Keywords
Chemotherapy, Adjuvant; Fluorouracil; gemcitabine; Pancreatic Neoplasms; Radiotherapy
Abbreviations:
alpha-GT: alpha-1,3 galactosyl transferase: ASCO: American Society of Clinical Oncology; CONKO: Charité Onkologie; EORTC: European Organization of Research and Treatment of Cancer; ESPAC: European Study Group for Pancreatic Cancer; GITSG: Gastrointestinal Tumor Study Group; RTOG: Radiation Therapy Oncology Group
What Did We Know Before the 2011 ASCO GI Cancer Symposium?
Only 10-20% of patients have resectable disease at the time of pancreatic cancer diagnosis. The prognosis of patients after complete resection of node-negative cancer is poor, with 3-year disease-specific survival rate at 27% (95% confidence interval (CI): 23-32%) and median survival of 15-19 months [1, 2, 3]. The treatment plan in the adjuvant setting is currently dependent on which side of the Atlantic you are located: chemotherapy alone is mostly used in Europe (European Study Group for Pancreatic Cancer-1: ESPAC-1, ESPAC-3; Charité Onkologie Clinical-001: CONKO-001) while chemoradiation therapy is the current standard in the U.S. (Gastrointestinal Study Group: GITSG; Radiation Therapy Oncology Group 9704: RTOG 9704).
Adjuvant Therapy with Chemotherapy and External Beam Radiotherapy
The randomized trials evaluating adjuvant therapy in pancreatic cancer are summarized in Table 1.
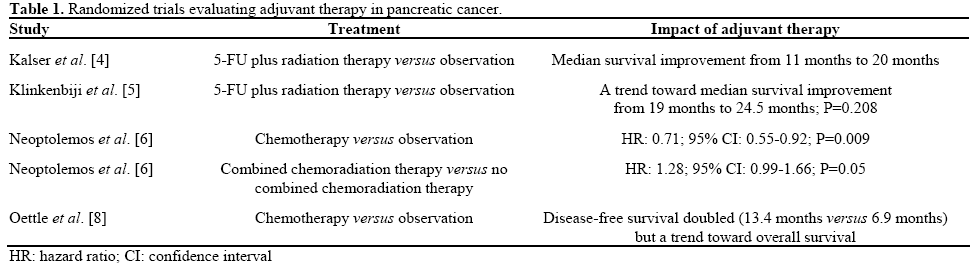
GITSG. The pivotal study to support adjuvant chemoradiotherapy in patients with resected pancreatic cancer was the GITSG study. This small study that enrolled 43 patients showed a survival benefit (median survival: 20 months versus 11 months; 5-year survival: 18% versus 8%) in patients who received bolus 5-FU with radiation therapy for one year compared with patients who did not [4]. This study was criticized for its small sample size.
EORTC. The European Organization of Research and Treatment of Cancer (EORTC) compared postoperative combined infusional 5-FU and radiotherapy given in split course (40 Gy) with observation only in patients with resected pancreatic and periampullary cancer. This study showed a trend toward benefit in terms of median survival (24.5 months versus 19 months; P=0.208) for the chemoradiation therapy arm. The subgroup analysis looking only at pancreatic cancer patients showed median survival of 17.1 months versus 12.6 months (P=0.099) for chemoradiation therapy versus observation [5]. This study was also criticized for its radiotherapy component: suboptimal lower doses and split courses.
ESPAC-1. This study was a two-by-two factorial designed study comparing adjuvant concurrent chemoradiation therapy (bolus 5-FU/split-course radiation), chemotherapy alone (5-FU/leucovorin), chemoradiation therapy followed by chemotherapy, and observation. The results revealed that the chemotherapy-only arm had statistically significant benefit over the observation arm in median survival (20.1 months versus 15.5 months; P=0.009). However, the chemoradiation therapy arm showed worse median survival (15.9 months versus 17.9 months; P=0.05) [6]. This study was criticized too for possible selection bias as both patients and clinicians were allowed to select which trial to enter, a concern of suboptimal radiotherapy, and for allowing the final radiotherapy dose to be left to the judgment of the treating physicians. Moreover, the treatment for patients in the chemoradiation therapy group did not include postradiotherapy adjuvant chemotherapy, making direct comparison with the GITSG trial difficult.
RTOG 9704. In USA, the RTOG 9704 study randomized 538 resected pancreatic cancer patients to evaluate the benefit of adding gemcitabine to infusional 5-FU combined with radiotherapy. One arm received 5-FU plus radiotherapy and the other arm was treated with gemcitabine before and after 5-FU plus radiotherapy. Although there was no significant difference when pancreatic body and tail cancers were all included, patients with pancreatic head tumors (n=380) showed benefit in median survival (18.8 months versus 16.7 months; P=0.047) [7].
Chemotherapy Alone
CONKO-001. In the CONKO-001 study, Oettle et al. randomized 368 patients with resected pancreatic cancer to gemcitabine or observation for six months. This trial showed a statistically significant disease-free survival benefit (13.4 months versus 6.9 months; P<0.001) of gemcitabine versus observation. Treatment with gemcitabine caused a trend toward overall survival benefit (22.1 months versus 20.2 months; P=0.06) [8]. This benefit of chemotherapy was consistent with the result from the ESPAC-1 trial, which showed the benefit of 5-FU/leucovorin over no adjuvant therapy in pancreatic cancer patients (median survival: 19.7 months versus 14 months) who had complete resection [6].
ESPAC-3. The role of gemcitabine as a single agent was further defined by the ESPAC-3 study, which is a randomized phase III study comparing observation versus 5-FU versus gemcitabine in the adjuvant setting of pancreatic cancer patients. Neoptolemos et al. presented the results of ESPAC-3 study [9], in which patients with an R0/R1 resection for pancreatic ductal adenocarcinoma were randomized (stratified for resection margin status and country) starting before 8 weeks of surgery to receive either bolus 5- FU/leucovorin or gemcitabine observation for 6 months versus observation. The study was later revised to close the observation arm. The primary outcome measure was overall survival. One-thousand and 88 patients from 16 countries were randomized in the 5- FU/leucovorin (n=551) and gemcitabine (n=537) arms. Median overall survival was 23.0 months (95% CI: 21.1-25.0 months) with 5-FU/leucovorin and it was 23.6 months (95% CI: 21.4-26.4 months) with gemcitabine. There was no significant difference in the effect of treatment across subgroups according to R status (P=0.56). The overall survival was similar on both arms, hence showing that gemcitabine is not superior to 5-FU in adjuvant setting. However, safety and dose intensity favored gemcitabine in this study.
What Did We Learn at the 2011 ASCO GI Cancer Symposium?
Hyperacute Immunotherapy Approach for Resected Pancreatic Cancer Patients
The development of pancreatic cancer vaccines has been the subject of recent developments in the adjuvant treatment of pancreatic cancer [10]. Algenpantucel-L is composed of irradiated, live, allogeneic human pancreatic cancer cells expressing the enzyme alpha- 1,3 galactosyl transferase (alpha-GT). Murine alpha- GT epitopes, not present on human cells, induce a hyperacute rejection of vaccine pancreatic cancer cell allografts. Binding of pre-existing human anti-alpha- GT antibodies (which naturally occur against gut flora) to murine alpha-GT epitopes, results in rapid activation of antibody-dependent cell-mediated cytotoxicity towards allograft cells. The host immune system then attacks endogenous pancreatic cancer cells, resulting in antibody-dependent cell-mediated cytotoxicity towards endogenous pancreatic cancer cells (Figures 1 and 2) [11]. Hyperacute immunotherapy is based on the hypothesis that alpha-GT epitopes in human cancer cells trigger a powerful immune response called “HyperAcute Rejection”, characteristically targeting xenotransplanted tissue, in this case against the modified cancer cells. This inflammatory reaction/immune response is thought to be responsible for generating immunity against tumor antigens.
Figure 1. Hyperacute rejection and immunotherapeutic applications.
Figure 2. Hyperacute rejection in xenotransplantation.
A phase II open-label single arm, multi-institutional phase II study was presented at the 2011 ASCO GI Cancer Symposium. The study was designed to evaluate algenpantucel-L plus standard adjuvant therapy (RTOG-9704: gemcitabine plus 5-FU and radiation therapy) for pancreatic cancer patients undergoing R0/R1 resection. Disease-free survival and overall survival were the primary and secondary endpoints, respectively. About 70 patients received gemcitabine plus 5-FU and radiation therapy plus algenpantucel-L (mean 12 doses, range 1-14 doses) as shown in Figure 3 [12].
Figure 3. Treatment schema.
Upward arrows are gemcitabine administrations. Downward arrows
are algenpantucel-L administrations.
This phase 2 study enrolled 73 (70 evaluable) mostly high risk patients (81% node positive; 20% CA 19-9 greater than 180 U/L; median tumor size: 3.2 cm). At a median follow up of 17 months (range: 12-36 months), analysis of the data shows 63% disease-free survival and 86% overall survival at one year. Furthermore, a subpopulation analysis indicates there may be a dose response effect favoring a higher dose (300M cells) compared to a lower dose (100M cell) for both diseasefree survival (80% versus 52%; P=0.02) and overall survival (96% versus 80%; P=0.053) at one year.
Algenpantucel-L was well tolerated, with no doselimiting toxicities. The only expected and commonly observed adverse reaction is inflammation at the injection site, which typically resolves within a week. The study revealed that the addition of algenpantucel-L to standard adjuvant therapy for resected pancreatic cancer may improve survival. A randomized phase III study involving about 700 patients began patient enrollment in May 2010. The phase III study allows either 6 months of gemcitabine alone (CONKO-001) or gemcitabine plus infusional 5-FU and radiation therapy (RTOG) as standard of care options.
Discussion
About 10-20% of patients have resectable disease at the time of pancreatic cancer diagnosis; the curative resection rate is approximately 14% and median survival up to 20 months despite the incorporation of gemcitabine in this setting. The 5-year survival rate following resection is 25-30% for node-negative disease and 10% for node-positive cancers. Local recurrence is usually attributed to the difficulty of achieving microscopically negative surgical margins, particularly at the retroperitoneal one. The high risk of local and systemic disease recurrence, as well as overall poor prognosis, laid down the rationale for adjuvant therapy after resection of pancreatic adenocarcinoma.
While both the CONKO-001, ESPAC-3 and RTOG 9704 studies support the use of gemcitabine as the systemic agent of choice in the adjuvant setting, the benefit of radiotherapy remains inconclusive in randomized trials. The ESPAC-3 study showed that the overall survival was similar on both arms: gemcitabine versus 5-FU/leucovorin. However, safety and dose intensity favored gemcitabine in this study. This study is very important because there has been a tendency to reject 5-FU in advanced pancreatic cancer and now it is very much back on the stage and further assessment of capecitabine in this setting is underway.
The vaccines have been developing in the adjuvant treatment of pancreatic cancer. Lutz et al. developed an irradiated granulocyte/macrophage-colony-stimulating factor (GM-CSF) transfected allogeneic whole cell line pancreas adenocarcinoma immunotherapy [13]. Their group presented the results of a phase II study of 60 patients with resected pancreatic adenocarcinoma administered a total of five immunotherapy treatments using two pancreatic cancer cell lines each delivering 2.5x108 cells intradermal [14]. The first immunotherapy treatment was administered 8 to 10 weeks following surgical resection. Patients subsequently were treated with 5-FU continuous intravenous infusion with concurrent radiotherapy. Patients who were disease-free one month after completion of chemo-radiotherapy received immunotherapy treatment 2-4, each one month apart. A fifth and final booster immunotherapy treatment was administered 6 months after vaccine 4. The primary endpoint was disease free survival and secondary endpoints were overall survival and toxicity, and the induction of mesothelin-specific T cell responses. They recently published the results showing the median disease-free survival of 17.3 months (95% CI: 14.6- 22.8 months) with median survival of 24.8 months (95% CI: 21.2-31.6 months). The administration of immunotherapy was well tolerated. They also reported that the post-immunotherapy induction of mesothelinspecific CD8 T cells in HLA-A1 and HLA-A2 patients correlated with disease-free survival.
This year at the 2011 ASCO GI Cancer Symposium, the researchers presented another vaccine study using hyper acute immunotherapy. Kaplan-Meier estimated survival rates at 12 and 24 months are 91% and 54%, respectively, comparing favorably to 63% and 32% expected survival rates based on the nomogram described by Brennan et al. [14]. Likewise, the current median disease-free survival of 16 months compares favorably to the 11 months observed in RTOG 9704. The results are very encouraging. Algenpantucel-L was well tolerated. Currently, a phase III study is recruiting patients to further assess the efficacy of incorporating the vaccine with either CONKO-001 or RTOG 9704 regimens.
The optimal adjuvant approach for patients with resected pancreatic cancer remains elusive. Intensive research is currently being conducted including chemotherapeutic, immunotherapeutic, and other agents. In the R0 resection setting cure is the goal and we can do better still. Hopefully, incorporation of novel agents and/or vaccine therapy may lead to a better outcome for these patients. In addition, early detection strategies, better identification of precursor lesions and high-risk groups, direction of patients to high-volume centers for surgical and oncologic expertise are warranted to improve outcome in this population of patients.
Conflict of interest
The author has no potential conflict of interest
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer Statistics, 2009. CA Cancer J Clin 2009; 59:225-49.
- Li D, Xie K, Wolff R, Abbruzzese JL. Pancreatic cancer. Lancet 2004; 363:1049-57.
- Saif MW. Controversies in the adjuvant treatment of pancreatic adenocarcinoma. JOP. J Pancreas (Online) 2007; 8:545-52.
- Kalser MH, Ellenberg SS. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg 1985; 120:899-903.
- Klinkenbijl JH, Jeekel J, Sahmoud T, van Pel R, Couvreur ML, Veenhof CH, et al. Adjuvant radiotherapy and 5-fluorouracil after curative resection of cancer of the pancreas and periampullary region: phase III trial of the EORTC gastrointestinal tract cancer cooperative group. Ann Surg 1999; 230:776-82.
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med 2004; 350:1200-10.
- RegineWF, Winter KA, Abrams RA, Safran H, Hoffman JP, Konski A, et al. Fluorouracil vs gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: a randomized controlled trial. JAMA 2008; 299:1019-26.
- Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA 2007; 297:267-77.
- Neoptolemos J, Büchler M, Stocken DD, Ghaneh P, Smith D, C. Bassi C, et al. A multicenter, international, open-label, randomized, controlled phase III trial of adjuvant 5-fluorouracil/folinic acid (5- FU/FA) versus gemcitabine (GEM) in patients with resected pancreatic ductal adenocarcinoma. J Clin Oncol 2009; 27(18 Suppl.):Abstract LBA4505.
- Laheru D, JaffeeEM. Immunotherapy for pancreatic cancer: science driving clinical progress. Nat Rev Cancer 2005; 5:459-67.
- Rossi GR, MautinoMR, AwwadDZ, Husske K, Lejukole H, Koenigsfeld M, Ramsey WJ, Vahanian N, Link CJ. Allogeneic melanoma vaccine expressing alphaGal epitopes induces antitumor immunity to autologous antigens in mice without signs of toxicity. J Immunother. 2008 Jul-Aug;31(6):545-54.
- J. M. Hardacre, M. F. Mulcahy, W. Small Jr., M. Talamonti, J. C. Obel, C. S. Rocha Lima, H. Safran, H. Lenz, E. G. Chiorean, C. J. Effect of the addition of algenpantucel-L immunotherapy to standard adjuvant therapy on survival in patients with resected pancreas cancer. J Clin Oncol 2011; 29(Suppl. 4):Abstract 236.
- Lutz E, Yeo CJ, Lillemoe KD, Biedrzycki B, Kobrin B, Herman J, Sugar E, Piantadosi S, Cameron JL, Solt S, Onners B, Tartakovsky I, Choi M, Sharma R, IlleiPB, Hruban RH, Abrams RA, Le D, Jaffee E, Laheru D. A Lethally Irradiated Allogeneic Granulocyte- Macrophage Colony Stimulating Factor-Secreting Tumor Vaccine for Pancreatic Adenocarcinoma: A Phase II Trial of Safety, Efficacy, and Immune Activation. Ann Surg. 2011 Jan 6.
- Brennan MF, Kattan MW, Klimstra D, Conlon K. Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann Surg. 2004 Aug;240(2):293-8.




