavej C, Pisters PW, Lee JE, Lenzi R, Vauthey JN, Wong AB, Phan T, Nguyen Q, Janjan NA. Is the therapeutic index better with gemcitabine-based chemoradiation than with 5-fluorouracil-based chemoradiation in locally advanced pancreatic cancer? Int J Radiat Oncol Biol Phys. 2002 Apr 1;52(5):1293-302.
- Brian A. Boone et al. Outcomes with FOLFIRINOX for locally advanced pancreatic cancer. J Clin oncol 30:2012 (suppl 34;abstr 256)
- Burris HA, 3rd, Moore MJ, Andersen J, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997;15:2403-2413.
- Saif MW, Kim R. Role of platinum agents in the management of advanced pancreatic cancer. Expert Opin Pharmacother. 2007 Nov;8(16):2719-27.
- Saif MW. Pancreatic neoplasm in 2012: an update. Tissue is an issue! JOP. 2012 Mar 10;13(2):124-7.
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364:1817-1825.
- Saif MW, Chabot J. Chemotherapy: Metastatic pancreatic cancer--is FOLFIRINOX the new standard? Nat Rev Clin Oncol. 2011 Jul 5;8(8):452-3.
- Saif MW. Research in pancreatic cancer: an update after ASCO 2012. JOP. 2012 Jul 10;13(4):330-1.
- J. R. Infante, H. Matsubayashi, N. Sato, R. Chang, A. P. Klein, J. A. Tonascia, T. A. Sohn, C. J. Yeo, C. A. Iacobuzio-Donahue, M. Goggins. The SPARC of pancreatic cancer stroma. 2006 Gastrointestinal Cancers Symposium. Abstract No:.141
- Daniel D. Von Hoff TJE, Francis P. Arena, E. Gabriela Chiorean, Jeffrey R. Infante, Malcolm J. Moore, Thomas E. Seay, Sergei Tjulandin, Wen Wee Ma, Mansoor N. Saleh, Marion Harris, Michele Reni, Ramesh K. Ramanathan, Josep Tabernero, Manuel Hidalgo, Eric Van Cutsem, David Goldstein, Xinyu Wei, Jose Luis Iglesias, Markus Frederic Renschler; Virginia G. Piper: Randomized phase III study of weekly nab-paclitaxel plus gemcitabine versus gemcitabine alone in patients with metastatic adenocarcinoma of the pancreas (MPACT). J Clin Oncol 30: 2012 (suppl 34; abstr LBA148), 2013
- Von Hoff DD, Ramanathan RK, Borad MJ, Laheru DA, Smith LS, Wood TE, Korn RL, Desai N, Trieu V, Iglesias JL, Zhang H, Soon-Shiong P, Shi T, Rajeshkumar NV, Maitra A, Hidalgo M. Gemcitabine plus nab-paclitaxel is an active regimen in patients with advanced pancreatic cancer: a phase I/II trial. J Clin Oncol. 2011 Dec 1;29(34):4548-54.
- Saif MW, Podoltsev NA, Rubin MS, Figueroa JA, Lee MY, Kwon J, Rowen E, Yu J, Kerr RO. Phase II clinical trial of paclitaxel loaded polymeric micelle in patients with advanced pancreatic cancer. Cancer Invest. 2010 Feb;28(2):186-94.
- Dimou A, Syrigos K, Saif MW. Rationale for inhibition of the hedgehog pathway paracrine loop in pancreatic adenocarcinoma. JOP. 2011 Jan 5;12(1):1-5.
- Saif M, Lee Y, Kim R. Harnessing gemcitabine metabolism: a step towards personalized medicine for pancreatic cancer. Ther Adv Med Oncol. 2012 Nov;4(6):341-6.
- Nilsson B., Hendlisz A., Castella M., Aamdal S., Dueland S., Nyakas M., et al. (2009) First-in-human study of a novel nucleoside analogue, CP-4126, in patients with advanced solid tumors. J Clin Oncol27(15 Suppl.): abstract 2577.

