Keywords
Chemotherapy, Adjuvant; Pancreatic Neoplasms
Abbreviations
CONKO: Charité Onkologie Clinical; ECM: extracellular matrix; EORTC: European Organisation for Research and Treatment of Cancer; ESPAC: European Study Group for Pancreatic Cancer; GITSG: Gastrointestinal Study Group; MMP-7: matrix metalloproteinase-7; RTOG: Radiation Therapy Oncology Group
Introduction
Pancreatic cancer continues to be an elusive disease with a 5-year overall survival of 4%. It is the 4th leading cause of cancer death in the United States. The American Cancer Society estimates in the United States for 2013 about 45,220 people (22,740 men and 22,480 women) will be diagnosed with pancreatic cancer. About 38,460 people (19,480 men and 18,980 women) will die of pancreatic cancer [1]. The only chance for a prolonged survival and cure is surgery. Unfortunately only 20% of all patients diagnosed with pancreatic cancer are surgical candidates due to the aggressive biology of this disease. The optimal adjuvant treatment approach remains unclear. Despite improvements in radiation, systemic therapies, and targeted agents, the 5-year survival rate for early stage resected patients remains less than 25%.
What We Knew Before the 2014 ASCO Gastrointestinal Cancers Symposium
There have been multiple studies looking to improve survival in the adjuvant setting; however, there remains considerable controversy regarding the optimal adjuvant treatment. The use adjuvant radiation to chemotherapy is the issue of some debate regarding adjuvant therapy. Although systemic disease represents the major risk for failure following resection, there are patients who would benefit from adjuvant local therapy that remain difficult to identify at present. Current accepted standard of care is adjuvant gemcitabine following curative resection, but there have been no conclusions regarding the role or timing of adjuvant chemoradiation [2].
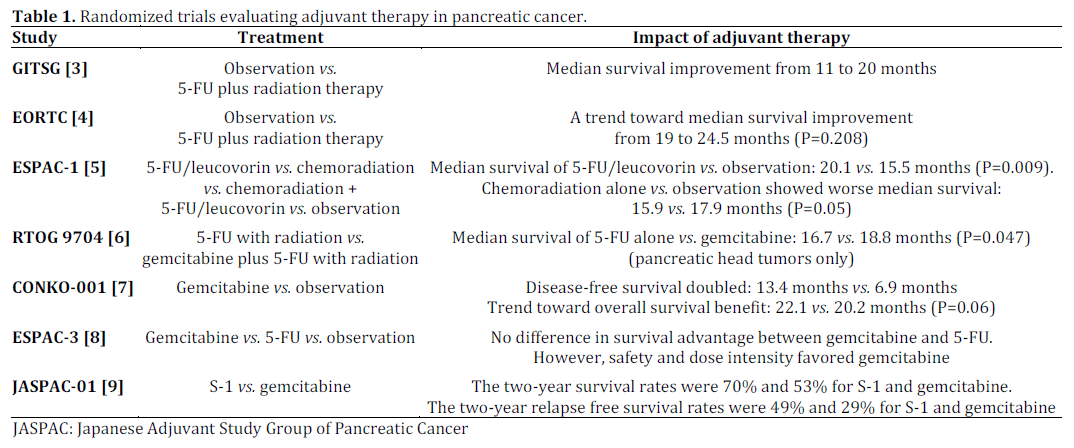
The randomized trials evaluating adjuvant therapy in pancreatic cancer are summarized in Table 1.
What We Learned at the 2014 ASCO Gastrointestinal Cancers Symposium
Pancreatic cancer remains a substantial public health problem internationally. This disease has been used for testing new therapies with very little progress. More innovative treatment options are needed to improve survival in this patient population. This year in ASCO Gastrointestinal Cancer Symposium, Cho et al. (Abstract #325) presented the results of adjuvant gemcitabine with the addition of docetaxel followed by 5-FU chemoradiation for patients with resected pancreatic cancer [10]. The primary objective was to evaluate the feasibility and safety of this regimen with the secondary aims to describe the toxicities, disease-free and overall survival. Kumar et al. (Abstract #330) presented the results of two different adjuvant treatments on survival. They compared adjuvant chemoradiation to adjuvant chemotherapy [11]. Lastly, Heestand et al. (Abstract #176) used a novel way to look at different biomarkers in serum of patients in the Radiation Therapy Oncology Group (RTOG) 9407 and evaluated the survival depending on the type of chemotherapy used [12]. A lower serum CEA and CA 19-9 gave a better overall survival in all patients which has already been established. Low levels of matrix metalloproteinase-7 (MMP-7) predicted an overall survival benefit from adjuvant gemcitabine, but not 5-FU.
Adjuvant Gemcitabine Plus Docetaxel Followed by 5- FU Chemoradiation for Patients with Resected Pancreaticobiliary Cancers: A Single Institution Phase II Study (Abstract #325 [10])
The aim of this study was to evaluate the feasibility and safety of adjuvant gemcitabine plus docetaxel followed by radiation with 5-FU after curative resection of pancreatic and biliary adenocarcinomas (Figure 1). They enrolled 50 patients with 30 patients completing therapy. Grade 3-4 nonhematologic toxicities include diarrhea (12%), fatigue (4%), renal failure (2%), hepatic toxicity (4%). Grade 3-4 hematologic toxicities include neutropenia (30%), anemia (2%) and thrombocytopenia (10%). The median overall survival and disease free survival for patients with pancreatic cancer was 17 and 9 months, respectively. They concluded that adjuvant gemcitabine plus docetaxel followed by concurrent 5-FU chemoradiation is feasible and tolerable.
Adjuvant Chemoradiation to Improve Survival Compared to Adjuvant Chemotherapy in Selected Patients with Pancreatic Cancer (Abstract #330 [11])
Figure 1. Schema of the treatment with gemcitabine plus
docetaxel followed by 5-FU and radiation, then followed by two
more cycles of gemcitabine and docetaxel for patients with
curatively resected pancreaticobiliary cancers [10].
This was a single institution review of 343 patients from 2000 to 2012 that underwent a pancreaticoduodenectomy for pancreatic cancer. Patients were placed in 1 of 3 categories. Surgery alone, adjuvant chemotherapy with gemcitabine, or adjuvant 5-FU chemoradiation. Median follow-up and median survival for all patients was 17.5 and 19.5 months, respectively. One-hundred and thirty patients had resection alone, 84 had adjuvant chemotherapy, and 129 had adjuvant chemoradiation. Median survival for were 13, 23 and 26 months for surgery, adjuvant chemotherapy and adjuvant chemoradiation, respectively. Locoregional recurrence was 60%, 63%, and 38% and distant failure was 64%, 65%, and 66%. Chemoradiation group had significantly lower local regional recurrence compared to adjuvant chemotherapy (P=0.01); however, survival between adjuvant chemotherapy and adjuvant chemoradiation was not statistically significant (P=0.23). Median survival of patients with lymph node ratio less than 0.2 and equal to, or greater than, 0.2 was 18 and 27 months, respectively. However, when compared to adjuvant chemotherapy alone, adjuvant chemoradiation improved survival for patients with a positive surgical margin and/or lymph node involvement when the ratio of lymph node positivity to the number of lymph nodes removed was less than 0.2
A Novel Biomarker Panel Examining Response to Adjuvant Pancreatic Cancer Therapy in RTOG 9704 (Abstract #176 [12])
RTOG 9704 was an adjuvant trial in patients with resected disease, randomized to receive 5-FU or gemcitabine chemotherapy given pre- and post-5- FU chemoradiotheray. Serum levels were drawn on all patients prior to adjuvant therapy as stored. A probe panel of available antibodies capable of quantifying 42 key proteins was used in a proximity ligation assay. They were looking if any of these proteins linked with survival or response. As seen in prior studies, decreased levels of CEA and CA 19-9 were prognostic for improved overall survival in all patients. Low levels of matrix metalloproteinase-7 (MMP-7) predicted an overall survival benefit from adjuvant gemcitabine, but not 5-FU (Table 2). This suggests that patients with low MMP-7 serum levels were most likely to benefit from adjuvant gemcitabine and not 5-FU.

Discussion
Adjuvant treatment options for pancreatic adenocarcinoma include fluorouracil (including S- 1), gemcitabine, chemoradiation, and chemoradiation plus fluorouracil or gemcitabine. The Charité Onkologie Clinical (CONKO)-001 and European Study Group for Pancreatic Cancer (ESPAC)-03 studies have shown that chemotherapy can almost double the disease free survival with an improved overall survival compared to observation. Gastrointestinal Study Group (GITSG), ESPAC-1, European Organisation for Research and Treatment of Cancer (EORTC), and RTOG 9407, have shown that the addition of chemoradiation compared to observation alone can improve survival. However, what is the best adjuvant treatment? Which gives the best results is still for debate. To try and answer this question Liao et al. did a meta-analysis of all controlled randomized trials for adjuvant therapy for resected pancreatic cancer [13]. They concluded that fluorouracil or gemcitabine is the most favorable adjuvant treatment, which reduces mortality from cancer after surgery. Chemoradiation plus chemotherapy, either fluorouracil or gemcitabine, is more toxic and less effective in prolonging survival compared to chemotherapy alone.
Cho et al. (Abstract #325 [10]) evaluated a novel approach. Systemic gemcitabine and docetaxel for two treatments followed by 5-FU sensitized radiotherapy and then three more treatments of systemic chemotherapy. Docetaxel is a taxane that is a mitotic inhibitor that affects the microtubules. It is most commonly used for ovarian, breast, prostate and lung cancers. The protocol is shorter than the standard systemic regimens. The study has only 30 patients so it is difficult to come to any conclusions except that it is a tolerable protocol. This novel approach has inferior overall and disease free survival (17 months, and 9 months) compared to the CONKO-001 with single agent chemotherapy (22.1 months, and 13.4 months) or RTOG 9704 with single agent chemotherapy with or without 5-FU based radiotherapy (median survival: 16.8 and 18.8 months).
Kumar et al. (Abstract #330 [11]) tried to clarify what adjuvant therapy would have the most benefit. This retrospective study from a single institution compared observation to two different adjuvant therapy protocols of systemic chemotherapy or chemoradiation after surgical resection. The two adjuvant treatment modalities had an increased survival advantage compared to the observation group. Local recurrence rates were improved with chemoradiation however survival did not change compared to systemic chemotherapy.
One way to address the controversy of different combinations of systemic chemotherapy and chemoradiation is personalized treatment. The follow up RTOG 9704 study used a novel technique to evaluate what combination of biomarkers and adjuvant therapy has the best survival advantage. A protein called matrix metalloproteinase-7 (MMP-7) at lower levels in the serum of patients with resected pancreatic cancers had a better overall survival with systemic gemcitabine than with 5-FU. MMP-7, also known as matrilysin, is frequently overexpressed in human cancer tissues and is associated with cancer progression [14]. MMP-7 has been shown not only in the breakdown of extracellular matrix (ECM) proteins, but also in the regulation of several biochemical processes such as activation, degradation, and shedding of non-ECM proteins to promote cancer progression.
Conflict of interest
The authors have no potential conflicts of interest
References
- American Cancer Society. Cancer Facts & Figures 2013. Atlanta, Ga: American Cancer Society; 2013.
- Saif MW. Controversies in the adjuvant treatment of pancreatic adenocarcinoma. JOP. J Pancreas (Online) 2007; 8:545-52.
- Kalser MH, Ellenberg SS. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg 1985; 120:899-903.
- Klinkenbijl JH, Jeekel J, Sahmoud T, van Pel R, Couvreur ML, Veenhof CH, et al. Adjuvant radiotherapy and 5-fluorouracil after curative resection of cancer of the pancreas and periampullary region: phase III trial of the EORTC gastrointestinal tract cancer cooperative group. Ann Surg 1999; 230:776-82.
- Regine WF, Winter KA, Abrams RA, Safran H, Hoffman JP, Konski A, et al. Fluorouracil vs gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: a randomized controlled trial. JAMA. 2008 Mar 5; 299(9):1019-26. Erratum in: JAMA. 2008 Apr 23/30; 299(16):1902.
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. 2004 Mar 18; 350(12):1200-10.
- Oettle H. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer. JAMA. 2007 Jan 17; 297:267-277.
- Neoptolemos JP, Stocken DD, Bassi C, Ghaneh P, Cunningham D, Goldstein D, et al. Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: a randomized controlled trial. JAMA. 2010 Sep 8; 304(10):1073-81.
- Uesaka K, Fukutomi A, Boku N, Kanemoto H et al. Randomized phase III trial of adjuvant chemotherapy with gemcitabine versus S-1 for patients with resected pancreatic cancer (JASPAC-01 study). J Clin Oncol 30: 2012 (suppl 34; abstr 145).
- Cho M, Wang-Gillam A, Gao F, Linehan D, Hawkins WG, Suresh R, Fournier C, Picus J, Tan B. Adjuvant gemcitabine plus docetaxel followed by 5FU chemoradiation for patients with resected pancreaticobiliary cancers: A single institution phase II study. 2014 Gastrointestinal Cancers Symposium J Clin Oncol 32, 2014 (suppl 3; abstr 325)
- Kumar A, Falk G, Stephans KL, Walsh M, Pelley RJ, Abdel-Wahab M; Adjuvant chemoradiation to improve survival compared to adjuvant chemotherapy in selected patients with pancreatic cancer. 2014 Gastrointestinal Cancers Symposium J Clin Oncol 32, 2014 (suppl 3; abstr 330)
- Heestand GH, Murphy JD, Moughan J, Regine W, Luo J, Graber MS, Kunz PL, Fisher GA, Guha C, Lin B, Mowat RB, Gaur R, Buyyounouski MK, Chen Y, Chang DT, Koong A. A novel biomarker panel examining response to adjuvant pancreatic cancer therapy in RTOG 9704. J Clin Oncol 32, 2014 (suppl 3; abstr 176)
- Liao W, Chien KL, Lin YL, et al. Adjuvant treatments for resected pancreatic adenocarcinoma: a systematic review and network meta-analysis. The Lancet Oncology, Volume 14, Issue 11, Pages 1095 - 1103, October 2013
- Ii M, Yamamoto H, Adachi Y, Maruyama Y, Shinomura Y. Role of matrix metalloproteinase-7 (matrilysin) in human cancer invasion, apoptosis, growth, and angiogenesis. Exp Biol Med (Maywood). 2006 Jan;231(1):20-7.


