Keywords
Chemoradiotherapy; Chemotherapy, Adjuvant; Pancreatic
Neoplasms; Radiotherapy
INTRODUCTION
Scientific societies have tried to define guidelines for
the management of diseases for more than 30 years. For
many oncological diseases, treatment recommendations
according to the tumor stage were developed on the basis
of the results of randomized trials.
Pancreatic carcinoma, for example, is a disease with a
very poor prognosis. 46,420 new diagnoses and 39,590
deaths were reported in the USA in 2014. Up to now, only
10 – 20% of the newly diagnosed patients can be resected
with curative intention. Efforts to prolong survival continue
with a major focus on improving the effectiveness of the
available treatment. According to the current guidelines,
adjuvant chemotherapy is an integral part of the treatment
concept for patients with resected pancreatic cancer
because the 5-year-survival rate rarely exceeds 20% even
after curative resection [1].
One of the most important studies for the
implementation of adjuvant treatment in international
guidelines was the ESPAC-1 trial. This study was designed
in 1993 [2] and included patients with resected pancreatic
cancer who were candidates for adjuvant therapy.
Results of the trial were published in 1997 [3], 2001
[4] and 2004 [5]. All publications drew the conclusion
that adjuvant chemotherapy should be recommended for
patients with advanced, but resectable, pancreatic cancer.
It is the aim of this paper to reevaluate the validity of
this extensively cited prospective, randomized clinical
trial and to analyse whether the results still justify
the recommendation of adjuvant chemotherapy in
international guidelines.
MATERIALS AND METHODS
We used the existing four publications of the ESPAC-1
trial: original study protocol (1993) [2], trial progress
report (1997) [3], interim results (2001) [4] and final
results (2004) [5]. We compared the reported study design,
recruitment period, selection of patients, randomisation,
participating centres, changes in the protocol, homogeneity
of subjects, surgical quality, statistical methods and
evaluation of the results.
Quality-of-life data assessed according to the study
protocol were not included into our reevaluation.
RESULTS
Description of the Original ESPAC-1 Protocol Of 1993
The ESPAC-1 trial was designed as a multicenter
randomized study using a two-by-two factorial design to
investigate whether an adjuvant treatment (chemotherapy
for 6 months with 5-FU and D-L folinic acid versus
radiotherapy with 40 Gray and 5-FU as radiosensitiser or
a combination therapy of both) can improve the 2-year
survival of patients with resected pancreatic cancer.
Inclusion criteria were patients with macroscopically
resected and histologically confirmed adenocarcinoma of
the pancreas, regardless of positive or negative resection
margins and the nodal stage.
Exclusion criteria were ascites, liver metastases, tumor
spread to distant abdominal organs, peritoneal or omental
seedlings or distant metastases, previous or concurrent
malignancies (except basal-cell carcinoma of the skin or
carcinoma in situ of the cervix) and serious medical or
psychological conditions precluding adjuvant therapy.
Randomisation was planned to be performed by the
central Pancreatic Cancer Trial Offices in the UK, Germany
and Switzerland. Patients were randomized in two
steps, first to radiotherapy or observation and second to
chemotherapy or observation. Unfortunately, no details
are reported on these two randomisation steps.
In the primary protocol, a stratification was mentioned
which can be performed according to the presence or
absence of tumour infiltration at the resection margins,
but it was not described whether patients were stratified
before or after randomisation. Furthermore, it was
mentioned that “if a participating surgeon felt strongly that
his patient should not be subjected to combination therapy,
he could choose to randomize between observation and
radiotherapy only or observation or chemotherapy only.”
The trial was designed to show an improvement in
the 2-year-survival rate from 20 to 40% in patients with
negative resection margins and from 1 to 20% in patients
with positive resection margins by one or both of the
adjuvant treatments (chemotherapy and/or radiotherapy).
According to the power calculation, 280 patients were
necessary to answer the study question (Table 1). Given
an alpha of 0.05 and a power of 90% to detect such a
difference, 220 patients with negative resection margins
(55 in each arm) and 60 patients with positive resection
margins (15 in each arm) were required in the 2×2 factorial
design. This design was planned to compare two pairs of
treatment groups in different settings:
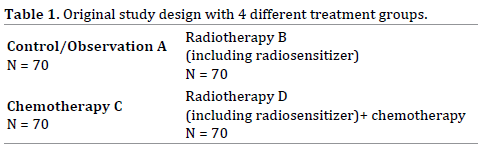
A+B versus C+D (no chemotherapy versus
chemotherapy) and A+C versus B+D (no radiotherapy
versus radiotherapy).
Desription of ESPAC-1 Trial Progress Report 1997
The ESPAC-1 study started in February 1994 and
recruited a total of 348 patients from 49 centers: UK
(n=85), Italy (n=66), Switzerland (n=62), Germany
(n=34), Greece (n=30), Hungary (n=32), Spain (n=19),
Sweden (n=7), Austria (n=7) and France (n=6) until May
31, 1997. Out of these 348 patients, 322 patients had a
ductal adenocarcinoma of the pancreas, and 26 patients
had other types of cancer.
Out of those 322 patients with ductal adenocarcinoma
of the pancreas:
−− 175 were randomized to the 2×2 design (any of the
4 arms),
−− 47 to radiotherapy only (versus control) and
−− 126 to chemotherapy only (versus control).
It was stated that 26 patients with periampullary
cancer were randomized separately. The distribution to
the various treatment arms was illustrated in two tables as
shown here in Table 2.
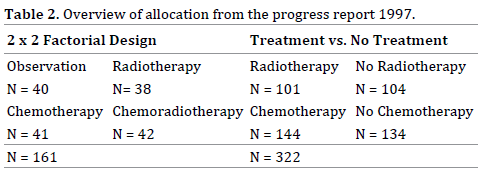
For the N=161 group, it was shown that this is the
number of patients assigned to the two-by-two design
after exclusion of the patients with periampullary cancer,
but the second part of the table is completely confusing
because it summarises N=322 at the buttom, but allocates
a total of 483 patients to different regiments.
The number of 483 patients can be reached if one adds
161 on the left part of the table to 322 on the right part of
the table, but it still remains unexplained why 483 patients
are mentioned when only 348 patients were allocated in
1997.
The data presented become even more confusing
when one realizes that out of 348 patients included in this
randomized trial, only half of them underwent the planned
randomization. One explanation might be the influence
of the individual doctor’s preference allowing a selected
allocation to treatment groups.
This preference could have been institutional (e.g.no
radiotherapy available) or individual (e.g. the patient’s
general condition).
Furthermore, a different section for patients with
periampullary cancer was established separately.The
change in the recruitement strategy was followed by a discussion of the calculated number of patients needed to
complete the trial. As a result, a number of 480 patients
was now calculated.
The paper stated a conflict of interest. Some members
of the ESPAC-1 study group were engaged in clinical trials
sponsored by British Biotech, which produces marimastat
(BB2516), and Lilly Oncology, which produces gemcitabine
(Gemzar).
Description of Interim Results 2001
The interim report describes the survival rates for
patients recruited between February 1994 and April 2000.
The recruitment period was originally planned for two
years, but had to be extended. At least 61 cancer centres
in 11 countries recruited 541 patients with resected
pancreatic cancer. This means that only 1.5 patients were
recruited in each participating centre per year. The paper
declared that, owing to the large number of European
centres involved, a central audit was not performed.
The primary outcome measure was the two-year-survival
rate. Secondary outcomes were the incidence of adverse
effects and recurrences and quality of life. All analyses were
carried out according to the intention-to-treat principle.
As already described in the study progress report,
the study design was changed to allow the inclusion of
additional patients. In this publication, 541 eligible patients
with pancreatic ductal adenocarcinoma were reported to
be randomized as follows:
• 285 patients in the two-by-two factorial design,
• 68 patients in radiotherapy versus no radiotherapy
and
• 188 patients in chemotherapy versus no
chemotherapy.
This strategy led to a variety of subgroups, as shown in Figure 1.
Figure 1. ESPAC-1 trial subgroups according to the interim report 2001.
The term ”radiotherapy” from the original protocoll
in 1993 and the first paper in 1997 was changed to
”chemoradiotherapy” in this publication and the following
in 2004 without further explanation.
The statistical analyses combined patients of the 2×2
design with additional groups. Analysis of the effect of no
radiotherapy vs. radiotherapy showed that the following
groups were included in the statistic: 69+74+35 vs. 70+72+33; resulting in groups of 178 vs. 175 patients.
For evaluation of the effect of no chemotherapy
versus chemotherapy, several subgroups (69+70+96 vs. 74+72+92; 235 vs. 238) also underwent a combined
analysis, so that several subgroups were included twice in
different combinations.
The reader gains the impression from this design that the
study reports on 826 patients (175+178+238+235=826), but
at the time of evaluation, only 541 patients were included,
and 314 events were registered. Median follow-up of the 227
patients still alive was 10 months (range 0-62).
Overall results of the combined group analysis showed
no survival benefit for adjuvant radiotherapy (median
survival 15.5 months in 175 patients with radiotherapy vs. 16.1 months in 178 patients without, p=0.24). Analysis of
the patients included into the two-by-two-factorial design
(N=285) was also interpreted as showing no significant
difference (p=0.09) for the overall survival.
In contrast, adjuvant chemotherapy (median survival
19.7 months in 238 patients with chemotherapy vs. 14.0
months in 235 patients without, p=0.0005) influenced
the outcome significantly, as reported from the combined
group analysis. Surprisingly, the analysis of the twoby-
two factorial design (N=285) could not identify any
survival benefit (p=0.19), but the authors described a nonsignificant
trend.
This interpretation seems to be highly subjective
because the authors consider a p=0.19 to be a nonsignificant
trend, whereas a p=0.09 is declaired to be not
significant.
The main difficulties with the reported data are:
−− The 541 eligible patients were not allocated to a
single, but to three different randomized trials.
−− None of these three trials was analysed separately.
−− Treatment groups derived from three different
trials were combined for the statistical analysis.
Authors’ potential conflicts of interest were not
mentioned.
Description of Final Results 2004
The final results of the ESPAC 1 trial were published
in 2004. The authors focused only on the data of patients
randomized to the two-by-two factorial design. The
paper reports a total of 289 patients in 53 hospitals in
11 European countries (0,9 patients/centre/year) who
underwent randomisation into one of the four treatment
groups between February 1994 and June 2000. At the
time of final analysis, 237 of 289 patients had died, and a
median follow-up of 47 months for 52 surviving patients
was recorded.
For the statistical analysis, two of the randomized
groups were combined and evaluated twice in different
combinations (Figure 2). This kind of evaluation creates
the impression that 588 patients instead of 289 were
evaluated.
Figure 2. ESPAC-1 study groups at final analysis (2004).
While the study was primarily designed to show an
improved survival rate after two years of 20%, the final
report now presents also the 5-year-survival data.
The median survival (95% confidence interval) of the
four different groups was:
16.9 months for observation (12.3 – 24.8; n=69),
13.9 months for radiotherapy (12.2 – 17.3; n=73),
21.6 months for chemotherapy (13.5 – 27.3; n=75) and
19.9 months for radiotherapy+chemotherapy (14.2 –
22.5; n=72).
The corresponding 5-year-survival rates were 11 %,
7%, 29% und 13%.
Whereas the median survival analysis included the 95%
confidence interval, which shows a broad variation in each
of the four groups, the 5-year-survival estimates reported
only mean values, but neither confidence intervals nor
p-values. The reason given for not reporting these data
was a lack of statistical power to compare the four groups
of the two-by-two trial directly.
The no-radiotherapy group seems to have an advantage
if you examine the forrest plot on the hazard ratio for
death comparing radiotherapy (radiation alone or in
combination with chemotherapy) with no radiotherapy
(chemotherapy or observation).
The chemotherapy group seems to have an advantage
if you examine the forrest plot on the hazard ratio for
death comparing chemotherapy (chemotherapy alone or
in combination with radiotherapy) with no chemotherapy
(radiotherapy or observation).
Applying this statistical design with double analyses of
the four patient groups in different settings, a statistically
significant survival benefit was described for patients
assigned to chemotherapy, whereas no significant
benefit for radiotherapy could be shown. This significant
difference in favour of chemotherapy could not be shown
in the interim results after two years in 2001. The different
numbers at risk (285 in 2001 and 289 in 2004) might have
contributed to this difference.
The increase in participating patients is not explained,
but it is obvious that the recruitement period had been
changed. Whereas the publication in 2001 reported
closing the study with recruitment until April 2000, the
2004 paper decribed recruitment until June 2000.
Although the authors declared that a direct comparison
of the four groups was not possible due to a lack of
sufficient statistical power, our recalculation of results
demonstrated the three following significant differences:
Chemotherapy versus Radiotherapy+Chemotherapy:
p=0.0124
Chemotherapy versus Radiotherapy: p=0.0004
Chemotherapy versus Observation: p=0.0088
Three other comparisons show no significant results:
Radiotherapy versus Radiotherapy+Chemotherapy:
p=0.2494
Radiotherapy versus Observation: p=0.3271
Observation versus Radiotherapy+Chemotherapy:
p=0.8689
Dr. Neoptolemos reports having received grant support
from Solvay Pharmaceuticals and KS Biomedix.
DISCUSSION
Pancreatic cancer is still a disease with a very poor
prognosis despite the development of radical operation
techniques, including extended lymphadenectomy,
introduction of perioperative chemotherapy or radiochemotherapy,
improved perioperative intensive care and
improved diagnostic tools during the last 30 years.
Large registries report an improvement in the 5-yearsurvival
rate for all patients from 3% to 8% in the USA or
up to 10% in Japan, but the reasons for this improvement
remain unclear [1, 6].
It was the aim of the ESPAC-1 study to find out if
postoperative chemo-, radio- or chemo-radiotherapy can
improve the survival rate in patients with advanced, but
still resectable, pancreatic cancer.
The published data of the ESPAC-1study convinced
the medical community to recommend postoperative
chemotherapy and to introduce this recommendation into
several European and international guidelines. The ESPAC-
1-Study is cited for example in the following guidelines:
ESMO/ESDO (Europe), S3-AWMF-Guidline (Germany),
KCE (Belgium) and NICE (UK) - each with a high grade of
recommendation [7, 8, 9, 10].
Considering the still poor survival rates for patients
with advanced, but resectable, pancreatic cancer, as well
as reflecting on the current discussion about a “choosing
wisely strategy” to minimize the patients’ risks, especially
for patients with a limited live expectancy, and the
financial burden on healthcare systems, we analysed the
reported data of the ESPAC-1 study in detail to find out
if the study was strong enough to justify the guidelines’
recommendations according to this study.
Our detailed analysis detected the following
weaknesses:
−− Large variability of institutions, unclear
patient selection: 53 hospitals in 11 countries
included patients, no surgical standards defined;
long recruitment period, low recruitment rate
although high-volume centers participated; no
central audit.
−− Changes in protocol: The recruitment period of 2
years was extended to 6 years. The possibility of a
preference-based randomization was introduced.
The primarily prospective randomized trial was
combined with the design of a pragmatic trial.
The observation period - planned for two years -
was extended to five years because no statistical
significance could be observed in the 2 x 2 factorial
design group after two years.
−− Randomization: Introducing a preference-based
study arm could have contributed an additional
sampling bias, which implies that patients with
different risk profiles might have been consciously
assigned to different therapeutic options.
−− Changes in terminology: The term ”radiotherapy”
from the original protocol in 1993 and the first paper
in 1997 was changed to ”chemoradiotherapy” in
the publications in 2001 and 2004 without further
explanation.
−− Questionable study design (2×2 factorial) and
statistical analysis: Since each patient is recorded
in two groups, the information on each patient is
used to answer two questions. This situation is
comparable with a multiple-testing procedure,
which might lead to an overestimation of observed
effects. Another shortcoming of the studies is the
failure to test each individual treatment group,
which was possible as shown above. P-values are
only given for groups in which all patients were
included at least twice.
−− Study question not answered: The study was
established to answer the question whether an
adjuvant therapy is able to increase the survival
rate of patients after pancreatic resections by 20%
after two years. This 20% increase in survival was
presumed for patients with negative, as well as for
patients with positive resection margins, but was
never analysed in the published papers.
Many patients have undergone adjuvant chemotherapy
since the results of the ESPAC-1 trial were published. A
prolongation of the survival interval might have been
achieved in an unknown number of cases, but side effects
with impaired quality of life also occurred. Furthermore
the costs for the healthcare systems have to be taken into
consideration.
It remains unclear whether the response to
chemotherapy and/or the prolonged survival after
resection of advanced tumor stages is more related to the
tumor biology than to a specific treatment option.
Meanwhile two new studies, the ESPAC-4-Study [11]
and the CONKO-001-Study [12], where published on a
similar topic as the ESPAC-1-Study. Unfortunately both
studies show similar lacks of validity like the ESPAC-1-
Study:
The aim of the ESPAC-4-Study was to compare the
combined gemcitabine and capecitabine chemotherapy
with gemcitabine monotherapy in patients with
resected pancreatic cancer. Between 2008 and 2014 372
patients from 98 hospitals were recruited. The result
of the study showed a median overall survival of 28,0
months for patients in the gemcitabine and capecitabine
group compared with 25,5 months for patients in the
gemcitabine monotherapy group (p=0,032). Because each
hospital recruited in average only 1,2 patients per year
a standardized surgical treatment is unlikely and a high
selection bias has to be suspected.
The CONKO-001-Study recruited 368 patients from
88 institutions in Germany and Austria over a period of
6 years. The result showed a significant increase of the
disease free survival time for those patients treated with
gemcitabine for 6 months after pancreatic cancer resection
(13,4 months) compared with an observation group (6,7
months). Again the weakness of the study is the small
number of patients enrolled per year (0.7 patients) by each
institution which might include a selection bias as well as
a lack of probability regarding a standardized operative
treatment.
The Japanese Pancreas Tumor Registry [6] analysed the
courses of several thousands of patients after pancreatic
cancer resections with and without postoperative
chemotherapy. The results show a slight improvement in
the survival rates over the decades, but they are far behind
an improvement of 20% as estimated in the ESPAC-1 trail.
It remains completely unclear how such a result might
have been achieved.
Data from the American Cancer society [1] also show
a minimal improvement of the survival rates over the
last decade but many factors, like standardization of
the operative procedure, the anesthesia, perioperative
management and technical developments might have
contributed to the progress despite the introduction of
adjuvant therapy.
The aim of our detailed analysis of the ESPAC-1-Study
was to take a critical look on the validity of that study
which is still mainly cited in many guidelines as a reference
for the recommendation of adjuvant treatment in patients
after resection of pancreatic cancer.
We therefore conclude that, according to the weakness
of the study, as well as more than 10 years of clinical
experience in the meantime, the recommendation for
adjuvant chemotherapy after resection of pancreatic
cancer has to be re-evaluated. Stratification according to
defined risk factors, like tumor characteristics, should be
introduced to identify possible responders to therapy and
thereby reduce the number of unnecessary treatments,
particularly because the clinical approach to oncological
patients has switched from standardized to personalized
medicine.
SUMMARY
We focused on the ESPAC-1-Study because in many
European and international guidelines this study is still
basis of the recommendation of adjuvant chemotherapy
after resection of pancreatic cancer. Our detailed analysis
of the ESPAC-1 trial revealed several shortcomings and
inconsistencies in the study design, patient selection,
randomization, statistical methods, recruitment period
and interpretation of the results. The conclusion is that a
general benefit from adjuvant chemotherapy in resectable
pancreatic cancer cannot be derived from this study.
Conflict of Interest
For non of the three authors exists a conflict of interests.
References
- https://www.cancer.org/research/cancer-facts-statistics.html
- Original study protocol of the ESPAC-1 trial on the adjuvant therapy
in operable pancreatic cancer. European Study Group for pancreatic
cancer 1993.
- Neoptolemos JP, Kerr DJ, Beger H, Link K, Pederzoli P, Bassi C, et
al. ESPAC-1 trial Progress report: The European randomized adjuvant
study comparing radiochemotherapy, 6 months chemotherapy and
combination therapy versus observation in pancreatic cancer. Digestion
1997; 58:570-7. [PMID: 9438604]
- Neoptolemos JP, Dunn JA, Stocken DD, Almond J, Link K, Beger H, et al.
Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic
cancer: a randomised controlled trial. Lancet 2001; 358:1576-85.
[PMID: 11716884]
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al.
A randomized trial of chemoradiotherapy and chemotherapy after resection
of pancreatic cancer. N Engl J Med 2004; 350:1200-10. [PMID: 15028824]
- Matsuno S, Egawa S, Fukuyama S, Motoi F, Sunamura M, Isaji S, et
al. Pancreatic Cancer Registry in Japan: 20 Years of Experience. Pancreas
2004; 28:219-30. [PMID: 15084961]
- Ducreux M, Cuhna AS, Caramella C, Hollebecque A, Burtin P, Goere
D, et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for
diagnosis, treatment and follow-up. Ann Oncol 2015; 26(Supplement 5):
v56–v68. [PMID: 26314780]
- www.awmf.org/uploads/tx_szleitlinien/032-010OLl_S3_Exokrines_
Pankreaskarzinom_21112013.pdf
- https://kce.fgov.be/about-kce
- https://www.nice.org.uk/guidance/indevelopment/gidcgwave0802
- Neoptolemos JP, Palmer DH, Ghaneh P, Psarelli EE, Valle JW, Halloran
CM, et al. Comparison of adjuvant gemcitabine and capecitabine with
gemcitabine monotherapy in patients with resected pancreatic cancer
(ESPAC-4): a multicentre, open label, randomised, phase 3 trial. Lancet
2017; 389:1011-24. [PMID: 28129987]
- Oettle H, Neuhaus P, Hochhaus A, Hartmann JT, Gellert K, Ridwelski K,
et al. Adjuvant Chemotherapy With Gemcitabine and Long-term Outcomes
Among Patients With Resected Pancreatic Cancer: The CONKO-001
Randomized Trial. JAMA 2013; 310:1473-1481. [PMID: 24104372]



