Saurabh Chawla*, Mary Jo Atten, Bashar M Attar
Division of Gastroenterology, John H. Stroger Hospital of Cook County and Rush University Medical School. Chicago, IL, USA
- *Corresponding Author:
- Saurabh Chawla
Division of Gastroenterology
Stroger Hospital of Cook County
1901 West Harrison Street; Chicago
IL 60612; USA
Phone: +1-312.864.7213
Fax: +1-312.864.9624
E-mail: chawlasaurabh@yahoo.co.in
Received: December 14th, 2010 Accepted: January 13th, 2011
Context Vasculitis is a known cause of pancreatitis and other gastrointestinal symptoms; however, most of these patients have medium vessel vasculitis like polyarteritis nodosa and often there are other associated conditions like hepatitis B or clinical manifestations that suggest the diagnosis. Wegener’s granulomatosis is predominantly a reno-pulmonary disorder, rarely having gastrointestinal manifestations. Case report We report a case of Wegener’s granulomatosis initially presenting as acute pancreatitis and then rapidly progressing to severe multi-organ involvement over the next few months. Discussion Pancreatic association as an initial presentation of Wegener’s granulomatosis is limited to only a few reports. This extremely rare initial presentation makes the diagnostic process challenging. Two different pancreatic manifestations have been reported: as a pancreatic mass mimicking a tumor or as acute pancreatitis. The patients who presented as pancreatic head masses underwent extensive surgical procedures before the diagnosis was established. Acute pancreatitis as the initial presentation is usually associated with an aggressive course of the vasculitis and often results in a fatal outcome. Conclusions This case illustrates Wegener’s granulomatosis as a rare cause of acute pancreatitis. It emphasizes the need for thorough continued systemic clinical evaluation of patients when the etiology is not readily evident. Also, since most patients with pancreatitis due to Wegener’s granulomatosis rapidly progress to severe multiorgan involvement, knowledge of a broad differential of potential etiologies and a low index of suspicion is required for timely diagnosis and treatment. INTRODUCTION
Keywords
Pancreatitis, Acute Necrotizing; Vasculitis; Wegener Granulomatosis
INTRODUCTION
Less common causes of acute pancreatitis are sought in patients after etiologies like gallstones and alcohol have been ruled out. When search of the easily investigated causes of acute pancreatitis, like hypercalcemia and hypertriglyceridemia, is exhausted, the focus is directed to possible autoimmune pancreatitis or classified as idiopathic pancreatitis. Vasculitis, especially Wegener’s granulomatosis is a rare cause of acute pancreatitis and is difficult to diagnose without other systemic manifestations. Since most patients with acute pancreatitis as the initial manifestation of Wegener’s granulomatosis tend to rapidly progress to multi-organ involvement, sometimes with a fatal outcome, knowledge of this association is important for timely and possibly life saving treatment. We report a case of Wegener’s granulomatosis initially presenting as acute pancreatitis and review the literature on similar presentations.
CASE REPORT
A 60-year-old previously healthy woman presented to our hospital with a one-week history of epigastric pain associated with nausea and vomiting. The review of systems was unremarkable. She denied use of alcohol or herbal medications or a history of biliary disease. On physical exam, she had a heart rate of 111 beats per minute and epigastric tenderness. Initial biochemical investigations revealed an elevated WBC count (12,300 dL-1; reference range: 4,400-10,600 dL-1) with 82.0% neutrophils (reference range: 45.3-74.5%) and lipase (1,316 IU/L; reference range: 5-50 IU/L). Her hemoglobin and liver chemistries were within normal limits. A CT scan of the abdomen revealed a diffusely edematous pancreas and a possible hypoattenuated lesion in the head of the pancreas with peripancreatic inflammatory changes; the gallbladder and common bile duct appeared normal. A diagnosis of mild acute pancreatitis was made and since no etiology was identified, endoscopic ultrasound (EUS) was performed to evaluate the common bile duct and pancreatic head. EUS revealed two small heterogeneous hypoechoic lesions in the head and the tail of pancreas and changes suggestive of acute pancreatitis. The common bile duct was found to be normal. Aspiration cytology was performed from the pancreatic lesions at the time of EUS and revealed inflammatory cells with no evidence of malignancy. She improved on symptomatic treatment and was discharged home. She had a stormy course over the next two months, first developing a pulmonary embolism, then a myocardial infarction secondary to emboli to her myocardial arteries. She then developed complete heart block requiring permanent pacing and finally central diabetes insipidus with MRI showing pituitary dysfunction and maxillary sinusitis. During this period she was noted to have intermittent hematuria and cavitary lung lesions, so she was thought to have a vasculitic cause for this constellation of findings, and further workup revealed decreased complement levels, elevated antineutrophil cytoplasmic antibody (c-ANCA) (titer 1:160) and elevated proteinase 3 levels (45.1 U/mL; reference range: 0-3.5 U/mL). The diagnosis of Wegener’s granulomatosis was confirmed by a renal biopsy that showed pauciimmune focal necrotizing glomerulonephritis. She was given a three dose course of pulse steroids, followed by oral prednisone and cyclophosphamide. Both of these were tapered over the next 6 months as she went into remission. She has since been maintained on azathioprine and is now doing well at 10 months of follow-up.
DISCUSSION
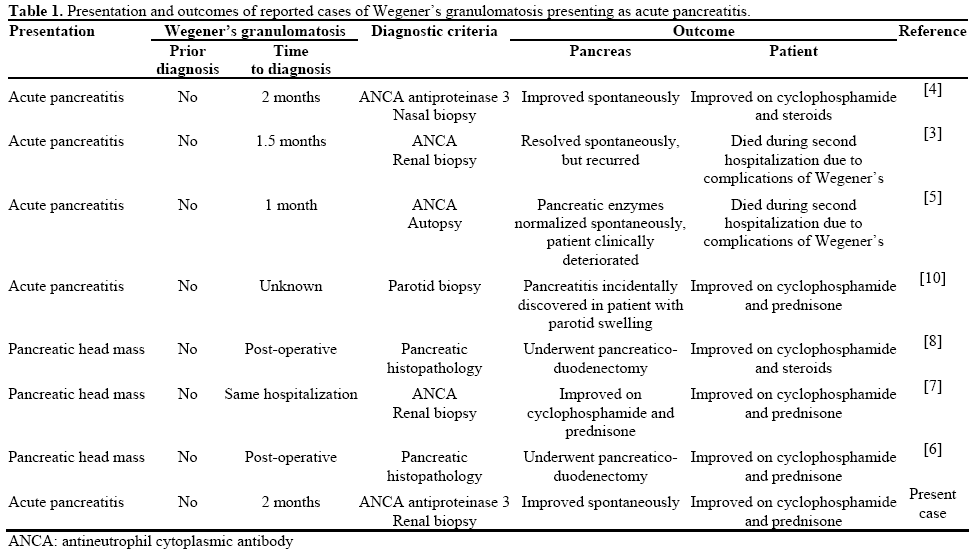
Vasculitis is known to involve the pancreas and gastrointestinal tract; however, most of these patients have medium vessel vasculitis like polyarteritis nodosa, and often there are other associated conditions like hepatitis B or other clinical manifestations that suggest the diagnosis [1]. Wegener’s granulomatosis is predominantly a reno-pulmonary disorder, rarely having gastrointestinal manifestations [2]. Pancreatitis as an initial presentation is limited to only a few reports [3, 4, 5, 6, 7, 8, 9]. Two different pancreatic manifestations have been reported: as a pancreatic mass mimicking a tumor [6, 7], and more rarely as acute pancreatitis [3, 4, 5]. This extremely rare initial presentation makes the diagnostic process challenging. Therefore, in most of these reports, as in our case, the diagnosis was established over time after patients developed other manifestations of the disease and met the criteria needed for diagnosis of Wegener’s granulomatosis [9]. All patients who presented initially with pancreatitis had a rapidly progressive course of disease and three patients had a fatal outcome because of fulminant progression of Wegener’s granulomatosis [3, 5] (Table 1). Patients who presented as pancreatic head masses underwent extensive surgical procedures before the diagnosis was established [6, 8].
This case illustrates Wegener’s granulomatosis as a rare cause of acute pancreatitis. It emphasizes the need for thorough and continued systemic clinical evaluation of patients when the etiology of pancreatitis is not readily evident. Since most patients with pancreatitis due to Wegener’s granulomatosis rapidly progress to severe multi-organ involvement, knowledge of a broad differential of potential etiologies and a low index of suspicion is required for timely diagnosis and treatment.
Conflict of interest
The authors have no potential conflicts of interest
References
- Pagnoux C, Mahr A, Cohen P, Guillevin L. Presentation and outcome of gastrointestinal involvement in systemic necrotizing vasculitides: analysis of 62 patients with polyarteritisnodosa, microscopic polyangiitis, Wegener granulomatosis, Churg-Strauss syndrome, or rheumatoid arthritis-associated vasculitis. Medicine (Baltimore) 2005; 84:115-28. [PMID 15758841]
- Pinkney JH, Clarke G, Fairclough PD. Gastrointestinal involvement in Wegener's granulomatosis. Gastrointest Endosc 1991; 37:411-2. [PMID 2071011]
- Abu-Hilal M, Abu-Hilal M, McPhail MJ, Zeidan B, Bryant T, Bateman A, Johnson CD. Acute pancreatitis as the first presentation of Wegener's granulomatosis. JOP J Pancreas (Online) 2008; 9:300- 4. [PMID 18469442]
- Joshipura VP, Haribhakti SP, Pandya SC, Soni HN, Patel NR. Wegener's granulomatosis--an etiology of acute pancreatitis. Indian J Gastroenterol 2007; 26:89-90. [PMID 17558075]
- Matsubayashi H, Seki T, Niki S, Mizumura Y, Taguchi Y, Moriyasu F, Go K. Wegener's granulomatosis with onset of acute pancreatitis and rapid progress. A case report. Pancreatology 2001; 1:263-6. [PMID 12120205]
- Christl SU, Borchard F, Keller R, Engemann R, Fischbach W. Pancreatic tail tumor as an unusual first manifestation of Wegener's disease. Z Gastroenterology 2004; 42:513-6. [PMID 15190447]
- O'Neil KM, Jones DM, Lawson JM. Wegener's granulomatosis masquerading as pancreatic carcinoma. Dig Dis Sci 1992; 37:702-4. [PMID 1563310]
- Tinazzi I, Caramaschi P, Parisi A, Faccioli N, Capelli P, Biasi D. Pancreatic granulomatous necrotizing vasculitis: A case report and review of the literature. Rheumatol Int 2007; 27:989-91. [PMID 17265156]
- Leavitt RY, Fauci AS, Bloch DA, Michel BA, Hunder GG, Arend WP, et al. The American College of Rheumatology 1990 criteria for the classification of Wegener's granulomatosis. Arthritis Rheum 1990; 33:1101-7. [PMID 2202308]
- Stuckey SL, Smart PJ. Wegener's granulomatosis: Parotid involvement and associated pancreatitis with CT findings. Australas Radiol 1992: 36:343-6. [PMID 1299199]

