Keywords
Carcinoma, Acinar Cell; Pancreas; Pancreatectomy; Panniculitis
INTRODUCTION
Subcutaneous panniculitis is a rare cutaneous eruption associated with pancreatic disease in 0.3-3% of cases [1]. Acinar cell carcinoma is a very rare malignant tumor, accounting for approximately 1-2% of primary pancreatic neoplasms [2, 3]. Although acinar pancreatic carcinoma is present in a small proportion of patients with pancreatic cancer, more than one-half of those with subcutaneous fat necrosis have this type of pancreatic malignancy [4]. Pancreatic panniculitis presents with ill-defined erythematous subcutaneous nodules located mainly on the legs. It may be associated with arthropathy, synovitis, osteolytic bone lesions and polyserositis. The pathogenesis of pancreatic panniculitis is still unknown, but it is believed to be associated with high levels of serum lipase produced by the neoplasm, causing fat necrosis in tissues [5].
We present the case of a 79-year-old woman with pancreatic acinar cell carcinoma who developed subcutaneous panniculitis on both legs.
CASE REPORT
In October 2008, a 79-year-old woman presented with an episode of acute pancreatitis and she was admitted to another hospital. Abdominal CT scan revealed an enlarged pancreatic head with the presence of an inhomogeneous, hypodense area in the uncinate process 1.5x3.0 cm in diameter. Tumor markers, including carcinoembryonic antigen (CEA) and CA 19- 9, were within the normal range. A cytologic sample derived from fine-needle percutaneous aspiration of the pancreas was inconclusive. The pancreatic lesion was interpreted as a consequence of the acute pancreatitis, and was not confirmed at a CT scan performed 3 months later.
In February 2009, the patient underwent a radical left mastectomy and right quadrantectomy for bilateral mammary invasive carcinoma (pT2 N1 M0; grade 2), followed by adjuvant radiotherapy and hormonal therapy. During the follow-up, an abdominal CT scan (August 2009) revealed a solid, ovoidal lesion (6.5x4.0 cm in diameter) in the pancreatic head, involving the uncinate process.
She underwent upper digestive endoscopy and endoscopic ultrasound (EUS) which revealed the presence of a large, solid mass localized in the pancreatic head, infiltrating the duodenal wall. A cytological examination of the lesion under EUS guidance was negative for neoplastic cells. A new CT scan revealed an enlargement of the pancreatic mass (9x5x8 cm in diameter) with infiltration of the duodenum (Figure 1).
Figure 1. Abdominal CT scan showing a large and solid mass
(9x5x8 cm in diameter) located in the head of the pancreas.
In October 2009, the patient complained of multiple painful migrant nodules, with erythematous skin, on her lower extremities which were explained as erythema nodosum or paraneoplastic syndrome (Figure 2). The patient was treated with steroids, without benefit.
Figure 2. Multiple erythematous subcutaneous nodules on the lower
legs.
In November 2009, after a second episode of acute pancreatitis, the patient was referred to our department. Laboratory investigations showed a hemoglobin concentration of 8.3 g/dL (reference range: 14.0-17.5 g/dL), amylase of 113 U/L (reference range: 0-53 U/L) and lipase of 1,508 U/L (reference range: 0-60 U/L). CEA, CA 19-9 and alpha-fetoprotein were within the normal range. Upper digestive endoscopy confirmed the presence of an ulcerated mass infiltrating the second duodenal portion, with evidence of recent bleeding. The endoscopic biopsy of the mass was positive for adenocarcinoma (grade 2-3) of pancreatic origin with widespread necrotic areas. A biopsy of the subcutaneous nodule confirmed the presence of areas of necrotic subcutaneous fat surrounded by chronic inflammation consistent with pancreatic panniculitis (Figure 3).
Figure 3. Skin biopsy, lower leg: lobular fat necrosis with
characteristic “ghost cells” and a mixed inflammatory infiltrate at the
margin of saponification (H&E).
In December 2009, the patient underwent a pyloruspreserving pancreaticoduodenectomy. Histopathological examination showed an acinar cell carcinoma with angiolymphatic invasion and infiltration of the duodenal wall (pT3 N0 M0; R0) (Figure 4). After surgery, there was regression of the subcutaneous nodules (Figure 5) with normalization of the serum lipase levels.
Figure 4. Microscopic findings show an acinar pattern, with the
neoplastic cells arranged in small glandular units. Within the
glandular units, cellular polarization is evident (H&E).
Figure 5.Right lower leg: regression of subcutaneous panniculitis
after surgery.
The postoperative course was complicated by a biliary and enterocutaneous fistula which was successfully treated with percutaneous drainage under radiologic guidance. A PET/CT scan carried out in June 2010 revealed the presence of multiple liver metastases. Serum lipase levels were 241 U/L. The patient underwent chemotherapy with gemcitabine, and she is still alive 14 months after resection.
DISCUSSION
Panniculitis is defined as a painful cutaneous nodule which arises from an inflammatory reaction in the subcutaneous fat in association with erythema nodosum, erythema induratum, Weber-Christian panniculitis, lupus panniculitis, alpha-1-antitrypsin deficiency and pancreatic disease including pancreatic neoplasm [6]. The association between pancreatic disease and subcutaneous fat necrosis was first described by Chiari in 1883 [7]. When associated with a pancreatic tumor, the combination of subcutaneous fat necrosis, polyarthritis and eosinophilia is known as Schmid’s triad [8]. The skin manifestation can precede, occur concurrently with or follow the pancreatic pathology [9, 10]. The subcutaneous nodules associated with pancreatic disease may be painful or painless. They may occur anywhere but most commonly develop on the lower legs [11]. The clinical presentation of panniculitis includes erythematous, illdefined reddish-brown nodules which can also appear on the arms, trunk, thighs and breast. Distinctive laboratory values include eosinophilia and elevated serum lipase levels [12]. The pathogenesis of pancreatic panniculitis is not fully understood, but it is thought to result from the saponification of fat secondary to the action of liberated pancreatic lipase and elastase I [5]. Pancreatic panniculitis is characterized histopathologically by lobular fat necrosis with anuclear adipocytes, called ghost cells, within a thick, shadowy wall. Focal calcification and a mixed inflammatory infiltrate may also be seen [13].
Pancreatic panniculitis can be associated with pancreatic malignant tumors (acinar cell carcinoma in 80% of the cases), and with acute or chronic pancreatitis [14]. Acinar cell carcinoma accounts for only 1% of all pancreatic tumors. It is defined as a carcinoma exhibiting pancreatic enzyme production by neoplastic exocrine cells, and its clinical presentation is usually related either to the local effects of the tumor or to metastasis [14]. It occurs predominantly in middleaged people (male:female ratio of 2:1), but can also occur in the pediatric population [2]. The presenting symptoms are usually nonspecific. The most common presentation is abdominal pain, with a palpable abdominal mass. Jaundice is infrequent [14]. Acinar cell carcinoma may induce local, regional and focally disseminated fat necrosis. Klimstra et al. [15] reported panniculitis and high serum lipase levels in 14% (4/28) of cases of pancreatic acinar cell carcinoma. In our patient, there was a diagnostic delay of more than one year between the first episode of pancreatitis and surgical treatment; an attempt to obtain a cytological diagnosis under endoscopic ultrasound guidance (EUSFNA) was unsuccessful, although EUS-FNA has been considered a highly sensitive and specific method for the preoperative work-up of pancreatic masses. Nevertheless, false negative results may occur, depending on the tumor diameter, number of tissue samples and expertise of the operator. He pancreatic panniculitis appeared one year after the onset of symptoms. Clinicians should be aware that panniculitis may be the sentinel of serious pancreatic disease, such as pancreatic cancer, and may precede the usual manifestations of these conditions [16]. Only a minority of cases of subcutaneous panniculitis are associated with pancreatic disease. However, in the presence of a pancreatic mass, as in our case, the diagnosis of acinar cell carcinoma should strongly be considered. The treatment of pancreatic panniculitis consists of surgical intervention, whenever possible, which may lower lipase levels and result in regression of the skin lesions [13]. The prognosis of acinar cell carcinoma is generally considered poor, although better survival as compared to ductal adenocarcinoma has also been reported [2, 3, 15].
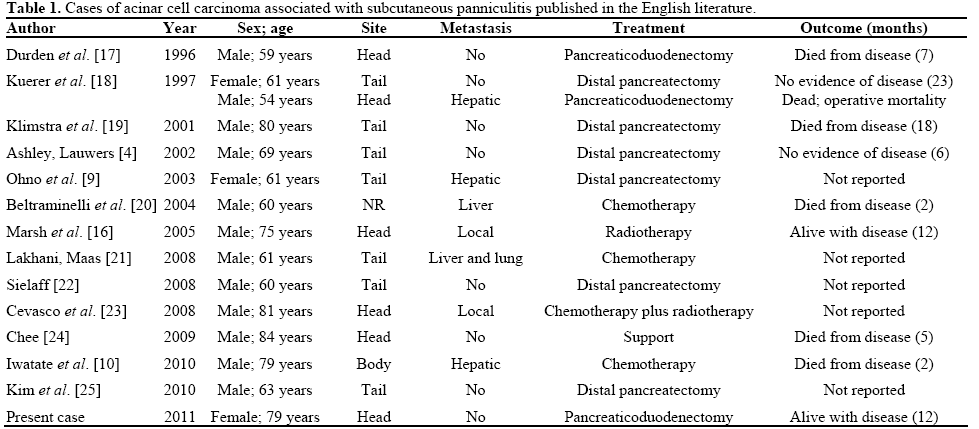
In a review of the literature, we found 15 cases (including our patient) of acinar cell carcinoma and subcutaneous panniculitis [4, 9, 10, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25] (Table 1). There were 12 males, and the mean age at presentation was 63.0 years (range: 59- 84 years). Pancreatic panniculitis occurred before the diagnosis of pancreatic cancer in 9 patients (at a median of 4 months, range: 1-12 months), was present at diagnosis in three patients, and occurred after diagnosis in one patient. In two patients, this information was lacking. In six cases, the tumor was located in the head of the pancreas; five tumors were metastatic and two were locally advanced at presentation. All patients presented with high serum lipase levels. Nine patients underwent a pancreatectomy, five chemo- or radio-therapy, and one supportive therapy only. There was one operative mortality. The follow-up was very short, ranging from 2 to 23 months; only four patients are alive (two with disease) 6, 12, 14, and 23 months after treatment, respectively. The presence of the subcutaneous manifestation seems to be associated with decreased survival, probably reflecting greater aggressiveness of the tumor. In the study of Klimstra et al. [15], mean survival of patients with lipase-secreting acinar cell carcinoma was 8.8 months, considerably worse than the survival of patients without the syndrome (20.0 months; P<0.05). In our case, the maximum tumor diameter increased from 3.0 to 9.0 cm after 11 months. So, the doubling time, based on the Schwartz formula [26] was 70 days, confirming the aggressive behavior of the neoplasm. Early recognition and neo-adjuvant therapy could be useful in improving the clinical management of this type of cancer.
In conclusion, acinar cell carcinoma is a rare tumor and its preoperative diagnosis is difficult. Although subcutaneous fat necrosis can occur late in the course of the disease, recognition of the association between subcutaneous panniculitis and a pancreatic neoplasm may prevent a long delay in the diagnosis and management of this malignancy.
Conflict of interest
The authors have no potential conflicts of interest
References
- Bogart MM, Milliken MC, Patterson JW, Padgett JK. Pancreaticpanniculitis associated with acinic cell adenocarcinoma: a case reportand review of the literature. Cutis 2007; 80:289-94. [PMID18038690]
- Kitagami H, Kondo S, Hirano S, Kawakami H, Egawa S, TanakaM. Acinar cell carcinoma of the pancreas: clinical analysis of 115patients from the Pancreatic Cancer Registry of Japan PancreasSociety. Pancreas 2007; 35:42-6. [PMID 17575544]
- Schmidt CM, Matos JM, Bentrem DJ, Talamonti MS, LillemoeKD, Billimoria KY. Acinar cell carcinoma of the pancreas in theUnited States: prognostic factors and comparison to ductaladenocarcinoma. J GastrointestSurg 2008; 12:2078-86. [PMID18836784]
- Ashley SW, Lauwers GY. Case records of the MassachusettsGeneral Hospital. Weekly clinicopathological exercises. Case 37-2002. A 69-year-old man with painful cutaneous nodules, elevatedlipase levels, and abnormal results on abdominal scanning. N Engl JMed 2002; 347:1783-91. [PMID 12456855]
- Heykarts B, Anseuw M, Degreef H. Panniculitis caused byacinous pancreatic carcinoma. Dermatology 1999; 198:182-3. [PMID10325476]
- Phelps RG. Shoij T. Update on panniculitis. Mt Sinai J Med2001; 68:262-7. [PMID 11514913]
- Chiari H. ÜberdiesogenannteFettnekrose. Prager MedWocheschr 1883; 8:285-6.
- Schmid M. The syndrome of metastasizing exocrine pancreasadenoma with secretory activity. Z Klin Med 1957;154:439-55. [PMID 13456796]
- Ohno Y, Le Pavoux A, Saeki H, Asahina A, Tamaki K. A caseof subcutaneous nodular fat necrosis with lipase-secreting acinar cellcarcinoma. Int J Dermatol 2003; 42:384-5. [PMID 12755979]
- Iwatate M, Matsubayashi H, Sasaki K, Kishida N, Yoshikawa S,Ono H, Maitra A. Functional pancreatic acinar cell carcinomaextending into the main pancreatic duct and splenic vein. JGastrointest Cancer 2010; Aug 12. [PMID 20703831]
- Dahl PR, Su WP, Cullimore KC, Dicken CH. Pancreaticpanniculitis. J Am AcadDermatol 1995; 33:413-7. [PMID 7657863]
- Shbeeb MI, Duffy J, Bjornsson J, Ashby AM, Matteson EL.Subcutaneous fat necrosis and polyarthritis associated withpancreatic disease. Arthritis Rheum 1996; 39:1922-5. [PMID8912516]
- Martin SK, Agarwal G, Lynch GR. Subcutaneous fat necrosis asthe presenting feature of a pancreatic carcinoma: the challenge ofdifferentiating endocrine and acinar pancreatic neoplasms. Pancreas2009; 38:219-22. [PMID 19238022]
- Chiou YY, Chiang JH, Hwang JI, Yen CH, Tsay SH, Chang CY.Acinar cell carcinoma of the pancreas: clinical and computedtomography manifestations. J Comput Assist Tomogr 2004; 28:180-6. [PMID 15091120]
- Klimstra DS, Heffess CS, Oertel JE, Rosai J. Acinar cellcarcinoma of the pancreas: a clinicopathologic study of 28 cases. AmJ SurgPathol 1992; 16:815-37. [PMID 1384374]
- Marsh R de W, Hagler KT, Carag HR, Flowers FP. Pancreaticpanniculitis. Eur J SurgOncol 2005; 31:1213-5. [PMID 16099617]
- Durden FM, Variyam E, Chren MM. Fat necrosis with featuresof erythema nodosum in a patient with metastatic pancreaticcarcinoma. Int J Dermatol 1996; 35:39-41. [PMID 8838928]
- Kuerer H, Shim H, Pertsemidis D, Unger P. Functioningpancreatic acinar cell carcinoma: immunohistochemical andultrastructural analyses. Am J ClinOncol 1997; 20:101-7. [PMID9020300]
- Klimstra DS, Adsay NV. Acinar cell carcinoma of the pancreas:a case associated with the lipase hypersecretion syndrome. PatholCase Rev 2001; 6:121-6. [PMID 1384374]
- Beltraminelli HS, Buechner SA, Hausermann P. Pancreaticpanniculitis in a patient with an acinar cell cystadenocarcinoma ofthe pancreas. Dermatology 2004; 208:265-7. [PMID 15118385]
- Lakhani A, Maas L. Necrotizing panniculitis: a skin conditionassociated with acinar cell carcinoma of the pancreas. South Med J2008; 101; 554-5. [PMID 18414166]
- Sielaff T. The telitale rash. A man with pretibial erythema. MinnMed 2008; 91:45-6. [PMID 19108548]
- Cevasco M, Rodriguez JR, Fernandez-del Castillo C. ClinicalChallenges and images in GI: pancreatic acinar cell carcinoma withsubcutaneous fat necrosis. Gastroenterology 2008; 135:1054. [PMID18789332]
- Chee C. Panniculitis in a patient presenting with a pancreatictumor and polyarthritis: a case report. J Med Case Reports 2009; 3:7331. [PMID 19830189]
- Kim KA, Kim MJ, Jang SJ. A pancreatic mass presented withmultiple hot spots in the subcutaneous fat layer on positron emissiontomography. Gastroenterology 2010; 139:e10-1. [PMID 20800656]
- Schwartz M. A biomathematical approach to clinical tumorgrowth. Cancer 1961; 14:1272-94. [PMID 13909709]






