Michael Roche1*, Odessa Hamidi1, Grace Weyant2, Jaimey Pauli1
1Department of Obstetrics and Gynecology, Penn State Milton S. Hershey Medical Center, Hershey, Pennsylvania, USA
2Department of Pathology and Laboratory Medicine, Penn State Milton S. Hershey Medical Center, Hershey, Pennsylvania, USA
*Corresponding Author:
Michael Roche
Department of Obstetrics and Gynecology Penn State Milton S. Hershey Medical Center, Hershey, Pennsylvania 500 University Drive, P.O. Box 850, MC H103 Hershey, PA 17033, USA
Tel: 708-834-4097
E-mail: mroche@pennstatehealth.psu.edu
Received date: April 19, 2017; Accepted date: May 09, 2017; Published date: May 15, 2017
Citation: Roche M, Hamidi O, Weyant G, et al. Advanced pemphigoid gestationis initially misdiagnosed as pruritic urticarial papules and plaques of pregnancy. Gynecol Obstet Case Rep 2017, 3:2. doi:10.21767/2471-8165.1000050
Keywords
Pregnancy complications; Pemphigoid gestationis; Skin diseases, Vesiculobullous; Pruritic urticarial papules; Plaques of pregnancy
Introduction
Pemphigoid gestationis (PG), previously known as herpes gestationis, is a rare autoimmune skin condition that affects between 1 in 10,000 and 1 in 50,000 pregnancies [1]. It is related to the pemphigoid skin disorders. Patients typically present in the second or third trimester with complaints of severely pruritic lesions involving the trunk [2,3]. These lesions begin as urticarial plaques that rapidly progress to bullae. The condition spreads to the extremities, involving the palms and soles but spares the face and mucous membranes. The differential diagnoses include other dermatoses of pregnancy, drug reaction, erythema multiforme (EM) and contact dermatitis [2]. Diagnosis is confirmed with lesion biopsy showing linear C3 deposition along the basement membrane zone [1-3]. Goals of treatment are to relieve symptoms, decrease further bullae formation, and promote healing of the lesions. Most patients will respond to a course of corticosteroids. There is a reported association between PG and small-for-gestational age infants and prematurity, and 10% of neonates will have transient eruption of PG [2]. Given its rarity and ability to mimic other dermatoses of pregnancy, high clinical suspicion is necessary to properly diagnose PG.
We present a case of PG initially misdiagnosed as pruritic urticarial papules and plaques of pregnancy (PUPPP), a more common and milder dermatosis of pregnancy.
Case
The patient is a 34 year old G5P1122 who presented to her obstetrician at 18 weeks gestational age due to pruritic lesions on her legs. Her pregnancy had otherwise been uncomplicated. She was diagnosed with PUPPP and was prescribed topical corticosteroids. Despite adequate therapy for PUPPP, the rash worsened, and she presented for an acute visit several weeks later. At this time her lesions were noted to be raised with associated blistering and present on multiple skin surfaces. She was given a course of oral corticosteroids to be treated outpatient. Her rash progressed, and she developed dyspnea and tachycardia, prompting her to present to her local emergency department at 23 5/7 weeks gestational age. She denied sick contacts, new lotions/soaps, or new medications. Concern arose for Stevens-Johnson syndrome due to this new constellation of symptoms. Sufficient NICU and dermatology services were not available to care for this patient. Given the complexity of the presentation and concern for preterm delivery at a periviable gestational age should symptoms worsen, she was transferred to our institution for care.
Upon physical examination, tense bullae were identified on the anterior aspect of her right thigh. In addition, erythematous plaques varying in size with central clearing (target lesions) were noted on her trunk and extremities (Figures 1-3). Mucus membranes were spared. The presumptive diagnosis of PG was made and dermatology was consulted. The lesions were biopsied. She was started on 0.8 mg/kg methylprednisolone and 0.1% triamcinolone cream. Her symptoms quickly improved and she was discharged on a steroid taper on hospital day four. The biopsies confirmed the diagnosis of PG. At her subsequent follow up appointments her skin was healing appropriately without any new lesion formation, and her foetus showed no signs of compromise.

Figure 1 Patient’s left flank.
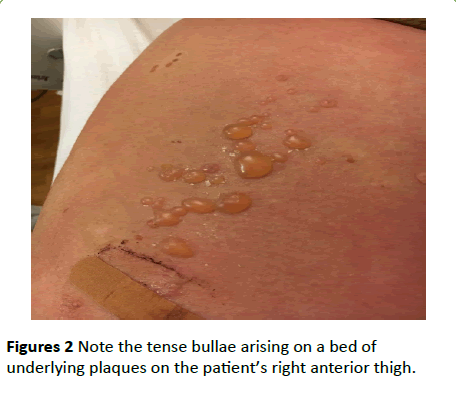
Figures 2 Note the tense bullae arising on a bed of underlying plaques on the patient’s right anterior thigh.
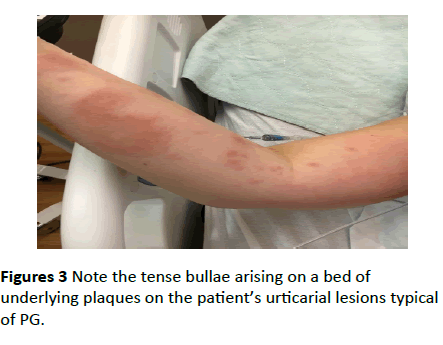
Figures 3 Note the tense bullae arising on a bed of underlying plaques on the patient’s urticarial lesions typical of PG.
Discussion
Managing dermatoses of pregnancy is part of the fundamental skill set for all practicing obstetricians. The most common dermatosis is PUPPP, and its course is generally mild [1]. Our case shows the importance of reassessing the presumed diagnosis should refractory symptoms or suspicious clinical findings arise, such as progression of lesions or development of bullae. The differential diagnosis should be expanded to include all dermatoses of pregnancy and as well as those not specific to pregnancy. When confronted with this picture, pathologic analysis of perilesional skin biopsies should be undertaken to narrow the diagnosis. In our case, pathology showed a spongiotic epidermis, papillary edema, and eosinophilic infiltrate. Immunofluorescence showed linear C3 deposition in the basement membrane zone (Figures 4 and 5).
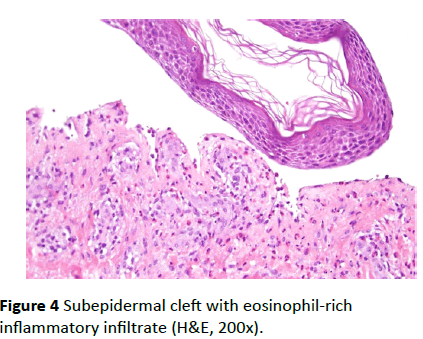
Figure 4 Subepidermal cleft with eosinophil-rich inflammatory infiltrate (H&E, 200x).
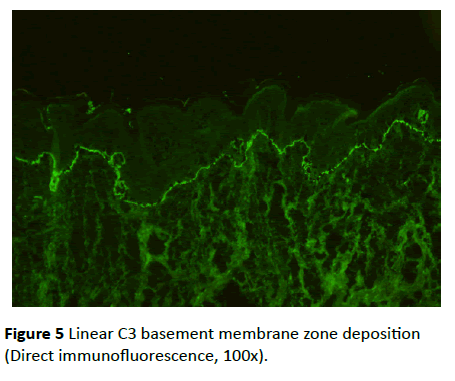
Figure 5 Linear C3 basement membrane zone deposition (Direct immunofluorescence, 100x).
Pemphigoid gestationis is a rare condition affecting between 1 in 10,000 and 1 in 50,000 pregnancies [1]. It typically affects Caucasian women. The disease’s tendency to favour Caucasian patients is perhaps due to an association between PG and the human leukocyte antigens HLA-DR3 (61% to 80%), HLA-DR4 (52%), or both (43% to 50%), which are more frequently found in the Caucasian population [4]. These antigens also predispose patients to future autoimmune disorders, most commonly Graves’ disease [3,5].
The disorder is unique to pregnancy, recently postpartum patients, and those affected by gestational trophoblastic disease [2]. Patients typically present in the second or third trimester, although nearly 25% of patients present in the postpartum period. The antibody responsible for the eruption begins expression in the second trimester and binds to a target on the basement membrane of the skin [3].
Lesions begin as urticarial plaques that rapidly progress to bullae. These lesions are intensely pruritic, usually begin in the periumbilical area, and are often debilitating. The condition spreads to the extremities, involving the palms and soles but sparing the face and mucous membranes. It is important to rule out infectious or allergic causes of the skin eruptions. Distinguishing it from other dermatoses of pregnancy, especially PUPPP, can be difficult [6].
Initial physical exam should document both areas of lesion involvement and areas spared. Definitive diagnosis of PG is made by immunofluorescence staining of skin biopsies. These lesions demonstrate linear deposits of C3 along the basement membrane zone. Histopathologic analysis shows papillary dermal edema that may result in subepidermal vesicle formation and a dermal inflammatory infiltrate with abundant eosinophils [1,7].
Differential diagnosis includes other dermatoses of pregnancy, erythema multiforme (EM) and contact dermatitis. PUPPP is more common than PG and tends to affect nulliparous women in the third trimester. PUPPP typically clusters in the striae and spares the umbilicus. Our patient fit the typical presentation as she is Caucasian, multiparous and initially presented in the second trimester. Differentiation between the two diseases can be done based on exam findings and immunofluorescence. The larger bullae of PG help distinguish it from PUPPP lesions which are typically no more than small vesicles. Additionally, positive direct immunofluorescence of PG also helps distinguish it from PUPPP [3]. Erythema multiforme can be differentiated from PG by a thorough patient history, direct immunofluorescence, and histologic examination [7]. Contact dermatitis lesions usually take the shape of the inciting agent (e.g. jewellery and clothing).
Proper diagnosis is essential, as PG is associated with preterm delivery and small for gestational age neonates [8]. As such, serial ultrasounds may be used to screen for fetal growth restriction after diagnosis is confirmed [1]. PG itself has only mild fetal effects therefore early delivery is not indicated based on the diagnosis of PG alone. Approximately 10% of neonates will show signs of PG, likely due to transplacental antibody transfer [3]. These lesions are self-limited and will resolve as the maternal antibodies clear from the infant’s system [4]. However, parental surveillance of these neonatal lesions is critical as bacterial superinfection can be devastating [2].
Treatment consists of corticosteroids, which relieve pruritus and prevent new bullae from developing. Low dose prednisone (20 mg to 40 mg daily in divided doses) typically results in improvement. Topical steroid creams such as triamcinolone can assist with symptom control. In more advanced cases, such as the one presented above, doses as high as 180 mg/day have been used [1-3]. Upon symptomatic control, the dose is then tapered and possibly discontinued. Given frequent peripartum flares, treatment is often restarted or the dose is increased at this time in anticipation of a flare [2,3].
Maternal effects of PG are limited to symptoms of the lesions. Patients at risk of prolonged postpartum flares are older, with higher parity, more widespread lesions, and have a history of PG [1-3]. Oral contraceptive use is also associated with postpartum flares, and this should be taken into account when discussing postpartum contraception [2]. Persistent PG has previously been treated with alternative therapies due to the adverse effects associated with long-term corticosteroid use. Case reports have described tetracyclines with nicotinamide, high dose intravenous IgG with cyclosporine, plasmapheresis, immunoapheresis, ritodrine, azathioprine, rituximab, and chemical oophorectomy with goserelin with good results [1,4].
Patients should be advised that PG frequently recurs in future pregnancies and may increase in both severity and duration with each subsequent pregnancy [2,3]. Because of the reported association between PG and Grave’s disease, immediate postpartum and periodic thyroid function screening is recommended. No consensus exists on frequency and timing of period thyroid function screening after the postpartum period [1-3,5].
This case reflected both typical and atypical features of PG. Typical features of this case were that our patient was a Caucasian multiparous female who presented in the second trimester. It was, however, atypical that her lesions initially began on her legs before spreading to the rest of her body. Prompt diagnosis of PG aids in rapid and effective relief of the intense discomfort of these pruritic lesions. The biggest challenges to rapid diagnosis are the rarity of this condition and its ability to mimic more common dermatoses. High clinical suspicion will allow for proper diagnosis with appropriate treatment and follow up.
References
- Kroumpouzos G (2010) Specific dermatoses of pregnancy: Advances and controversies. Expert Rev Dermatol 5: 633-48.
- Kroumpouzos G (2012) Skin disease in pregnancy and the puerperium. In: Gabbe SG, Niebyl JR, Simpson JL, Landon MB, Galan HL, Jauniaux ERM, Driscoll, DA, (Eds). Obstetrics: Normal and Problem Pregnancies (6thedn); Philadelphia (PA): Elsevier/Saunders 1091-1093.
- Engineer L, Bhol K, Ahmed AR (2000) Pemphigoid gestationis: A review. Am J Obstet Gynecol 183: 483-491.
- Semkova K, Black M (2009) Pemphigoid gestationis: Current insights into pathogenesis and treatment. Eur J Obst Gynecol Reprod Biol 145: 138-144.
- Shornick, JK, Black MM (1992) Secondary autoimmune diseases in herpes gestationis (pemphigoid gestationis). J Am Acad Dermatol 26: 563-566.
- Kroumpouzos G, Cohen LM (2003) Specific dermatoses of pregnancy: An evidence-based systematic review. Am J Obstet Gynecol 188: 1083-1092.
- Katz SI (1993) Herpes gestationis. In: Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg IM, Austen KF (Eds). Dermatology in general medicine. (4thedn); New York (NY): McGraw-Hill 626-629.
- Shornick JK, Black MM (1992) Fetal risks in herpes gestationis. J Am Acad Dermatol 26:63-68.

