Keywords
Pancreatic Neoplasms; Quality of Life
INTRODUCTION
Pancreatic adenocarcinoma is worldwide the forth most common cause of cancer-related death [1]. Nowadays, it remains one of the most challenging malignant diseases in many ways. About 80-90% of patients are already locally and systemically advanced at the time of diagnosis with median survival of 3-4 months without treatment. Even with some improvements in treatment in the last 40 years, however, there has been an insignificant increase from 2% to 5-6% in 5-year survival rates. Surgical resection remains the only option for possibly curative treatment but only 5%-22% are amenable to surgery at presentation, still the 5-year survival remains less than 30% [1-3]. The standard treatment of advanced cases includes chemotherapy or chemoradiation. The benefits in terms of improving survival (only a marginal survival benefit of 2–3 months reported) and providing palliative care (toxicity leading to side effects and complications) remain controversial and require good patient selection [1].
Pancreatic cancer (PC) patients present with systemic and gastrointestinal symptoms severely impairing their quality of life (QoL) [3]. Abdominal pain is probably the most common and distressing symptom along with weight loss and fatigue, causing anxiety and depression in most of the patients. In the course of the disease, biliary and intestinal obstruction or pancreatic insufficiency with diarrhea and vomiting complete the clinical presentation. Pain relief with opioids is often inadequate, has temporary results and many side effects. According to literature, nerve block procedures and thoracoscopic splanchnicectomy can lead to significant but very limited reduction of pain and do not improve either quality of life or survival so their value is questionable and their used as additives to opioids is advised [4,5].
Apart from the cancer itself, different interventions during treatment also affect patients’ QoL in terms of general condition, physical, emotional and social functioning. This is why considering patients’ personal needs and durability is important. For this reason, information about the health-related quality of life (HQOL) must be taken into account apart from the routinely used objective data such as survival, remission and recurrence time, complications, respond to treatment, tumor markers etc. [3,6,7].
In inoperable advanced PC cases, providing local disease control, better survival and symptom relief can be achieved by physical destruction of the tumor with different ablation techniques. Such ablative therapies are high-intensity focused ultrasound (HIFU), radiofrequency ablation (RFA), irreversible electroporation (IRE), iodine-125, iodine-125–cryosurgery, photodynamic therapy (PDT) and microwave ablation [8].
AIM
The aim of our review was to search through the literature if the quality of life of patients with advanced pancreatic cancer was investigated after different ablation techniques.
METHODOLOGY
A non-systematic literature search was performed through the PubMed, Scopus, EMBASE databases and the Cochrane Library to identify studies published before 1st April 2015, related to quality of life after ablative techniques, introduced in PC treatment. The search also included relevant information in the literature about validated instruments for evaluation of the quality of life. The ablation techniques included in the search were high-intensity focused ultrasound (HIFU), radiofrequency ablation (RFA), irreversible electroporation (IRE), photodynamic therapy (PDT), cryoablation, and microwave. Only materials in English describing ablation in unresectable PC were selected. Review articles, original manuscripts, abstracts and clinical guidelines were included. References were also screened for any relevant studies.
Quality of Life Evaluation
For an aggressive disease such as PC, the treatment must not only be clinically effective, but must cause as little harm as possible [6,10]. This is why using patients’ selfassessment and QoL evaluation as an additional criterion for patient stratification and treatment choice should be well developed. Many studies have already provided satisfactory results about baseline and treatment QoL as a prognostic factor both for survival and respond to therapy [6,11-13]. As important as QoL is, the instruments used to evaluate it must be relevant and feasible. They range from visual analogue scales to generic and diseasespecific questionnaires.
The pain response is usually measured by a numeric rating scale (0-10). Performance status in oncology is a measure for patients’ general condition or well-being and daily routine, used to determine the curative or palliative treatment necessary. In some trials it is used to try to evaluate the quality of life. The Karnofsky performance status (KPS) score is often used for evaluation of the oncology patient’s health status. In the Karnofsky score 100 is "perfect" health and 0 means death [14]. The Eastern Cooperative Oncology Group (ECOG) score is similar to the Karnofsky scale but ranges from 0 to 5 (here 0 stands for “perfect” health; 5–for “death”) [15]. The Edmonton Symptom Assessment System (ESAS) is another simple method for the assessment of palliative care patients [16].
Different instruments for QoL assessment are the Functional Assessment of Cancer Therapy (FACT) questionnaires (FACT-G and FACT-Hep) as well as the ones validated by the European Organization of Research and Treatment of Cancer (EORTC QLQ-C30 and QLQ Pan26) [13,17,18]. Other questionnaires are under investigation - the NIH PROMIS, the pancreatic cancer disease impact (PACADI) score and Gastrointestinal Symptom Rating Scale (GSRS) - a validated questionnaire to assess GI symptoms [19].
High-Intensity Focused Ultrasound (HIFU)
HIFU is a new therapeutic for the treatment of locally advanced, unresectable and systemically advanced, metastatic PC patients with no surgical excision and no blood-loss during procedure. An extracorporeal device is used to focus high-intensity ultrasound beam into a target zone of the tumor and causes local destruction with high level of precision, preserving the surrounding tissues. HIFU causes a rapid local rise in temperature over 70 degrees which leads to coagulative necrosis. HIFU also induces apoptosis at a lower dose of hyperthermia than necrosis [20,21]. Most of the complications of HIFU reported in literature are minor and could be avoided by careful preoperative patient selection and preparation, HIFU parameter calculation and target localization as well as intraoperative monitoring [22]. Complications observed include superficial skin burns or edema, fever, insignificant gastrointestinal dysfunction and mild abdominal pain in the treated area, duodeno-pancreatic fistulas, asymptomatic vertebral body or subcutaneous fat necrosis with no need for further treatment. A major concern about HIFU is pancreatitis, caused by the physical destruction of cells [20-22]. Up to present, no deformation or occlusion after HIFU treatment is reported. Only one patient had portal vein thrombosis after HIFU [23]. Large studies in China and smaller researches in Europe have confirmed HIFU as a safe and feasible treatment option for advanced PC patients [22-31].
Significant pain relief, increased KPS, prolonged survival and restricted tumor growth are reported in almost all studies [22-33]. The median survival reported is 8-11 months in stage III and 5-6 mo in stage IV patients. All researchers report pain relief after HIFU treatment in about 80%- 100% of patients [22-32]. A study showed that the average pain scores (according to VAS) on the day before treatment was 5.80±2.14, and those at 7th day after HIFU were 2.45±2.4 [32]. A significant correlation is reported between HIFU treatment and the average quantity of morphine needs. A study reported decrease of 16.8±39.7 mg for each person every day [32]. Also, common symptoms such as fatigue and loss of appetite were improved after HIFU exposure, increasing the QoL.
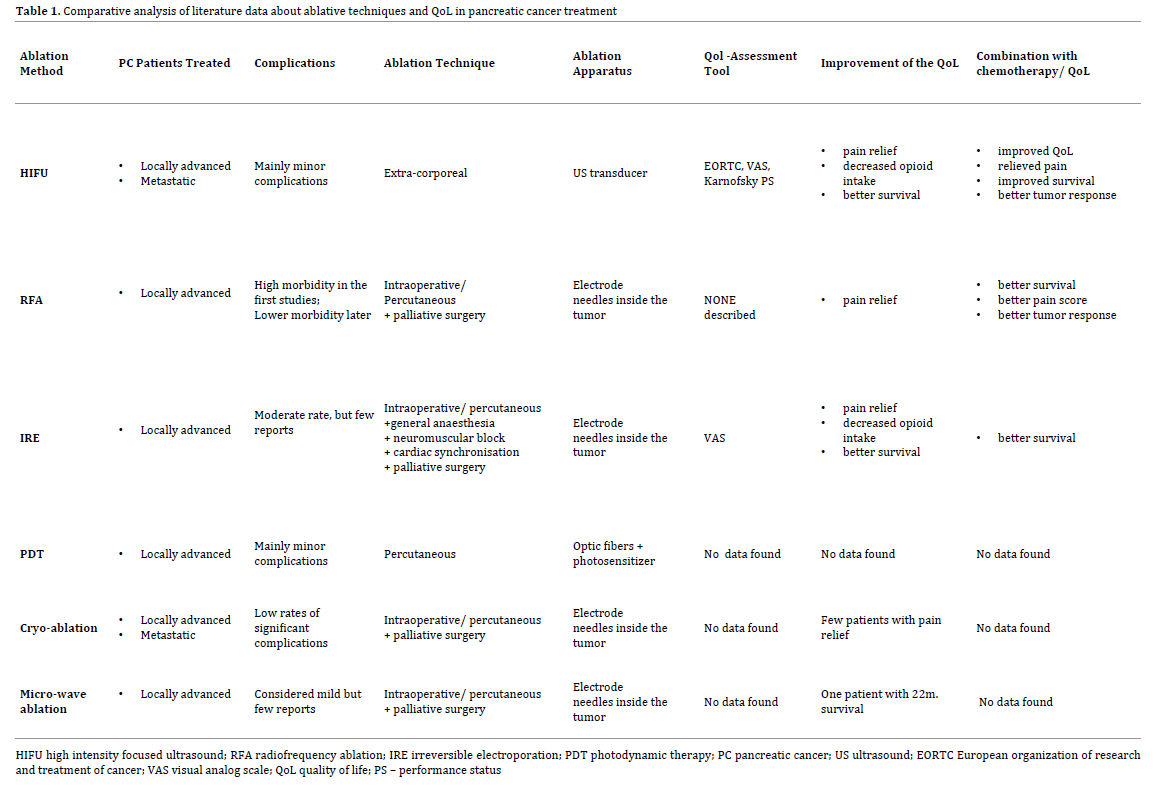
According to literature, a combination multimodality treatment with HIFU, chemotherapeutics, chemoradiation and immunotherapeutics could have better therapeutic outcomes such as higher level of pain relief and longer survival [33-35]. A recent study on combination treatment of gemcitabine with HIFU in locally advanced PC showed that overall survival was 12.6 mo and the estimates of overall survival at 12 and 24 months were 50.6% and 17.1% respectively. Pain was relieved in 78.6% [34]. Dimitrov et al reported pain relief from 7 to 2 out of 10 according to VAS in a patient after HIFU; combined with neoadjuvant and adjuvant chemotherapy. The authors introduced the EORTC instruments for evaluation of the QoL of PC patients. In their case report QoL assessed with the validated instruments was improved significantly. The patient survival after HIFU at the time of case report was 24 months [33]. The literature data about HIFU treatment was presented concisely in Table 1.
There are already clinical studies reporting enhanced antitumor immunity after HIFU. The immune response can be stimulated by large amount of tumor antigens in the necrotic tissue, protein Ag determinants and heat shock protein activation by hyperthermia, local aseptic inflammation due to necrosis [36,37].
Radiofrequency Ablation (RFA)
RFA is an ablative method for local radiofrequencyinduced thermal coagulation of solid tumors under ultrasound (US) guidance during open surgery by needles with expandable electrodes, placed in the tumor. RFA has been used successfully for hepatic tumors. Recent studies have come with tentative results for unresectable locally advanced, non-metastatic PC ablation [8,9,38-40]. However, the number of patients treated with RFA was small in most reports.
RFA for PC was combined with palliative bypass surgery and drainage in most studies [38-41,45]. The local temperature reached up to 105 degrees as in the liver tumor ablation. The early applications of RFA in the pancreas were associated with very high rates of morbidity related to RFA (4-37%), overall morbidity (10%-40%) and mortality (0%-25%) [38-40]. Median survival after RFA was 3-33 months, in most studies around 16 months [38-41]. Frequent complications were fluid collection, pancreatic fistula, duodenal perforation and vascular damage, digestive or abdominal bleeding, infections or abscesses [38-42]. Severe acute pancreatitis was a rare complication. In a study with 20 cases, two patients died from severe complications - septic shock and gastrointestinal bleeding [42]. In later RFA applications the temperature goal was decreased to < 90 °C at the RFA probe tip and sufficient distances between the probe and surrounding structures as well as local cooling was ensured [43,44]. While some studies reported a significant decrease in morbidity, others still had some tentative results.
In all studies RFA led to tumour necrosis and tumor cytoreduction [38-44]. Authors observed promising results in pain relief (in 50% of cases in one study, and in 68% according to another) and decreased analgesia requirements [38-43].
Some studies came out with survival of those who received chemotherapy after RFA reaching 25.6 months. These results are suggestive of better outcomes of combined local control and systemic treatment but further research is needed [53]. RFA combined with 125iodine seed implantation for unresectable pancreatic tumors was reported as a feasible and safe option with better tumor responses, significantly decreased tumor marker levels and pain score. In this study , the median survival time of 32 patients was 17.5 months, and 20months for the group receiving chemotherapy against 16months for the group with no chemotherapy [54]. Some authors suggested RFA as an alternative to the conventional phenol and alcohol neurolytic splanchnic nerve block methods thanks to the well-known neuroanatomy and accurate needle placement [55]. There was no QoL instrument implemented in the RFA studies (Table 1).
Irreversible Electroporation (IRE)
Irreversible electroporation (IRE) is a non-thermal ablation technique using short electrical pulses between needles around the tumor, placed after laparotomy or through the skin under US guidance [56]. It is performed under general anesthesia with neuromuscular blockage to avoid muscle contractions. IRE has been performed in locally advanced, surgically unresectable, non-metastatic cases. One of the main concerns and now a patient exclusion criterion is a metal stent in the bile duct. A case report described severe complications including bowel perforation and bleeding from a branch of the superior mesenteric artery leading to death after IRE in the head of the pancreas close to a metal stent [57]. A review of 4 studies with 74 patients in total reported morbidity from 0 to 33% and significant survival benefit: overall survival in matched IRE group - 20months, and non-IRE group - 11 months. A moderate rate of complications from IRE is reported up to present but the studies are still few with a small number of patients [8,9,56]. A study of 27 patients (with IRE; IRE+ resection; IRE+ palliative surgery) demonstrated 90 days after treatment some palliation of pain, assessed by VAS (pain score from 5 to 3) and reduction of narcotic use (from median 75 mcg to 25 mcg fentanyl per day) [57]. There is still no specific data about quality of life, affected by IRE (Table 1).
Microwave Ablation
Microwave ablation is a local thermal ablative method, used safely in liver tumors. Studies for its use in locally advanced, non-metastatic PC cases are few. It is based on microwave currents from antennae percutaneously or most often intraoperatively inserted into the tumour during palliative bypass surgery under imaging guidance [8,9,58,59]. The largest study up to present included 15 patients and there were minor complications were reported in 40%, namely asymptomatic pancreatitis, ascites and minor bleeding. One patient had a survival of 22 months [59]. Quality of life, including pain relief was not assessed with a validated tool (Table 1).
Cryoablation
Cryoablation is a technique for argon-gas-based freezing of unresectable pancreatic lesions to -160 °C by probes placed in the pancreas intra-operatively or percutaneously under US guidance. Safety margins and simultaneous palliative bypass procedures are brought to attention here too. Studies report prolonged survival with low rates of significant complications [8,9,61-63] A study revealed median overall survival in a combined cryoimmunotherapy group of 13months compared to chemotherapy group - 3.5 months [64]. Pain control is assessed in few patients with some positive results for alleviating the pain symptoms [62,63]. The effects on QoL have not been described yet (Table 1).
Photodynamic Therapy (PDT)
Photodynamic therapy causes predictable destruction of tumor cells, photosensitized with special substances and exposed to light from optic fibers, placed percutaneously under image guidance. A study of 16 patients reported median survival of 9.5 months. In two cases bleeding from the gastrointestinal tract was observed. Photosensitivity and danger of skin necrosis was a major concern in the first clinical trials, nowadays successfully avoided by new generations of photosensitizers [8,9,65,66].
DISCUSSION
Based on the review data, we can outline several problems. Firstly, there is no standardized method for dynamically evaluating the QoL of PC patients, treated with ablative techniques. The development of a method improving the QoL would lead to a positive change in the really grim statistics for this type of cancer, so establishing a trustworthy instrument for evaluation is important. Another problem which was also a major discussion topic during the American Society of Clinical Oncology (ASCO) annual meeting 2013 was whether quantity or quality of life must be the treatment goal in patients with advanced PC. It was underlined that clinical response to chemotherapy does not automatically correlate with improved QoL of patients. Also poor quality of life is associated with a low response to chemotherapy [6]. The literature review shows that technological progress is now capable of successfully combining chemotherapy with local ablation of the tumor in the pancreas. The combination of physical destruction with chemotherapy could not only lead to prolonged survival but also to improved QoL. This beneficial effect may be associated with decreased pain, reduced dose of morphine derivatives, increased total immunity and some antibodies, etc. Last, but not least it is a discouraging fact for patients to know that they are left on palliative chemotherapy without a real opportunity for treatment. Considering the up-to-date studies, it can be concluded that for an ablative method to achieve its goal to increase QoL, it should cause possibly the most minimal trauma and/or to be non-invasive; have minimal complications; should lead to pain relief after treatment; achieve tumor necrosis; provide accuracy and precision as well as image-guided control. It should be borne in mind that most ablation techniques have restrictions in the treatment indications and cannot be used in all cases with advanced PC. Most authors carry out a serious patient selection for successful implementation of the techniques into the clinical practice [8,9,20,27,38,39,56]. Ablative therapies in patients with advanced pancreatic cancer seem to be feasible and safe [8,9]. Quality of life assessment is still a secondary goal in most researches.
CONCLUSION
None of the ablative techniques is a standardized method for pancreatic malignancies yet, but studies have proved them safe and feasible with different rates of complications. Survival outcomes as well as benefits for quality of life need further investigation. There is not yet a standardized method for QoL evaluation in ablative treatment. Multimodality treatment with chemotherapy and ablation methods seems to have better outcomes in advanced PC cases.
Conflict of interest
Authors have no conflicts of interest
References
- Hsueh CT. Pancreatic cancer: current standards, research updates and future directions. GastrointestOncol 2011; 2:123-125. [PMID: 22811841]
- Singh SM, Longmire WP Jr, Reber HA. Surgical palliation for pancreatic cancer. The UCLA experience. Ann Surg 1990; 212:132-139. [PMID: 1695834]
- Labori KJ, Hjermstad MJ, Wester T, Buanes T, Loge JH. Symptom profiles and palliative care in advanced pancreatic cancer - a prospective study. Support Care Cancer 2006; 14:1126-1133. [PMID: 16601947 ]
- Seufferlein T, BachetJB E Van Cutsem, Rougier P. Pancreatic adenocarcinoma: ESMO-ESDO ClinicalPractice Guidelines for diagnosis, treatment andfollow-up. Annals of Oncology 2012;23 Suppl. 7: vii33-vii40. [PMID: 22997452]
- Johnson CD. An open randomized comparison of clinical effectiveness of protocol-driven opioid analgesia, celiac plexus block or thoracoscopicsplanchnicectomy for pain management in patients with pancreatic and other abdominal malignancies. Pancreatology2009; 9:755-763. [PMID: 20090396]
- Shahrokni A, Saif MW. Metastatic Pancreatic Cancer:The Dilemma of Quality vs. Quantity of Life. JOP. J Pancreas 2013; 14:391-394. [PMID: 23846935]
- Lee V, Haiying C, Li G, Saif MW. Quality of Life in Patients with Pancreatic Cancer. JOP J Pancreas 2012; 13:182-184. [PMID: 22406597]
- Keane MG, Bramis K, Pereira SP, Fusai GK. Systematic review of novel ablative methods in locally advanced pancreatic cancer. World J Gastroenterol 2014; 20: 2267-2278. [PMID: 24605026]
- Rombouts SJ. Systematic review of innovative ablative therapies for the treatment of locally advanced pancreatic cance. British Journal of Surgery 2015;102: 182-193. [PMID: 25524417]
- Crippa S, Domínguez I, Rodríguez JR, Razo O. Quality of Life in Pancreatic Cancer: Analysis by Stage andTreatment. Gastrointest Surg 2008; 12: 783-794. [PMID: 18317851]
- Anwar S, Tan W, Yu J, Hutson A, Javle M, Iyer R. Quality-of-life (QoL) as a predictive biomarker in patients with advanced pancreatic cancer (APC) receiving chemotherapy: results from a prospective multicenter phase 2 trial. J GastrointestOncol 2014; 5:433-439. [PMID: 25436122]
- Quinten C. Coens C, Mauer M, Comte S, Sprangers MA, Cleeland C, Osoba D, et al. Baseline quality of life as a prognostic indicator of survival: a meta-analysis of individual patient data from EORTC clinical trials. The lancet oncology 2009; 10:865-871. [PMID: 19695956]
- Gupta, Digant LIS, Christopher G, Grutsch, James F. The European organization for research and treatment of cancer quality of life questionnaire: implications for prognosis in pancreatic cancer. International journal of gastrointestinal cancer 2006; 37: 65-73. [PMID: 17827524]
- Karnofsky, David A. The clinical evaluation of chemotherapeutic agents in cancer. Evaluation of chemotherapeutic agents 1949.
- Oken MM, Creech RH, Tormey DC.Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982;5: 649-55. [PMID: 7165009]
- Bruera E, Kuehn N, Miller MJ, Selmser P, Macmillan K. The Edmonton Symptom Assessment System (ESAS): a simple method for the assessment of palliative care patients. J Palliat Care 1991;7:6-9. [PMID: 1714502]
- EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 1990; 16: 199-208. [PMID: 10109801]
- Fitzsimmons D, Johnson CD. Development of a disease specific quality of life (QoL) questionnaire module to supplement the EORTC core cancer QoL questionnaire, the QLQC30 in patients with pancreatic cancer. EORTC Study Group on Quality of Life. Eur J Cancer 1999; 35: 939-941. [PMID: 10533475]
- HeibergT, Nordby T, Kvien TK, BuanesT. Development and preliminary validation of the pancreaticcancer disease impact score. Support Care Cancer2013;21:1677-1684. [PMID: 23314652]
- Wu F. High intensity focused ultrasound: A noninvasive therapy for locally advanced pancreatic cancer. World J Gastroenterol 2014; 20: 16480-16488. [PMID: 25469016]
- Khokhlova TD, Hwang JH. HIFU for palliative treatment of pancreatic cancer.Journal of gastrointestinal oncology2011;2: 175. [PMID: 22811848]
- JungSE,choSH,jang JH. High-intensity focused ultrasound ablation in hepatic and pancreatic cancer: complications.Abdominal imaging2011;36: 185-195. [PMID: 20512587]
- Orsi F, Zhang L, Arnone P. High-intensity focused ultrasound ablation: effective and safe therapy for solid tumors in difficult locations. AJR Am J Roentgenol 2010; 195: W245-W252 . [PMID: 20729423]
- Wu Y,Li J,zhang SJ. Observation of high intensity focused ultrasound treating 40 cases of cancer of pancreas. Chin J Clin Hep 2003; 19: 145-146. [PMID: 23157899]
- Wu F, Wang ZB, Zhu H, Chen WZ, Zou JZ, Bai J, et al. Feasibility of US-guided high-intensity focused ultrasound treatment in patients with advanced pancreatic cancer: initial experience. Radiology 2005; 236: 1034-1040. [PMID: 16055692]
- Xiong LL, Hwang JH, Huang XB, Yao SS, He CJ, Ge XH, et al. Early clinical experience using high intensity focused ultrasound for palliation of inoperable pancreatic cancer. JOP 2009; 10: 123-129. [PMID: 19287104]
- Zhang L, Wang ZB. High-intensity focused ultrasound tumor ablation: Review of ten years of clinical experience. Front Med China 2010; 4: 294-302. [PMID: 21191835]
- Wang K, Chen Z, Meng Z, Lin J, Zhou Z, Wang P, et al. Analgesic effect of high intensity focused ultrasound therapy for unresectable pancreatic cancer. Int J Hyperthermia 2011; 27: 101-107. [PMID: 21191835]
- Sung HY, Jung SE, Cho SH. Long-Term Outcome of High-Intensity Focused Ultrasound in Advanced Pancreatic Cancer. Pancreas 2011; 40: 1080-1086. [PMID: 21926543]
- Li PZ, Zhu SH, He W, Zhu LY, Liu SP, Liu Y, et al. High-intensity focused ultrasound treatment for patients with unresectable pancreatic cancer. HepatobiliaryPancreat Dis Int 2012; 11: 655-660. [PMID: 23232639]
- Wang K, Zhu H, Meng Z, Chen Z, Lin J, Shen Y, et al. Safety evaluation of high-intensity focused ultrasound in patients with pancreatic cancer. Onkologie 2013; 36: 88-92. [PMID: 23485995]
- Tan X, Chen J. Analgesic effect of high-intensity focused ultrasound in patiens with advanced pancreatic cancer. Chinese-German J ClinOncol 2013; 8: 385-388. [PMID: 21219135]
- Dimitrov D, Andreev T, Feradova H, Ignatov B. Multimodality Treatment by FOLFOX plus HIFU in a Case of Advanced Pancreatic Carcinoma. A Case Report. JOP J Pancreas (Online) 2015; 16:66-69. [PMID: 25640787]
- Zhao H, Yang G, Wang D, Yu X, Zhang Y, Zhu J, et al. Concurrent gemcitabine and high-intensity focused ultrasound therapy in patients with locally advanced pancreatic cancer. Anticancer Drugs 2010; 21: 447-452. [PMID: 20075714]
- Lee JY, Choi BI, Ryu JK, Kim YT, Hwang JH. Concurrent chemotherapy and pulsed high-intensity focused ultrasound therapy for the treatment of unresectable pancreatic cancer: initial experiences. Korean J Radiol 2011; 12: 176-186. [PMID: 21430934]
- Wu F, Zhou L, Chen WR. Host antitumor immune responses to HIFU ablation. Int J Hyperthermia 2007; 23: 165-171. [PMID: 22633269]
- Wu F, Wang ZB, Lu P, Xu ZL, Chen WZ, Zhu H, et al. Activated anti-tumor immunity in cancer patients after high intensity focused ultrasound ablation. Ultrasound Med Biol 2004; 30:1217-1222. [PMID: 15550325]
- D'Onofrio M, Barbi E, Girelli R, Martone E, Gallotti A, Salvia R, et al. Activated anti-tumor immunity in cancer patients after high intensity focused ultrasound ablation. World J Gastroenterol 2010; 16: 3478-3483. [PMID: 15550325]
- Fegrachi S, Besselink MG. Radiofrequency ablation for unresectable locally advanced pancreatic cancer: a systematic review. HPB 2014; 16: 119-123. [PMID: 23600801]
- Pezzilli R, Raffaele. The problems of radiofrequency ablation as an approach for advanced unresectable ductal pancreatic carcinoma. Cancers 2010; 2: 1419-1431. [PMID: 24281165]
- Pandya GJ. Radiofrequency ablation of pancreatic ductal adenocarcinoma-the past, the present and future. World J GastrointestOncol 2015; 7: 6-11. [PMID: 25685272]
- Wu Y, Yulian. High operative risk of cool-tip radiofrequency ablation for unresectable pancreatic head cancer. Journal of surgical oncology 2006; 94: 392-395. [PMID: 16967436]
- Matsui Y, Yoichi. Selective thermocoagulation of unresectable pancreatic cancers by using radiofrequency capacitive heating. Pancreas 2000; 20: 14-20. [PMID: 10630378]
- Girelli R, Frigerio I, Salvia R, Barbi E, Tinazzi Martini P, Bassi C. Feasibility and safety of radiofrequency ablation for locally advanced pancreatic cancer. British Journal of Surgery 2010; 97: 220-225. [PMID: 20069610]
- Girelli R. Survival after radiofrequency of stage III pancreatic carcinoma abstracts. HPB : The Official Journal of the International HepatoPancreato Biliary Association 2011; 13(Suppl 2): 15.
- Spiliotis JD, Datsis AC, Michalopoulos NV, Kekelos SP, Vaxevanidou A, Rogdakis AG, et al. Radiofrequency ablation combined with palliative surgery may prolong survival of patients with advanced cancer of the pancreas. Langenbeck's Archives of Surgery 2007; 392: 55-60. [PMID: 17089173]
- Elias D, Baton O, Sideris L, Lasser P, Pocard M. Necrotizing pancreatitis after radiofrequency destruction of pancreatic tumours. European Journal of Surgical Oncology (EJSO) 2004; 30: 85-87. [PMID: 14736529]
- Hadjicostas S, Malakounides N, Varianos C, Kitiris E, Lerni F, Symeonides P. Radiofrequency ablation in pancreatic cancer. HPB 2006; 8.1: 61-64. [PMID: 18333241]
- Varshney S. Radiofrequency ablation of unresectable pancreatic carcinoma: feasibility, efficacy and safety. JOP 2006; 7: 74-78. [PMID: 16407624]
- Siriwardena, Ajith KAK. Radiofrequency ablation for locally advanced cancer of the pancreas. JOP 2006; 7:1-4. [PMID: 16407612]
- Tang Z, Wu YL, Fang HQ, Xu J, Mo GQ, Chen XM, et al. Treatment of unresectable pancreatic carcinoma by radiofrequency ablation with 'cool-tip needle': report of 18 cases. Zhonghuayixuezazhi 2008; 88: 391-394. [PMID: 18581892]
- Pai. PWE-055 Endoscopic Ultrasound Guided Radiofrequency Ablation (EUS-RFA) for Pancreatic Ductal Adenocarcinoma. Gut 2013; 62: A153-A153.
- Giardino A, Girelli R, Frigerio I, Regi P, Cantore M, Alessandra A, et al. Triple approach strategy for patients with locally advanced pancreatic carcinoma. HPB 2013; 15: 623-627. [PMID: 23458679]
- Zou YP, Li WM, Zheng F, Li FC, Huang H, Du JD, Liu HR. Intraoperative radiofrequency ablation combined with 125 iodine seed implantation for unresectable pancreatic cancer. World journal of gastroenterology: WJG 2010;16: 5104-10. [PMID: 20976848]
- Garcea G, Thomasset S, Berry DP, Tordoff S. Percutaneous splanchnic nerve radiofrequency ablation for chronic abdominal pain. ANZ journal of surgery 2005; 75: 640-644. [PMID: 16076323]
- Moir J. Systematic review of irreversible electroporation in the treatment of advanced pancreatic cancer. European Journal of Surgical Oncology (EJSO) 2014; 40: 1598-1604. [PMID: 25307210]
- Mansson C,Nilsson A, Karlson BM. Severe complications with irreversible electroporation of the pancreas in the presence of a metallic stent: a warning of a procedure that never should be performed. Actaradiologica short reports 2014; 3: 2047981614556409. [PMID: 25535573]
- Martin RC, McFarland K, Ellis S, Velanovich V. Irreversible electroporation therapy in the management of locally advanced pancreatic adenocarcinoma. J Am Coll Surg 2012; 215: 361-369. [PMID: 22726894]
- Carrafiello G, Ierardi AM, Fontana F, Petrillo M, Floridi C, et al. Microwave ablation of pancreatic head cancer: safety and efficacy. J Vasc Interv Radiol2013; 24: 1513-1520. [PMID: 24070507]
- Lygidakis NJ, Sharma SK, Papastratis P, Zivanovic V, Kefalourous H, et al. Microwave ablation in locally advanced pancreatic carcinoma-a new look. Hepato-gastroenterology 2006; 54: 1305-1310. [PMID: 17708242]
- Arcidiacono PG, Carrara S, Reni M, Petrone MC, Cappio S, Balzano G, et al. Feasibility and safety of EUS-guided cryothermal ablation in patients with locally advanced pancreatic cancer. Gastrointestinal endoscopy 2012; 76: 1142-1151. [PMID: 23021160]
- Kovach SJ, Hendrickson RJ, Cappadona CR, Schmidt CM, Groen K, Koniaris LG, et al. Cryoablation of unresectable pancreatic cancer. Surgery 2002; 131: 463-464. [PMID: 11935137]
- Niu L, Wang Y, Yao F, Wei C, Chen Y, Zhang L, et al. Alleviating visceral cancer pain in patients with pancreatic cancer using cryoablation and celiac plexus block. Cryobiology2013; 66.2: 105-111. [PMID: 23267876]
- Niu LZ, Li JL, Zeng JY, Mu F, Liao MT, Yao F, Li L, et al. Combination treatment with comprehensive cryoablation and immunotherapy in metastatic hepatocellular cancer. World journal of gastroenterology: WJG 2013; 19: 3473. [PMID: 23801841]
- Bown SG, Rogowska AZ, Whitelaw DE, Lees WR, Lovat LB, Ripley P, et al. Photodynamic therapy for cancer of the pancreas. Gut 2002; 50: 549-557. [PMID: 11889078]
- Huggett MT. Photodynamic therapy of locally advanced pancreatic cancer . In SPIE BiOS International Society for Optics and Photonics 2013; 85680J-85680J-6.

