Keywords
Severe Acute Pancreatitis, Infected Pancreatic Necrosis,
Step-up approach, Outcome, Videoscopic assisted retroperitoneal
debridement, Percutaneous Catheter Drainage
Abbreviations
CR complete resolution; IPN infected pancreatic
necrosis; PCD percutaneous catheter drainage; VARD videoscopic
assisted retroperitoneal debridement
INTRODUCTION
Acute pancreatitis (AP) results in an overall mortality
rate of 7.5% in Malaysia [1]. Moderately severe and severe
pancreatitis may result in the development of pancreatic
and or peripancreatic necrosis [2]. The pancreatic necrosis
may be sterile or infected. Patients may be relatively well
or may have persistent organ failure. INP in the absence of persistent organ failure results in mortality rates
ranging between 6-11% [3, 4]. Risk of mortality doubles
with persistant organ failure [5]. Unfortunately organ
failure persisting more than 48 hours is present in 50% of
patients with NP and approximately two thirds of patients
with INP. The crucial determining factor in management
should be whether the necrosis is sterile or infected, the
patient symptomatic or not, and the nature of the necrosis.
In general treatment should be aimed at patients who are
symptomatic and with suspected or proven infection. 2
types of necrotic collections are present, notably Acute
Necrotic Collections (ANC) and Walled-Off Necrosis (WON).
In general ANC require drainage while WON may require a
“step-up” to formal debridement. Intervention for NP can
be divided broadly into the following: 1. Catheter based
therapy 2. Endoscopic management 3. Combination of
both-dual modality and 4. Open surgical debridement [6].
Historically, open surgical debridement was considered
the goal standard and perhaps the only option of treatment
prior to the minimally invasive era of management. Although the landmark PANTER trial paved the way for a
more minimally invasive approach towards necrosectomy,
there are many studies performed which have questioned
the actual need for a formal necrosectomy. A systemic
review revealed that Percutaneous Catheter Drainage
(PCD) alone was able to obviate the need for further
therapy in 56.2% of patients [7, 8]. Successful outcome
depends on appropriate type and timing of intervention
[9, 10]. Extent of necrosis correlates with probability of
infection, organ failure, the need for intervention and
overall mortality and morbidity. The main aim of this study
was to evaluate the trends in management and outcomes
in patients undergoing intervention for infected NP in 2 of
the largest HPB centres in Malaysia and to analyse factors
predicting mortality in these patients. Our secondary
objective was to compare 2 of the commonest procedures
performed in these 2 institutions, PCD alone versus VARD.
METHODOLOGY
Study Design
This is a Cross sectional study of patients undergoing
intervention for Infected Pancreatic Necrosis in 2 of the
largest Hepatobiliary centres in Malaysia.
Data Collection
Data were collected from the institution written
admission records and progress notes, outpatient
clinic visit notes, operative database and the computer
information system database for all patients diagnosed
with NP between 2000 to 2018.
Participating Centres
Patients with necrotizing pancreatitis undergoing
intervention for Infected Pancreatic Necrosis between
January 2009 till December 2018 in Hospital Selayang
(HS), Selangor and Hospital Sultanah Bahiyah(HSB),Alor
Setar, Kedah were included.
Primary Objective
The main aim of this study was to evaluate the trends
in management and outcomes in patients undergoing
intervention for infected NP in 2 of the largest HPB centres
in Malaysia and to analyse factors predicting mortality in
these patients. The factors that were analyzed included the
following
Patient demography: Age, gender, race, presence
or absence of comorbidities (Hypertension, Diabetis
Mellitus, Ischaemic heart disease, Renal impairment,
COAD / Asthma, other premorbids), Aetiology (Biliary,
Alcohol, ERCP related, idiopathic, hypertriglyceridaemia),
admission to ICU, type of primary intervention employed
(no intervention, PCD alone, VARD, Endoscopic drainage
without necrosectomy, Open drainage/ resection),
presence or absence of gas on CT scan, nature of
necrosis whether ANC or WON, presence or absence
of asscociated pleural effusion, duration of symptoms
prior to admission, timing of primary intervention from
admission, total number of interventions performed, days of hospitalization, Balthazar CT severity index
score (CTSI) score, size of necrosis from cross sectional
CT scan, C-reactive protein and Albumin levels prior to
intervention.
Secondary objective: Using the variables above our
secondary objective was to compare the outcomes of the 2
main interventions VARD and PCD alone.
Inclusion criteria: All patients diagnosed with Infected
Pancreatic Necrosis between January 2009 till December
2018 in Hospital Selayang (HS), Selangor and Hospital
Sultanah Bahiyah (HSB), Alor Setar, Kedah were included.
Exclusion Criteria: Patients with incomplete data or
where outcome measures were not clearly stated were
excluded. Traumatic pancreatitis was also excluded.
Statistical Analysis: All statistical analyses were
performed using SPSS version 25.0 (SPSS Inc, Chicago, IL)
and SAS version 9.4. Descriptive analysis was performed
using Pearson Chi-squared test for categorical variables
and Fisher exact test when appropriate. Continuous
independent variables were analyzed using Mann-
Whitney U test. Univariable and multivariable analysis
were performed using binary logistic regression and
penalized logistic regression where appropriate. Using a
confidence interval of 95% a p value < 0.05 was considered
statistically significant.
RESULTS
A total number of 65 patients (35 patients from
Hospital Sultanah Bahiyah and 30 patients from Hospital
Selayang) were included in the study. From this total only
data from 61 patients were adequate for final analysis.
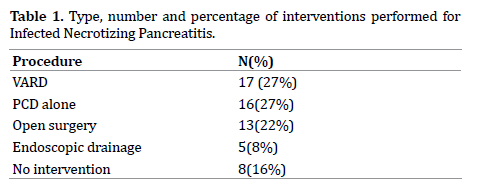
17 patients underwent Video Assisted Retroperitoneal
Debridement (VARD),16 Percutaneous Catheter Drainage
Alone (PCD alone), 13 patients underwent open surgery
(open debridement, open resection), 5 were subjected to
endoscopic drainage while 8 patients did not undergo any
formal procedure (Table 1).
Out of the 61 patients that were included, final analysis
were based on the outcomes of 59 patients (6 were lost to
follow up). Mortality rate was 25% (15/59 patients).
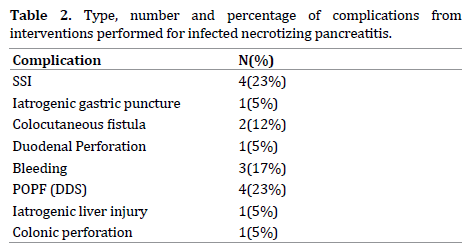
The following complications that developed included
surgical site infection, iatrogenic gastric injury during
percutaneous catheter drainage with ensuing peritonitis,
colocutaneous fistula, bleeding, duodenal perforation,
colonic perforation, post-operative pancreatic fistula
(POPF) with disrupted duct syndrome (DDF) and
iatrogenic liver injury (Table 2).
Positive cultures were obtained in 73% (43/59
patients). 16 patients had no growth from cultures taken.
The commonest isolate was E.Coli followed by ESBL
Klebsiella. Following are the different isolates obtained
along with percentages (Figure 1).
Figure 1 List and percentages of positive culture isolates from 1st drainage and procedures.
Patient Demography (age, race, gender)
26 male and 18 female patients had complete resolution
of necrosis. 11 male patients and 3 female patients died. (p
= 0.097). There was no difference in outcome across the 3
races (p = 0.875). The median age for patients with CR was
43.7 +/- 14.45 and 55.13 +/- 12.36 for those patients who
died (p=0.008).
Duration of Symptoms Prior to Admission, and
Associated Comorbidities
The median duration for patients in the CR group was
1 (1-4 days) while those within the D group was 1.5 (1-3)
days (p = 0.690). When comparing comorbidities between
the 2 groups, there was a statistical difference in patients who
had Renal Impairment (p = 0.006). 41 (93.2%) patients in the
CR group had no RI while 3 (6.8%) had RI in this group. In the
group who died 9 (60%) patients had no RI while 6 (40%)
had RI. No difference exist between the 2 groups in terms
of HPT (p = 0.058), IHD (p = 0.593), and COAD/Asthma (p =
0.564). Within the group of patients who died, 66.7% (10/15)
patients had DM compared with 36.4% (16/28) patients in
the group with CR (p = 0.041) (Table 3, 4).
Aetiology of Pancreatitis
Within the group of patients who had CR 26 patients (59.1%) had biliary aetiology while 3(6.8%), 2(4.5%),
12(27.3%) had alcohol, ERCP and idiopathic aetiology
respectively. Within the group of patients who died, 7
patients (46.7%) had biliary aetiology, 1 each (6.7%) were
alcohol and ERCP related, while 5 patients (33.3%) were
of idiopathic aetiology. There were 2 patients who had
hypertriglyceridaemia, 1 had complete resolution while
the other patient died. There was no statistical difference
between the 2 groups when comparing the different
aetiology (p = 0.774) (Table 5, 6).
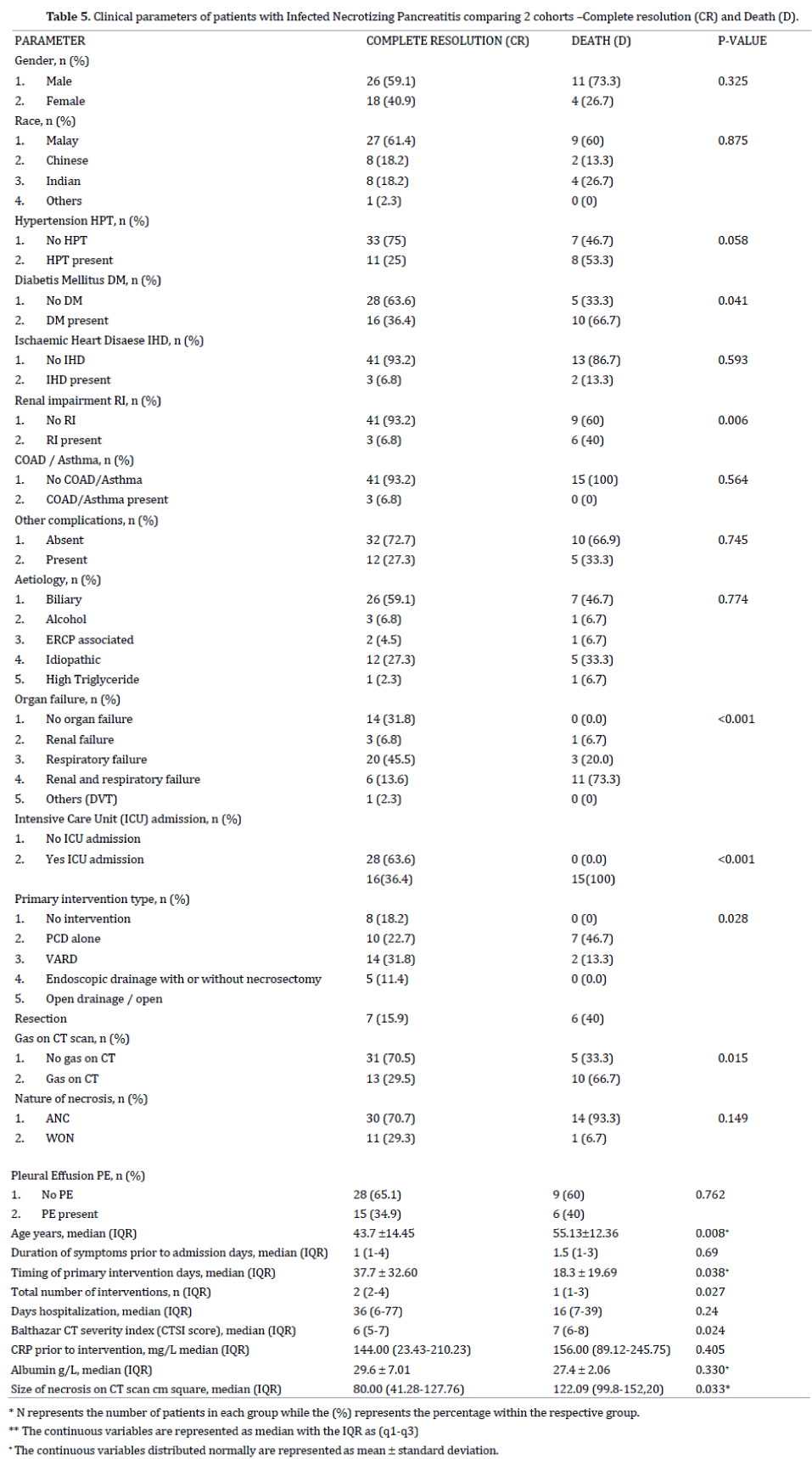
Organ failure (OF) and Intensive Care Unit (ICU)
Admission
There was a significant difference between the 2
groups in terms of OF (p < 0.001). 14 patients (31.8%)
in the CR group had no OF while there all patients in the D
group that had at least one OF. In the CR group, 3 (6.8%) and
20 (45.5%) had renal and respiratory failure respectively. 6
patients (13.6%) in the CR group had a combination of renal
and respiratory failure while 11 patients (73.3%) within the
D group had a combination of these 2 OF. 1 patient who had
DVT had CR. 15 patients (100%) within the D group had ICU
admission. Out of the 34 patients with CR 16 patients (36.4%)
were admitted to ICU while 28 (63.6%) did not require ICU
admission. Overall, a higher percentage of patients within the
Death group had 2 OF (renal and respiratory) (73.3% within
D group vs. 13.6% within the CR group).
Type and Timing of Primary Intervention and Total
Number of Intervention/s Performed
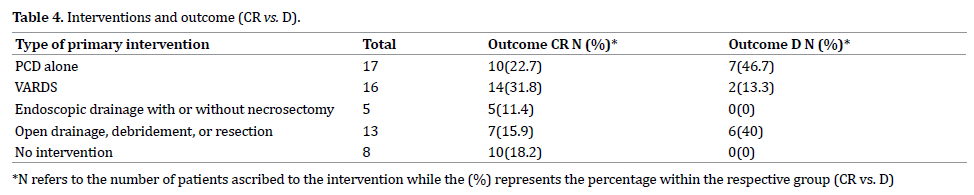
The commonest procedure performed was PCD alone
(17) and VARDS (16),followed by open drainage and
resection (13) and Endoscopic drainage with or without
necrosectomy (5). Table 4 summarizes the interventions
performed, number of patients and their outcomes. Of
the 15 patients who died, 7 (46.7%) were from the PCD
alone group, while 6 (40%) were from the open drainage
/ open resection group. Timing of primary intervention
was 37.7 +/- 32.60 days for patients in the CR group and
18.3 +/- 19.69 days in the D group (p = 0.038). Patients
in the D group had fewer number of interventions, 1(1-3)
compared to the CR group 2(2-4) (p = 0.0027)
CTSI score, Size of Necrosis, CRP Level Prior to
Intervention, Albumin Levels
Patients with CR had a lower median CTSI score of 6 (5-7)
compared to patients who died 7 (6-8) (p = 0.024). CRP (p
= 0.405) and Albumin (p= 0.330) levels prior to intervention
were similar in both groups. Size of necrosis on cross sectional
imaging was significantly higher in the D group compared to
the CR group (p = 0.033). Median size is 80.00 cm sq (41.28 –
127.76) in the CR group and 122.09 cm sq (99.8 – 152.20) in
the cohort of patients who died (Table 7, 8, 9).
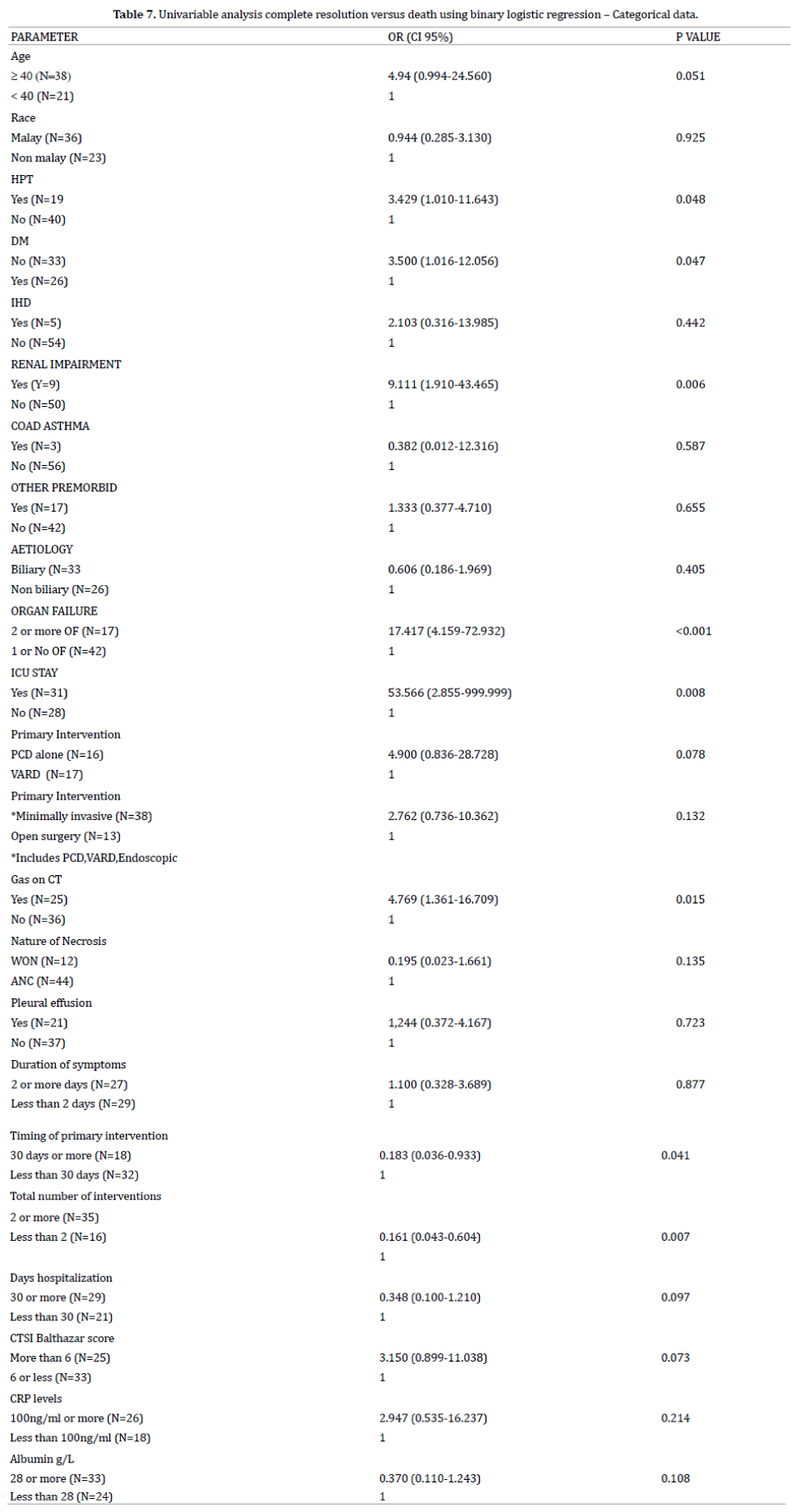
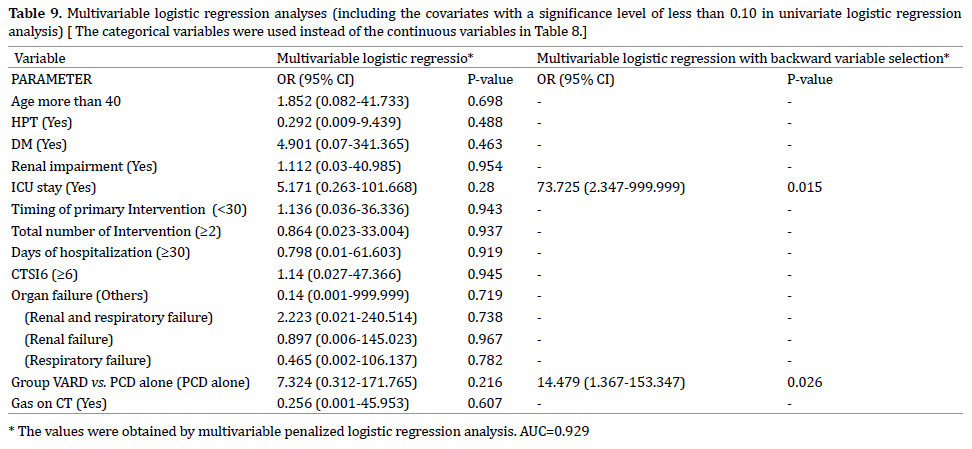
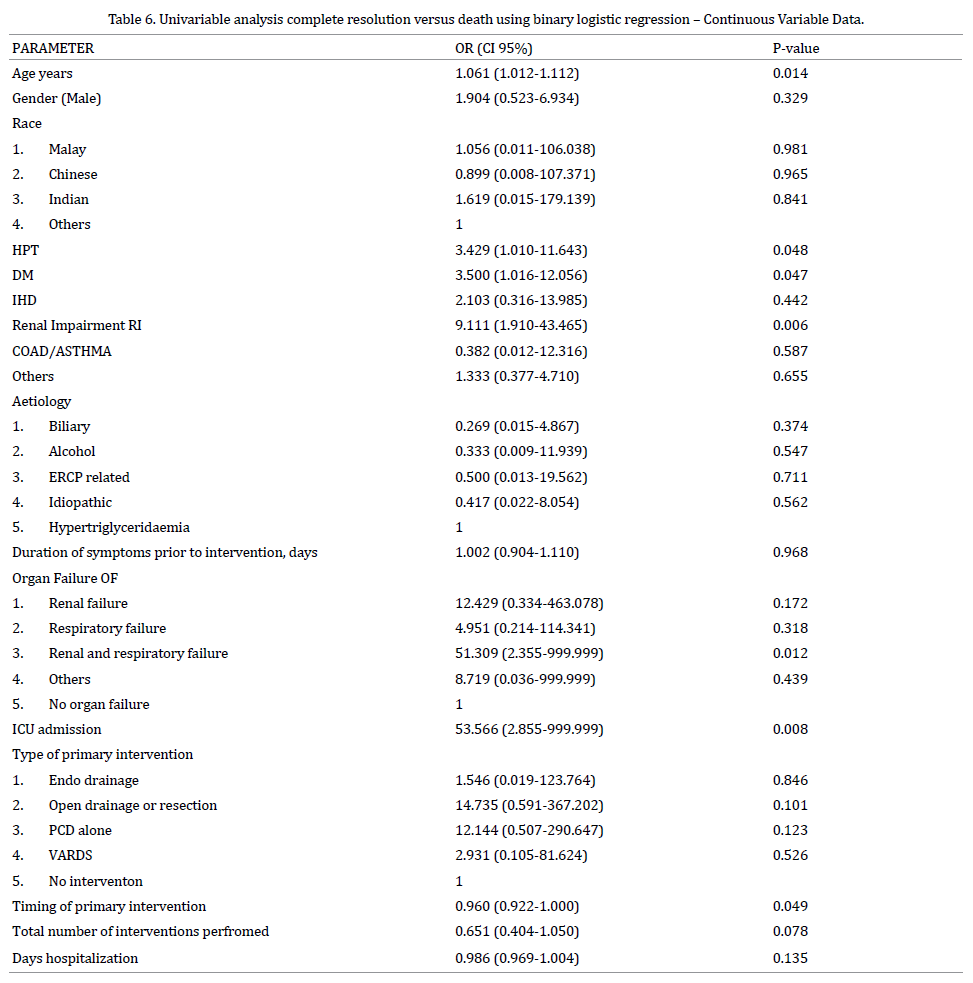
Factors Predicting Mortality
To identify the predictors of mortality, univariable and multivariable logistic regression analyses were performed for
Death compared to complete resolution. Univariable analysis
indicated that patients Age, presence of Hypertension and
Diabetis Mellitus, Renal Impairment, admission to ICU, organ
failure, intervention with PCD as oppose to VARDS and
presence of Gas on CT scan were significantly associated
with mortality. Penalized logistic regression analysis was
performed for some variables with one cell having zero
frequency in contingency tables.
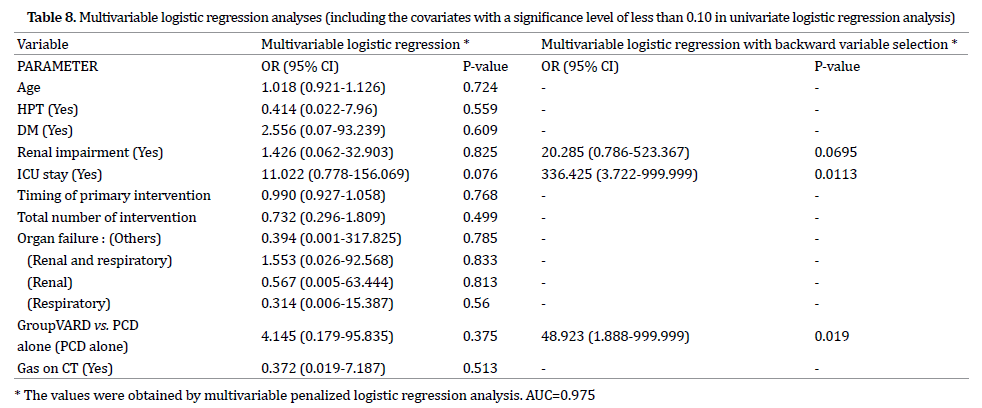
We fitted two separate multivariable models. The
first included the significant continuous variables and
categorical variables in univariate analyses. The second
model included the categorical variables created by their cut off values instead of continuous variables in the first
model.
These values in multivariable analyses were obtained
using a multivariable penalized logistic regression model.
The final models of these models using a backward variable
selection showed an Area under the Curve (AUC) of 0.975
for the first model and 0.929 for the second model. Renal
impairment, admission to ICU and intervention by PCD
were included in the final model of the first model and only
admission to ICU and intervention by PCD were included
in the final model of the second.
DISCUSSION
The present study highlights the different modalities
that have been employed in the management of patients
with infected NP within 2 of the main Hepatobiliary
centres in Malaysia. Over the last decade or so these
different modalities ranged from the traditional open
drainage and debridement to the less invasive PCD
and VARD, to modalities that require only drainage
without debridement notably PCD and endoscopic internal
drainage. Since the inception of the PANTER trial there has
been a paradigm shift towards doing less and “stepping
up” when required [5].
As we now understand that the necrosis that
develops may be pancreatic as well as extrapancreatic
(peripancreatic), there are still many questions to
be answered regarding the natural history of these
necrosums [11]. There still remains a question mark as
to which patients can be managed with drainage alone
and which would require additional debridement as well.
This is due the heterogenous nature of the necrosis. It
may be completely liquified, partially liquefied, softer
friable necrosis, more adherent and not easily flushed
suggesting that the process is an evolving one [11, 12].
The pragmatic approach would be to assume that all
patients with ANC require drainage possibly obviating
the need for debridement while those with WON require
drainage and debridement. Based on the revised Atlanta
Classification describing both ANC and WON, these
collections are still heterogenous collections and to
ascribe a particular treatment modality in terms of
drainage versus drainage and debridement is difficult.
However this is too simplistic.
Choosing a treatment modality should be based on
many factors not least institutional capabilities, the least
invasive route providing maximal clearance and tailored
towards the patients outcome rather than the anatomical
aspect of the necrosis. The nature of the necrosis has to be
taken into consideration as well. It is imperative to have a
standardize purpose so that the treatment modality can be
tailored to the purpose rather than vice versa. This would
include drainage, lavage, fragmentation, debridement, or
excision [13, 14]. As a result it would be difficult to compare
the outcome of different procedures as some patients who
are treated with drainage and debridement may eventually
improve even if debridement was not performed. The flip side is patients who are treated with prolonged drainage
with multiple insertions and upsizing my have improved if
debridement was performed earlier.
From our study the 2 most favoured methods were
PCD alone and PCD followed by VARDS. PCD alone was the
favoured modality of treatment in one of the institutions
while VARDS was favoured more in the other institution.
This practice reflects the institutional preference rather
than one intervention being superior than the other.
As previously mentioned, there are many factors
that predict mortality in patients with Severe Acute
Pancreatitis [15]. However not many studies have been
performed addressing the factors that predict mortality
in patients with infected NP undergoing intervention. A
large single centre retrospective study performed in the
US revealed the determinants of mortality were increasing
age, persistant organ failure and amount of necrosis..
Guo et al in a large prospective study showed that
persistant organ failure after one week, age, bacteremia
and pancreatic necrosis (as opposed to peripancreatic
necrosis) were predictors of mortality [15]. In the present
study, age, comorbidities such as Hypertension, Diabetis
Mellitus and Renal Impairment, ICU stay, Timing and
number of interventions, organ failure, Gas on CT scan,
type of intervention (VARDS vs. PCD alone) were factors
associated with higher mortality rates. However using
multiple penalized logistic regression analysis ICU stay
and PCD alone (compared to VARDS) were found to predict
mortality in our cohort of patients.
There is compelling evidence that the use of PCD alone
without a further “step up” procedure may be successful in
managing patients with infected NP with reported success
rates ranging from 50-55% and mortality rates harbouring
between 15 to 17% [7, 8]. However so, there are many factors
that have to be taken into consideration. Most of these studies
were retrospective cohorts and included patients with sterile
pancreatic necrosis. It is also difficult to ascertain for sure
whether these collections warranted drainage to begin with.
Also, approximately 10% of patients eventually succumbed
to death as they were deemed unfit for further intervention.
Although PCD was found to be an independent
predictor of mortality when compared to a VARD ( a “step
up” procedure in our case), we cannot conclude for sure
that VARD is superior to PCD. PCD was employed in all
patients undergoing VARD. The indication for PCD was to
drain any infected collection causing symptoms as well as
sepsis. There may be an inherent bias in one of the centres
to commit to VARD after PCD as part of the “step up
approach” even though the amount of debridement may
not have been significant, rather as a means for improved
lavage. Secondly, patients in the PCD alone group may
have been too ill to be subjected to another procedure, for
example VARD or open surgery accounting for the higher
mortality rate after this procedure.
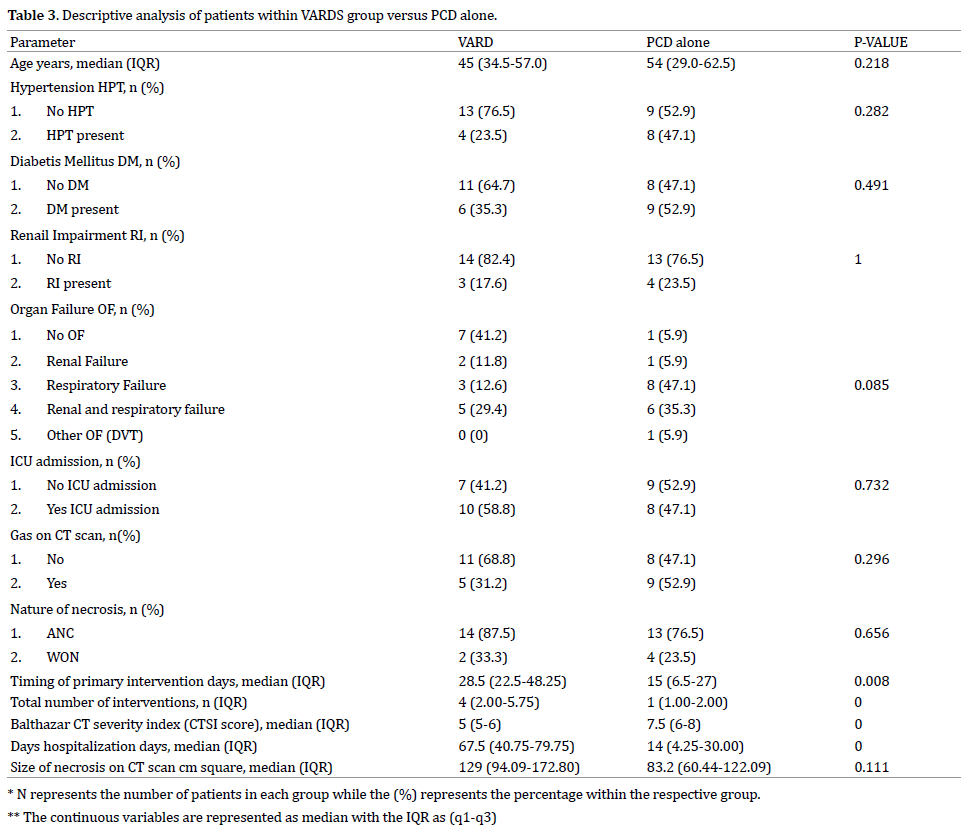
On a head to head comparison, patients in the PCD
alone group had significantly less interventions (median
= 1) performed compared to those in the VARD group (median = 4) (p < 0.0001) but significantly higher CTSI
score (median score of 5 for VARD group vs. 7.5 for PCD alone
group) (p < 0.0001). This difference in the CTSI score could
have accounted for the higher mortality rate. The fact
that the VARD group had higher number of interventions
could account for the fact that these patients were more
tolerant to repeated general anaesthesia while the patients
in the PCD group could have been more ill. Although not
statistically significant (p = 0.086), a higher percentage
of patients within the PCD alone group had a higher
percentage of organ failure, notably respiratory failure and
combination of respiratory and renal failure.
Our study had some noteworthy limitations. Our study
did not include the cause of death of the patients and it was
difficult to ascribe death due to the severity of pancreatitis
or the intervention performed. Secondly, the reason for
choosing one procedure over the other was not clearly
defined. Whether VARD was actually required as a means of
debridement or lavage was not clearly stated. In one of the
centres that favour PCD alone, a large number of patients
were transferred to other centres for continuation of care
and important information with respect to their progress
was not clearly documented.
However so, one important aspect that we have understood
is that NP is a very heterogenous disease. The natural history of
this disease is still not clearly understood. Most of the decisions
regarding intervention are based on institution preference and
available expertise. Perhaps defining the actual need or purpose
of intervention is more important.
CONCLUSION
Mortality rate still remains high in patients with
Infected NP undergoing intervention. Many of the factors
associated with mortality are not modifiable. The inherent
physiological insult resulting from the early systemic
response of SAP coupled by the further deterioration once
infection develops sets the tone for further deterioration.
The persistent organ failure requiring ICU admission
means that patients remain ill despite intervention. There
is no doubt that a step up approach is necessary as the
use of Percutaneous Catheter Drainage alone may not be
sufficient in a selected cohort of patients.
This points to the fact that repeated debridements
removing as much necrotic material may be required
However much has to be learned regarding the natural
history and nature of the infected necrosis so as to choose
the appropriate treatment. We welcome further prospective
studies evaluating this. Deciding on which patients will
recover with drainage alone while deciding on an appropriate
step up to further remove all necrotic tissue is paramount.
Conflicts of interest
The authors had no conflicts of interest to declare in
relation to this article.
References
- Kandasami P, Harunarashid H, Kaur H. Acute pancreatitis in a multi-ethnic population. Singapore Med J 2002; 43:284-8. [PMID: 12380724]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013; 62:102-11. [PMID: 23100216]
- Petrov MS, Shanbhag S, Chakraborty M, Philips AE, Windsor JA. Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis. Gastroenterology 2010; 139:813-20. [PMID: 20540942]
- van Santvoort HC, Besselink MG, Bakker OJ, Hofker HS, Boermeester MA, Dejong CH, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med 2010; 362:1491-502. [PMID: 20410514]
- Garg PK, Madan K, Pande GK, Khanna S, Sathyanarayan G, Bohidar NP, et al. Association of extent and infection of pancreatic necrosis with organ failure in acute necrotizing pancreatitis. Clin Gastroenterol Hepatol 2005:3:159-166. [PMID: 15704050]
- Freeman ML, Werner J, van Santvoort HC, Baron TH, Besselink MG, Windsor JA, et al. Interventions for Necrotizing Pancreatitis, summary of a multidisciplinary consensus conference. Pancreas 2012; 41:1176-94. [PMID: 23086243]
- Ke L, Li J, Hu P, Wang L, Chen H, Zhu Y. Percutaneous Catheter Drainage in Infected Pancreatitis Necrosis: a Systematic Review. Indian J Surg 2016; 78:221–228. [PMID: 27358518]
- van Baal MC, van Santvoort HC, Bollen TL, Bakker OJ, Besselink MG, Gooszen HG. Gooszen for the Dutch Pancreatitis Study Group. Systematic review of percutaneous catheter drainage as primary treatment for necrotizing pancreatitis. Br J Surg 2011; 98:18-27. [PMID: 21136562]
- Besselink MG, Verwer TJ, Schoenmaeckers EJ, Buskens E, Ridwan BU, Visser MR, et al. Timing of Surgical Intervention in Necrotizing Pancreatitis. Arch Surg 2007; 142:1194-1201. [PMID: 18086987]
- Mier J, León EL, Castillo A, Robledo F, Blanco R. Early versus late necrosectomy in severe necrotizing pancreatitis. Am J Surg 1997; 173:71-5. [PMID: 9074366]
- Beger HG, Rau B, Isenmann R. Natural History of Necrotizing Pancreatitis. Pancreatology 2003; 3-93-101. [PMID: 12774801]
- Bakker OJ, van Santvoort H, Besselink MG, Boermeester MA, van Eijck C, Dejong K, et al. Extrapancreatic necrosis without pancreatic parenchymal necrosis: a separate entity in necrotising pancreatitis?. Gut 2013; 62:1475–1480. [PMID: 22773550]
- Tenner S, Baillie J, DeWitt J, Vege SS; American College of Gastroenterology. ACG Clinical Guideline: Management of Acute Pancreatitis. Am J Gastroenterol 2013; 108:1400–1415. [PMID: 23896955]
- Loveday BP, Petrov MS, Connor S, Rossaak JI, Mittal A, Phillips AR, et al. A Comprehensive Classification of Invasive Procedures for Treating the Local Complications of Acute Pancreatitis Based on Visualization, Route, and Purpose. Pancreatology 2011; 11:406-413. [PMID: 21894058]
- Guo Q, Li A, Xia Q, Liu X, Tian B, Mai G, et al. The Role of Organ Failure and Infection in Necrotizing Pancreatitis. Ann Sur 2014; 259:1201-1207. [PMID: 24169172]


