Keywords
Hereditary pancreatitis
Abbreviations
DNA Deoxyribonucleic acid; ICP Idiopathic chronic
pancreatitis; PCR Polymerase chain reaction
INTRODUCTION
Chronic pancreatitis (CP) is an inflammatory condition
of the pancreas seen as irreversible morphological
changes that results in exocrine or endocrine deficiency
[1, 2]. In clinical practice evaluation fails to detect the
cause of pancreatitis in nearly 10–30% of the patients,
and these patients are labeled as idiopathic CP [3]. Many
studies have been conducted on acute and CP, but only
few have focused on idiopathic CP. Idiopathic CP was
earlier thought to be seen only in certain parts of India
[4]. During the last few years, many cases of idiopathic
CP have been reported from western world and almost
all states in India [5].
The SPINK1 is also known as pancreatic secretory
Trypsin inhibitors located on chromosome 5. It is a 56
amino acid peptide that inhibits Trypsin by physically
blocking the active site [6, 7]. Provides the first line
defense against premature Trypsinogen activation within
pancreas, because it is capable of inhibiting about 20%
of Trypsin activity by competitively blocking the active
site of Trypsin. In 2000, the role of SPINK 1 mutation in
chronic pancreatitis emerged. The most frequent mutation
in (SPINK1) gene exon 3 results in asparagine to serine
amino acid change (N34 S) which leads to decreased
trypsin inhibitory capacity. SPINK 1 (N34S), mutation are
relatively common seen in 2% of general population.
Mutations in cationic trypsinogen gene (PRSS1), SPINK1
gene, cystic fibrosis transmembrane conductance regular
gene (CFTR) and Cathepsin B gene have been studied in
acute recurrent and CP [8]. Genetic mutations may be the
cause of pancreatitis in patients whom etiology is not found
[9]. Idiopathic pancreatitis represents a complex disease
process resulting from an interaction of genetic mutations
and environmental factors. Recent research has shown
complex interactions like gene –gene, gene – environment
in the pathogenesis of pancreatitis [10]. Mutations in
SPINK1 gene, is associated with ICP but its prevalence may be under determined. Hence a prospective study on ICP
and prevalence of SPINK 1 mutation was studied.
MATERIALS AND METHODS
The study was a prospective analysis of patients
with idiopathic CP during the period October 2010 to
December 2011. It was conducted at the Department of
Gastroenterology PSG Institute of Medical Sciences and
Research (PSG IMSR) in collaboration with the Centre for
Molecular Medicine and Treatment. The study protocol was
approved by the Institutional Human Ethics Committee
prior to the start of the study.
Patients underwent routine hematological and
biochemical tests in addition to radiological imagings like
Ultrasound and Computed tomography. Complications of
CP like diabetes mellitus, steatorrhea, bile duct obstruction,
and pseudocyst were diagnosed as per standard criteria
either biochemically or imaging.
Inclusion Criteria for Idiopathic Chronic pancreatitis
1. Documented episodes of typical pancreatic type of
abdominal pain
2. Amylase or lipase greater than 3 times the upper
limit of normal
3. Features of pancreatitis on imaging studies
(ultrasound / CT abdomen)
4. No identifiable cause or risk factors
Exclusion Criteria
Patients with identifiable cause and risk factors for
acute and recurrent pancreatitis, malignancy, retroviral
infection, Psychiatric illness, hereditary and known genetic
diseases.
Genetic analysis: It involved DNA extraction, PCR to
amplify SPINK gene, RFLP using PST I restriction enzyme
and Poly Acrylamide Gel Electrophoresis (PAGE) of the
digested product.
DNA Extraction Procedure
Blood sample 300 μL + 1 volume of cell lysis buffer + 3
volume of sterile MilliQ water mixed up in 2 mL Eppendorf
tubes which were then incubated on the ice 4°C for 10
minutes. The samples centrifuged at 4°C for 20 minutes at
4000 rpm. The supernatant discarded and again 150μl of
same cell lysis buffer added in every sample and 480 μL of
autoclaved H2O also added. The sample then centrifuged at
4°C for 20 minutes at 4000 rpm. Then again the supernatant
was discarded. Then 720 μL of nucleic acid lysis buffer,
along with add 15 μL of RNAse added to the eppendorf tube.
The samples were vortex mixed and incubated for 10 -15
minutes at 37°C. 30 μL of 10% SDS and 30 μL of Proteinase
K then added. The sample was incubated in water bath or
heat block at 55°C for 2-3 hours. Equal volume of phenol:
chloroform (1:1) added and centrifuged at 15800rpm for 5
minutes. The supernatant of the samples (aqueous layer)
transferred to the new tube.
PCR amplification of SPINK gene
1. Primers
Forward primer SPINKF: TTCTGTTTAATTCCATTTTTAGGCCAAATGCTGCA
Reverse primer SPINKR: GGCTTTTATCATACAAGTGACTTCT
2. DNTPs (Himedia)
3. Taq DNA polymerase (colorless Taq Genei)
4. Taq Buffer A (Genei)
5. DNA Sample Optimised concentration: 0.05μg
6. Milliq water
Identification of Genotypes
The genotypes were determined based on the expected
product size.
A/A Genotype (Asn 34 Asn) - 320bp
G/G Genotype (Ser 34 Ser) - 286bp
A/G Genotype (Asn 34 Ser) - 320,286 and 34
Peripheral blood samples were drawn from patients
and collected in EDTA tubes. DNA was isolated using
Micro AX Blood Gravity Kit (A&A Biotechnology, Gdańsk,
Poland). Quality and concentration of isolated DNA was
measured by Nano Drop 2000 (Thermo Scientific, TK
Biotech, Poland). Genotyping was performed using the
following molecular biology techniques: allele-specific
PCR (ASA-PCR) and high-resolution melting (HRM)-PCR.
Statistical analysis: Descriptive statistics were used to
summarize the variables. All data were analyzed using the
statistical package SPSS (version 10.0).
RESULTS
33 patients were included with mean age of 31.75±13.07
years with youngest being 9 yrs and oldest being 69 yrs.
22 (67%) of patients were males, 11 (33%) were females.
Mean age of patients with Spink positive was 31.96±9.25
yrs. The mean duration of illness was 31.33±19.89 months.
Mean fasting sugar level was 112.57±12.53 mg/dL. Of the
33 patients 12 (36%) were positive for SPINK-1 mutation.
Mutant genotype was seen in the age group of 11-20 years.
6 patients had heterogeneous genotype in the age group of
21-30, 2 each in the age group of 31-40 and 41-50 (Figure
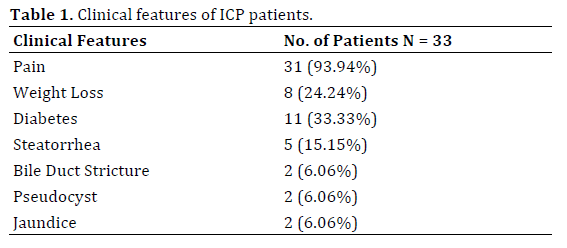
1). Most of the patients’ positive for the SPINK-1 mutation
had a younger age of onset. Nearly 93.34% of patients had
pain as their clinical symptoms. The clinical manifestations
are given in Table 1. Nearly 26/33 (78.78%) of patients
had no evidence of malnutrition as evidenced by BMI>18.5.
25/33 (73.75%) patients had ductal dilation and around
29/33 (87.87%) had parenchymal calcification (Table 2).
All the patients with SPINK positive had 100% parenchymal
calcification. Spink mutation is given in Figure 2.
Figure 1: Age wise distribution of ICP patients with genotype.
Figure 2: Spink mutation in ICP patients.

Most of the patients in both the group were below 30
yrs. Male preponderance was seen. 36.36% of patients with idiopathic CP were positive for SPINK1 mutation.
Pain was predominant symptom and diabetes was seen
only in 11 (33.33 %).
DISCUSSION
The mean age of ICP was 31.75±13.07 years
which resembles the age group given in other studies.
Balakrishnan et al. showed mean age of patients was 30
years [11]. Data from Layer et al. from United States had
mean age of 19 yrs. [12]. Kandula et al. showed idiopathic
CP occurred among children and adolescents [13]. The
mean age of patients from northern India in a survey was
36.7 years and study from New Delhi showed majority of
patients were younger [14, 15].
Majority of the patients in our study were male (67%).
Data from prospective nationwide study from India showed male preponderance [16]. Study by Balakrishnan et al. showed male to female ratio of 2.7:1 [11]. A study
from Delhi and Lucknow showed majority of their patients
with tropical pancreatitis were males [17, 18]. In our study
mean duration of symptoms at the time of presentation
was 31 months. The study from Delhi reported mean
duration of 48 months while Shallu Midha et al. showed in
their study mean duration was 27 months [17, 18].
Pain was the common presentation in our study
which was similar to other studies by Layer et al. [12],
Balakrishnan et al. [11], Midha et al. [18] reported 97%
presented with pain which was similar to our data. Diabetes
was reported in 33% of patients in our study which is
different from study conducted by Geeverghese [19] and
Tandon et al. who in their study showed upto 90% of
patients having diabetes [12]. The study by Balakrishnan et al. also showed higher incidents of diabetes upto 70%
[16]. The study from Lucknow reported diabetes in 26% of
patients with idiopathic CP. Midha et al. also reported 27%
patients having diabetes in chronic idiopathic pancreatitis
[18].
In our study symptomatic steatorrhea was seen
around 15% while Midha et al. reported frequency of 5%
steatorrhea in their study [18] and data from New Delhi
also showed around 5% of patients with steatorrohea
[17]. The present study showed 26 (78%) of patients
with BMI>18.5 and 9 (22%) with BMI<18.5. This is in
contrast to older studies from Kerala which showed high
incidence malnutrition. Midha et al. and Narendranathanshowed
lack of association of malnutrition and Cassavsa
consumption in their study [19, 20]. In 1988 study by
Balakrishnan implicates malnutrition in pathogenesis of tropical calcific pancreatitis [16]. The study from lucknow
and delhi showed mean BMI of 19 kg/m2 and 20.2 kg/m2 [17].
Ultrasound and CT findings included dilated
pancreatic duct, calculi, atrophy. CT was more sensitive in
identifying ductal dilatation and calcification. Study from
all India institute of medical science showed usefulness
ultrasonographic evaluation of calcific pancreatitis [15].
Sensitivity of identifying ductal dilatation and calcification
is less than CT abdomen or MRI. In our study 87.87% had
parenchymal calcification 75% had ductal dilation and
only 21% had ductal calculi. The study from Lucknow
reported 57% of their patients with tropical pancreatitis
had calcification. Khuroo et al. reported 96% of patients
with tropical calcific pancreatitis had pancreatic ductal
calculi [21]. All the 12 patients with SPINK mutation had
12(100%) parenchymal calcification and 9 (75%) atrophy
of pancreas on CT.
The etiology of idiopathic pancreatitis is not well
known. Recent studies have implicated SPINK 1 and
CFTR gene in idiopathic CP. Study by Pfutzer et al. [22],
Sundaresan et al. [23] have shown strong association
of tropical calcific pancreatitis with SPINK 1 Our study
showed 36.36% of patients with SPINK mutation .The
study of Bhatia et al. showed SPINK 1 mutation was found
in 40% of patients with tropical idiopathic CP in India. In
a study from Bangladesh Schneider et al. showed there
was difference in SPINK1 mutation between patients with
tropical calcific pancreatitis with and without diabetes. An
Italian study by Macarena Gomez - showed association of
SPINK 1 and CFTR gene mutation in idiopathic pancreatitis
[24]. In addition to SPINK1, CFTR gene mutations have
been found in patients with CP than controls. The data
from AIIMS showed 42% of patients had SPINK mutation
and 9% CFTR mutation in patients with idiopathic CP.
Studies from south India showed SPINK gene mutations
were common in patients with idiopathic chronic patients.
Thus genetic mutations seen to play as important
role in the pathogenesis of idiopathic CP. Recent study
have shown role of chymotrypsin C gene mutation in
idiopathic CP which lands support to the genetic theory of
etiopathogenesis of idiopathic CP. The present study shows
phenotypic and genetic similarities between idiopathic CP
in India and in other countries [25, 26].
Our study reveals that spink mutation is strongly
associated with more number of acute episodes in RAP
and parenchymal calcification in CP. It may be useful to
do functional studies of SPINK 1 mutation in cell cultures
to understand the pathophysiology of the disease status
more completely. Clinical profile of idiopathic chronic
pancreatitis is different from what has been reported
previously. Genetic testing and screening may be proposed
to have role in diagnosis, prediction of clinical features and
severity in future.
Conflict of Interest
The authors declare that there is no conflict of interests
regarding the publication of this paper.
References
- Forsmark CE. Chronic Pancreatitis. In: Sleisenger MH, Feldman M, Friedman LS, Brandt LJ. Sleisenger and Fordtran's gastrointestinal and liver disease: Pathophysiology, diagnosis, management. 10th ed. Philadelphia, Saunders 2015; 994-1026.
- Owyang C, DiMagno MJ. Chronic pancreatitis. In: Yamada T, Alpers DH, Kalloo AN, Kaplowitz N, Owyang C, Powell DW, editors. Textbook of Gastroenterology 5th ed. Philadelphia, Pennsylvania, USA. 2009; 1811–52.
- Conwell DL, Wu BU. Chronic pancreatitis: making the diagnosis. Clin Gastroenterol Hepatol 2012;10:1088-95. [PMID: 22642958]
- Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology 2013; 144:1252–61. [PMID: 23622135]
- Yadav D, Timmons L, Benson JT, Dierkhising RA, Chari ST. Incidence, prevalence, and survival of chronic pancreatitis: a population-based study. Am J Gastroenterol 2011; 106:2192-9. [PMID: 21946280]
- Ogawa M. Pancreatic secretory trypsin inhibitor as an acute phase reactant. Clin Biochem1988; 21:19-25. [PMID: 2449986]
- Whitcomb DC. Genetic predispositions to acute and chronic pancreatitis. Med Clin North Am 2000; 84:531-547. [PMID: 10872412]
- Sobczyńska-Tomaszewska A, Bak D, Oralewska B, Oracz G, Norek A, Czerska K, Mazurczak T, et al. Analysis of CFTR, SPINK1, PRSS1 and AAT mutations in children with acute or chronic pancreatitis. J Pediatr Gastroenterol Nur 2006; 43:299-306.
- Gomez-Lira M, Bonamini D, Castellani C, Unis L, Cavallini G, Assael BM, Pignatti PF. Mutations in the SPINK1 gene in idiopathic pancreatitis Italian patients. Eur J Hum Genet 2003; 11:543–546. [PMID: 12825076]
- Pfützer RH, Barmada MM, Brunskill AP, Finch R, Hart PS, Neoptolemos J, Furey WF, Whitcomb DC. SPINK1/PSTI polymorphisms act as disease modifiers in familial and idiopathic chronic pancreatitis. Gastroenterology 2000; 119:615–23. [PMID: 10982753]
- Balakrishnan V, Nair P, Radhakrishnan L, Narayanan VA. Tropical pancreatitis- a distinct entity ormerely a type of chronic pancreatitis? Indian J Gastroenterol 2006; 25:74-81. [PMID: 16763335]
- Layer P, Yamamoto H, Kalthoff L, Clain JE, Bakken LJ, DiMagno EP. The different courses of early- and late-onsetidiopathic and alcoholic chronic pancreatitis. Gastroenterology 1994; 107:1481-7.
- Kandula L, Whitcomb DC, Lowe ME, Genetic issues in pediatric pancreatitis. Curr Gastroenterol Rep 2006; 8:248-53. [PMID: 7926511]
- Garg PK, Tandon RK. Survey on chronic pancreatitis in the Aisa Pacific egion. J Gastroenterol Hepatol 2004;19:998-1004. [PMID: 15304116]
- Choudhuri G, Bhatia E, Sikora SS, Alexander G. Tropical pancreatitis in North India. In: Chronic pancreatitis and Pancreatic Diabetes in India Balakrishnan V, Kumar H, Sudhindran S, Unnikrishnan AG, eds (Indian Pancreatitis study Group) 2006; 53-9.
- Balakrishnan V, Unnikrishnan AG, Thomas V, Choudhuri G, Veeraraju P, Singh SP, Garg P, et al. Chronic pancreatitis: a prospective nationwide study of 1,086 subjects from India. JOP 2008;9:593-600. [PMID: 18762690]
- Garg PK. Chronic Pancreatitis: The AIMS, New Delhi experience. In: Chronic Pancreatitis and Pancreatic Diabetes in India Balakrishnan V, Kumar H, Sudhindran S, Unikrishnan AG, eds (Indian Pancreatitis Study Group) 2006; 61-76.
- Midha S, Singh N, Sachdev V, Tandon RK, Joshi YK, Garg PK. Cause and effect relationship of malnutrition with idiopathic chronic pancreatitis: prospective case control study. J Gastroenterol Hepatol 2008; 23:1378-83.
- Geeverghese PH. Pancreatic diabetes: a clinicopathological study of growth onset diabetes with pancreatic calculi. Mumbai, India: Popular Prakashan; 1968.
- Balakrishnan V, Sauniere, Hariharan M, Sarles H. Diet, pancreatic function and chronic pancreatitis in South India and France. Pancreas 1988; 3:30-5. [PMID: 3362842]
- Khuroo NS, Khuroo MS, Khuroo MS. Anomalourspancreaticobiliary ductal union in
tropical calcific pancreatitis. JOP.J Pancreas (Online) 2010; 11:18-24. [PMID: 20065547]
- Pfutzer RH, Whitcomb DC. SPINK 1 mutations are associated with multiple phenotypes. Pancreatology 2001; 1:457-60. [PMID: 12120224]
- Sundaresan S, Chacko A, Dutta AK, Bhatia E, Witt H, TeMorsche RH, Jansen JB, et al. Divergent roles of SPINK 1 and PRSS2variants in tropical calcific pancreatitis. Pancreatology 2009; 9:145-9. [PMID: 19077465]
- Schnerder A, suman A, Rossi L, Barmada MM, Beglinger C, Parvin S, Sattar S, et al. SPINK1/PSTI mutations are associated with tropical pancreatitis and type II diabetes mellitus in Bangladesh. Gastroenterology 2002; 123:1026-30. [PMID: 12360464]
- Lira MG, Bonamini D, Castellani C, Unis L, Cavallini G, Assael BM, Pignatti PF. Mutations in the SPINK1 gene in idiopathic pancreatitis Italian patients. Eur J Hum Genet 2003; 11:543-6. [PMID: 12825076]
- Midha S, Khajuria R, Shastri S, et al. Idiopathic chronic pancreatitis in India: phenotypic characterization and strong genetic susceptibility due to SPINK 1 and CFTR gene mutations. Gut 2010; 59:800-7. [PMID: 20551465]



