Keywords
Acetaminophen; Acidosis; Pancreatitis
INTRODUCTION
Drugs are a relatively rare cause of acute pancreatitis, with an estimated incidence of 0.1-2% [1, 2] and more than 100 drugs have been implicated in causing the disease. Acetaminophen has been linked to acute pancreatitis; however, there have only been five case reports [3, 4, 5, 6, 7]. In this report, we present a rare case of recurrent episodes of acute pancreatitis and metabolic acidosis which may have been caused by an acetaminophen overdose.
CASE REPORT
A 35-year-old woman (height 146 cm, weight 38 kg, BMI 17.8 kg/m2) reported severe pain in the lower limbs after experiencing high levels of stress which led to prolonged abuse of the analgesic drug, Naron® (Taisho Pharmaceutical Co., Ltd, Tokyo, Japan). Naron® is readily available on the market in Japan. The drug contains acetaminophen (265 mg acetaminophen in two tablets). Beginning in 2004, the patient experienced a buildup of stress relating to her working and home environment. She had no history of alcohol dependence, but she had a history of depression for which she attended a mental clinic. Beginning in November 2004, she began to take 30-40 tablets of the analgesic drug everyday. Early in December 2004, she presented appetite loss, upper abdominal pain and finally showed difficulty in breathing. She was then admitted to our hospital. On admission, she had a high fever of 40°C, tachycardia (170 min-1) and tachypnea (35 min-1). She had no skin rash or lymphadenopathy. Her blood pressure was 80/60 mmHg and she presented marked delirium. Initially, we could not obtain any information regarding her medical history from her or her family. Laboratory examination revealed: white cell blood count 24,390 mm-3 (reference range: 4,000-8,000 mm-3), neutrophils were dominant and the eosinophil count was 0.0% (reference range: 0-10%); red cell blood count 4,460,000 mm-3 (reference range: 3,800,000-4,800,000 mm-3); hemoglobin 15.4 g/dL (reference range: 11.3-15.2 g/dL); and platelet count 387,000 mm-3 (reference range: 150,000-380,000 mm-3). The serum amylase level was 1,414 IU/L (reference range: 37-125 IU/L), serum total protein level 6.9 g/dL (reference range: 6.7-8.3 g/dL), total bilirubin level 0.6 mg/dL (reference range: 0.3-1.2 mg/dL), aspartate aminotransferase level 75 IU/L (reference range: 13-33 IU/L), alanine aminotransferase level 28 IU/L (reference range: 6-27 IU/L), alkaline phosphatase level 368 IU/L (reference range: 115-359 IU/L), gamma-glutamyl transferase level 445 IU/L (reference range: 10-47 IU/L), lactate dehydrogenase level 549 IU/L (reference range: 119-229 IU/L), blood urea nitrogen level 18.6 mg/dL (reference range: 8-22 mg/dL), creatinine level 1.1 mg/dL (reference range: 0.4-0.7 mg/dL), calcium level 8.1 mg/dL (reference range: 8.7-10.3 mg/dL), glucose level 72 mg/dL (reference range: 70-110 mg/dL) and C-reactive protein level 24.4 mg/dL (reference range: 0-0.3 mg/dL). Prothrombin time was 17.5 sec (49%; reference range: 9.0-14.9 sec) and a blood gas test revealed marked metabolic acidosis: a pH level of 7.04 (reference range: 7.36-7.44) and base excess of -14.4 mEq/L. Elevation of the level of serum non-specific IgE was not detected. A computed tomography (CT) examination revealed a mild swelling of the total pancreas and fluid collection around the pancreas, but there was no pancreatic necrosis (Figure 1a). Although there was some discrepancy between her symptoms, the laboratory data and the findings of the abdominal CT, we diagnosed severe acute pancreatitis with 17 points in the APACHE II score and 13 points in the Japanese Severity Score [8]. In the intensive care unit (ICU), she was electively intubated and ventilated, and 1,400 mg/day of gabexate mesilate were administered intravenously. For the severe metabolic acidosis, she also received continuous hemodiafiltration. Her vital signs and the laboratory data showed that she improved dramatically and she was discharged from the ICU after 7 days. The CT findings on the sixth day (Figure 1b) demonstrated that the fluid collection had disappeared but the mild pancreatic swelling remained. MRCP examination revealed no hepatobiliary abnormalities, including stones, and ERCP revealed no anatomical abnormalities in the main pancreatic duct, such as pancreatic divisum. She did not demonstrate hypertriglyceridemia or hypercalcemia during the entire clinical course. Autoimmune pancreatitis was excluded owing to no elevation of serum IgG or IgG4 levels, and no features of endoscopic retrograde pancreatography findings suggesting autoimmune pancreatitis. She had not ingested any other drugs including antidepressants for about one month before admission. Therefore, we concluded that an overdose of the drug containing acetaminophen may have caused the acute pancreatitis with severe metabolic acidosis. After hospital discharge, she attended the mental clinic again and had no abdominal pain for a while. Two months later, a CT showed that there was an improvement in the pancreatic swelling (Figure 1c). However, the patient gradually felt stress in her home environment, and felt the same pain as before in the lower limbs and, beginning in March 2005, started taking Naron® again. Shortly after she was admitted to our hospital with mild metabolic acidosis and mild acute pancreatitis again, and, at that time, conservative therapy was effective. A similar episode occurred again in April 2007, soon after abusing Naron® again. Following her self-rechallenge test with the same acetaminophen drug, this case could be diagnosed as drug-induced acute pancreatitis with metabolic acidosis.
Figure 1. a. Abdominal CT on her first admission. b. Abdominal CT
on sixth day of hospitalization. c. Abdominal CT two months after
the first admission.
DISCUSSION
A national survey carried out in Japan in 1999 reported that 1.2% of all cases of acute pancreatitis were drug-induced [9]. Drug-induced acute pancreatitis is rare but should not be overlooked in a patient who presents with idiopathic acute pancreatitis [1]. Certain subpopulations such as children, women, the elderly and patients with advanced HIV infection or inflammatory bowel disease may be at higher risk [2]. Drug-induced acute pancreatitis is often challenging for clinicians for the following reasons [1, 2]: 1) the list of drugs associated with acute pancreatitis has increased, but many case reports suffer from a combination of inadequate criteria for reaching a diagnosis; 2) drug-induced pancreatitis is rarely accompanied by clinical or laboratory evidence of a drug reaction, such as rash, lymphadenopathy, and/or eosinophilia and 3) although a positive re-challenge with a drug is the best evidence available for cause and effect, it is not proof [1].
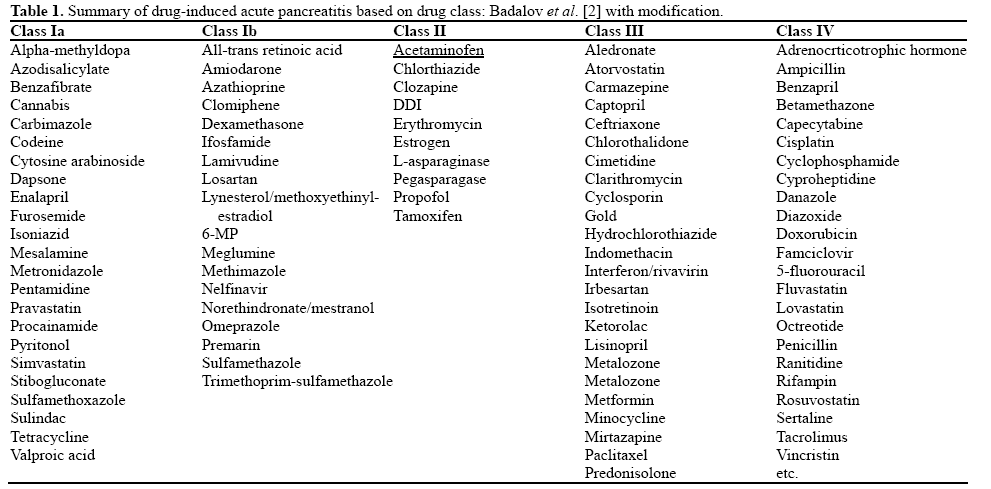
In previous years, experts created a classification system that addresses the likelihood which certain drugs would be associated with acute pancreatitis, using categories of definite, probable and questionable/possible [1, 2]. Most recently, Badalov et al. expanded the classification system into five categories [1]. Class Ia includes drugs with at least one case report, evidence of a positive rechallenge, and exclusion of other causes of acute pancreatitis. Class Ib drugs have at least one published case showing a rechallenge, but the case failed to rule out other common causes of acute pancreatitis. Acetaminophen is classified as a Class II drug and includes at least four case reports with a consistent latency period for at least 75% of the cases (Table 1). Class III drugs have at least two case reports but do not have rechallenge data or a consistent latency period. Class IV drugs have one case report without rechallenge data [1].
The mechanism of drug-induced pancreatitis is unknown. In general, some potential mechanisms include pancreatic duct obstruction, cytotoxic and metabolic effects, accumulation of a toxic metabolite or intermediary, and hypersensitivity reactions [1, 2]. Acetaminophen has been associated with acute pancreatitis in cases where there has been an overdose of drugs containing acetaminophen; however, its frequency is rare [3, 4, 5, 6, 7]. Schmidt and Dalhoff [3] reported that paracetamol (analgesic drug containing acetaminophen) poisoning has primarily been associated with hepatotoxicity including fulminant hepatic failure. They also showed that hyperamylasemia was frequent in patients with paracetamol poisoning whereas clinical acute pancreatitis rarely occurs [3]. Eight hundred and fourteen patients with paracetamol poisoning were analyzed and only thirty-three patients were diagnosed with paracetamol-associated acute pancreatitis [3]. Considering the number of cases of acetaminophen overdose and the rarity of pancreatitis in this setting, it is much more likely that an idiosyncratic reaction plays a role rather than intrinsic drug toxicity [1, 3, 4, 5, 6, 7]. Idiosyncratic reactions can be divided further into those secondary to hypersensitivity reactions and those caused by the accumulation of a toxic metabolite or some intermediary injurious substance [1]. The range of previously reported acetaminophen overdoses is 9.75 to 50 g, but, in this case, the patient had taken approximately 5 g of acetaminophen per day. In the case of this patient, the buildup was small and a daily overdose may result in the accumulation of acetaminophen. Acetaminophen overdose is also known to cause metabolic acidosis, at least in one case, which was also independent of hepatic failure or its complications [10]. However, detailed mechanisms remained unclear. In this case, the patient experienced a similar situation three times each after an overdose of acetaminophen; demonstrating acute pancreatitis, diagnosed by abdominal pain, elevated serum amylase level and CT findings, and complicated by metabolic acidosis. Severe acute pancreatitis often complicates metabolic acidosis and the systemic inflammatory response syndrome. In this case, the extent of the pancreatitis could be thought of as relatively mild according to the CT findings; therefore, it may be appropriate to diagnose this case as drug-induced acute pancreatitis complicated by drug-induced metabolic acidosis.
Once the acetaminophen overdose is diagnosed, N-acetylcysteine treatment is usually given to the patient [3, 7, 10]. In this case, information regarding the patient’s medical history was not immediately available which led to our extensive testing. There is one case report using continuous arteriovenous hemofiltration for the treatment of metabolic acidosis induced by acetaminophen overdose [10], and continuous hemodiafiltration might be effective in this case.
In conclusion, we have described a rare case of acetaminophen-induced pancreatitis. It is very important to rule out drug-induced pancreatitis when treating pancreatitis having an unknown etiology.
Conflict of interest The authors have no potential conflicts of interest
References
- Badalov N, Baradarian R, Kadirawel I, Iswara K, Li J, Steinberg W, et al. Drug-induced acute pancreatitis: an evidence-based review. ClinGastroenterolHepatol. 2007; 5: 648-61. [PMID 17395548]
- Balani AR, Grendell JH. Drug-induced pancreatitis: incidence, management and prevention. Drug Saf. 2008; 31: 823-37. [PMID 18759507]
- Schmidt LE, Dalhoff K. Hyperamylasemia and acute pancreatitis in paracetamol poisoning. Aliment PharmacolTher. 2004; 20:173-9. [PMID 15233697]
- Mofenson HC, Caraccio TR, Nawaz H, StecklerG.. Acetaminophen induced pancreatitis. J ToxicolClinToxicol. 1991; 29: 223-30. [PMID 1675695]
- Gilmore IT, Tourvas E. Paracetamol-induced acute pancreatitis. Br Med J. 1977; 1: 753-4. [PMID 851712]
- Coward RA. Paracetamol-induced acute pancreatitis. Br Med J. 1977; 1: 1086. [PMID 858062]
- Caldarola V, Hasset JM, Hall AH, Bronstein AB, Kuliq KW, Rumack BH. Hemorrhagic pancreatitis associated with acetaminophen overdose. Am J Gastroenrerol. 1986; 81: 579-82. [PMID 3717123]
- Ogawa M, Hirota M, Hayakawa T, Matsuno S, Watanabe S, Atomi Y, et al. Development and use of a new staging system for severe acute pancreatitis based on a nationwide survey in Japan. Pancreas 2002; 25: 325-30. [PMID 12409824]
- Sekimoto M, Takada T, Kawarada Y, Hirata K, Mayumi T, Yoshida M, et al; JPN. JPN guidelines for the management of acute pancreatitis: epidemiology, etiology, natural history, and outcome predictors in acute pancreatitis. J HepatobiliaryPancreat Surg. 2006; 13: 10-24. [PMID 16463207]
- Ala A, Schiano T, Burroughs A, Keshav S. Recognition of nonhepatic coma in the setting of acetaminophen overdose. Dig Dis Sci. 2004; 49: 1977-80. [PMID 15628737]


