Keywords
Drug-Eluting Stents; Hemorrhage; Pancreatic Fistula
Abbreviations
IR interventional radiology; POH post-operative
hemorrhage
INTRODUCTION
Post-operative hemorrhage (POH) after pancreatic
surgery is a life-threatening complication [1, 2, 3]. Its
incidence remains between 1.5% and 15% with a mortality
rate from 0 to 5% [4]. Delay between surgery and POH
defined early POH (≤24 hours or <3 days) and delayed
POH (>24 hours or >8 days) [5, 6].
Early post operative hemorrhage is mainly due to
technical failure and is essentially treated by reintervention
[5] but IR may be used in certain cases.
Delayed POH is generally due to a postoperative
pancreatic fistula (POPF) and its exposes to two main issues
problems: a) a difficult surgical approach of the bleeding
zone increasing with the delay from surgery [7], and b) the
necessity to treat the POPF with a high rate of completion
pancreatectomy [8]. In this setting, interventional radiology
(IR) (angiography with transarterial embolization (TAE)
or stent placement) [7, 9], has become the preferred
approach in hemodynamically stable patients presenting
with delayed POH.
However, surgery is still indicated for delayed
hemorrhage in various situations. Hemodynamic
instability is the main indication but other diagnosis
requiring surgery such as associated peritonitis, grade C
POPF… could benefit from reintervention. Moreover, in non
tertiary referral centers, delay from surgery, experience of
the IR team, anatomic features of the patient precluding
IR, available material for IR (stent, coils, of different size...)
are all component to be considered to choose between
reintervention or IR.
Reintervention for delayed POH is very difficult and
ligature in adverse local condition during surgery could
explain that re-bleeding is not rare notably if the pancreatic
anastomosis/remnant is preserved. Recurrence of bleeding
is elevated, up to 27% [10, 11, 12] after intervention. Thus,
hazardous hemostasis could justify another therapeutic
option to complete the surgical treatment. We supported
that surgery and IR are not exclusive choice and could be
complementary procedure. IR could avoid re-bleeding
after surgery and secure the surgical ligature.
We reported our experience in management of delayed
POH needing surgical treatment immediately followed by
IR in order to reduce re-bleeding.
CASES
From 2000 to 2015, 899 patients underwent a
pancreatic resection in our department. All clinical,
biological and radiologic data were prospectively collected
in our database. Patients with delayed postoperative
hemorrhage were included and analyzed. We focused on patients with severe delayed POH with hemodynamic
shock needing emergency reintervention.
Hemorrhage was defined using the definition of
the ISGPF as postoperative evidence of bleeding in the
abdominal drain superior to 300 mL or the nasogastric
tube or external bleeding from the gastrointestinal tract.
Hemodynamic shock was defined as hypotension, or
rapid heart rate superior to 90/min or both. Management
of POH has been standardized in our department since
2007. In case of early postoperative hemorrhage (before
postoperative day 3), a reintervention is indicated in most
of cases. IR is performed for delayed POH depending of the
hemodynamic status.
We decided to focus on patients presenting a delayed
POH associated with hemodynamic instability requiring
emergency surgery because of the life-threatening situation
and the impossibility to securely use an interventional
radiologic procedure.
Of the 899 patients, 70 of them (7.8%) presented
a postoperative hemorrhage. Obviously, because of
hemodynamic shock, an interventional radiologic
procedure was not possible. An emergency surgery
was performed to stop the bleeding and stabilized the
patient. However, at the end of the intervention, because
of the adverse local conditions during reintervention,
the difficulty to perform a correct and secure hemostasis
of the bleeding vessel, the friability of the tissues due to
inflammation, we decided to manage them by surgery
immediately followed by IR. We report how we particularly
managed three cases of delayed hemorrhage.
Case #1
A Seventy-eight-year old male with jaundice and
weight loss was diagnosed with an intrapancreatic
cholangiocarcinoma and underwent pancreaticoduodenectomy
with pancreaticojejunostomy. Five days after surgery, he
presented a massive POH with hemodynamic shock. Emergency
laparotomy revealed a massive bleeding from the stump of the
gastroduodenal artery (GDA), which was controlled by direct
suture sparing the common hepatic artery. No pancreatic
fistula was detected intraoperatively. The pancreatic
parenchyma was soft with a small main pancreatic duct with
a high risk to develop a POPF. In this setting placement of a
stent in order to cover the stump of the GDA (Figures 1, 2)
was considered to avoid a secondary bleeding. Procedure
was performed 24 hours after surgery. The patient
eventually developed POPF on postoperative day 9
without bleeding recurrence and was discharged on POD
23.
Figure 1. Angiography from the celiac trunk (A) angiography showing the stump of the gastroduodenal artery (GDA).
Figure 2. Stent covering the stump A and B: Covered stent-graft in the common hepatic artery.
Case #2
A Sixty-four-year-old man with jaundice, anorexia and
weight loss was diagnosed with ampullary carcinoma.
Sixth day after PD with pancreaticojejunostomy, he
developed POPF. On POD 8, the patient presented a
POH with hemodynamic shock. Emergency laparotomy
revealed a bleeding arising from the stump of the GDA and controlled by a ligature sparing the common hepatic artery.
Completion of pancreatectomy was decided because of
the complete disruption of the pancreatic anastomosis.
Ligation of the stump of the GDA was performed in fragile
tissue due to impregnation of pancreatic juice. Hence stent
placement to avoid a recurrent hemorrhage was decided
and successfully performed 12 hours later. The patient
was discharged on POD 24.
Case #3
A Fifty-three-year-old woman was diagnosed with
a pancreatic tail adenocarcinoma and underwent
splenopancreactectomy with elective ligation of the main
pancreatic duct and overlock on the pancreatic section.
Seven days after surgery, she experienced a brutal pain
with hemodynamic shock and blood exteriorization from
the drain. Emergency laparotomy revealed a bleeding from
the stump of the splenic artery, which was ligated. A POPF
was detected; obviously form the pancreatic section and
drained. However, we decided a TAE, 6 hours after surgery, of the ligated splenic artery to not expose the patient to
another bleeding.
The patient was discharged home 19 days after
reintervention.
Interventional Radiology Procedure
Operating procedure was performed under digital
subtraction angiography. The Seldinger technique was
used to puncture the femoral artery inserted a 6F arterial
catheter sheath (Terumo). Then a 5F radiography catheter
was used to conduct celiac artery angiography (Terumo,
Cobra, Somerset, Cook) and a 0.035-inch ultra-smooth black
guide wire to superselect the radiography catheter for hepatic
or splenic artery radiography. The target vessel was identified
by visualization of irregularity or pseudoaneurysm or active
contrast extravasation. In the two first cases, gastroduodenal
artery stump was irregular so that a covered stent placement
was decided (Abbott). In the third case, an embolization
was performed with embolic agents type gelatin sponge
(Gelitaspon) (Table 1).
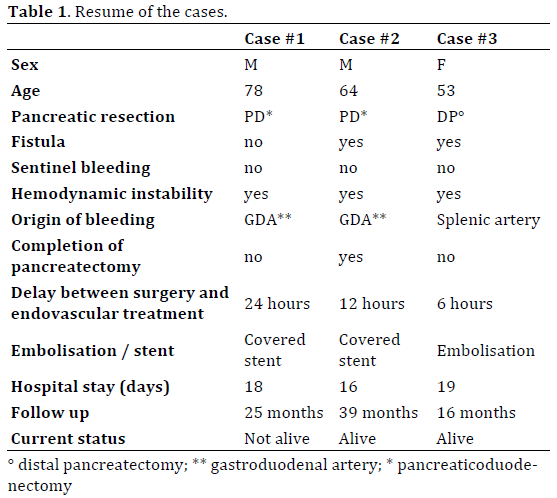
None of the three patients presented re-bleeding.
Hospital stay was 18, 16 and 19 days respectively. All the
cases were respectively followed 25, 39 and 16 months.
The first patient died after 25 months because of a
recurrence of his pathology.
DISCUSSION
Arterial bleeding occurs as a result of inflammatory
vascular erosion related to pancreatic juice or bile leaking
from an insufficient anastomosis and/or due to local
infection [13]. It has been proven that in case of POH a
prompt treatment either by IR or surgery is necessary
because it is very unlikely that a patient with a pancreatic
leak-related hemorrhage will be treated successfully with
conservative measure [14, 15].
When POH is related to a POPF, recurrence of bleeding
is elevated, up to 27% [10, 11, 12] after reintervention
and up to 18% after IR [10, 11, 12, 16, 17, 18] notably if
it was choose a conservative treatment of the pancreatic
anastomosis (IR or reintervention without completion of
the pancreatectomy). Pottier et al. showed that after a first
endovascular procedure for delayed POH, the reebleding
rate is high and 25% of the patient will experienced
a novel hemorrhage following the IR procedure [19].
Completion of pancreatectomy is sometimes decided
due to total disruption of the pancreatic anastomosis
or septic local condition. However, conservation of the
pancreatic anastomosis or the pancreatic remnant should
be considered and was successfully reported during
reintervention for POH in around 40% of cases in the
literature [20, 21]. Consequently, a pancreatic surgeon
faced a dilemma: completion of the pancreatectomy to
avoid another dramatic bleeding or conservation of the
pancreatic anastomosis/remnant with high risk of rebleeding.
However, completion pancreatectomy is often
difficult, due to bad local condition, with a high morbidity
and mortality [8]. We showed that reintervention
completed by IR should be a serious option to preserve, when appropriate, the pancreatic remnant, and to decrease
the risk of re-bleeding.
However, we have to highlight several points. First, we
did not know if these 3 patients would have experienced a
re-bleeding if we only perform a reintervention. But, again,
re-bleeding after re-intervention is not rare and usually
arises from the same vessel. Moreover, we could not
measure a subjective point: the local condition of the vessel
control. Indeed, ligaturing a vessel that was in contact with
pancreatic juice did not provide an experienced pancreatic
surgeon a satisfaction. Sensation of fragility and suspicion
of failure of this ligation are not measurable but strongly
impacted us to going further than sole reintervention.
Second, we supported that leaving a long stump of the
GDA, when oncologically possible, is a crucial point during
PD [22]. Thus, during reintervention, we could easily made
a new ligature of the GDA without injury/stenosis of the
common hepatic artery. Moreover, stent placement during
IR was easy and safe. Third, IR after reintervention should
not provoke specific morbidity. We did not experience IRrelated
morbidity in our 3 patients. However, it will not be
supportable to have an arterial disruption or thrombosis
to prevent a hypothetic risk. We supported that IR had to
be performed in the presence of the pancreatic surgeon to
choose or not to achieve the stent placement. For example,
if anatomy of the celiac trunk did not permit radiologist to
place a stent, they could decide to make a TAE of the hepatic
artery [9, 23, 24, 25, 26]. This should not be achieved to
not expose the patient to hepatic ischemia and related morbidity: the pancreatic surgeon had to be in the IR room
to stop the procedure because the pancreatic surgeon is the
most aware physician of post pancreatectomy morbidity.
Fourth, IR was performed several hours following the
reintervention but we did not have recommendation about
the maximum delay between reintervention and IR. Delay
between surgery and IR was from 6 to 24 hours, depending
on hemodynamic status after surgery. We supposed that IR
had to be achieved after patient hemodynamic stabilization
and during the first post reintervention day because rebleeding
could occurs from this date. In certain centers
distant from a department specialized in endovascular
treatment, a delayed support could be fatal for the patient.
Theses cases of life-threatening complication illustrate.
However, a re-laparotomy first could permit a hemodynamic
stabilization of the patient and organized safely a transfer for
a stent-placement. The importance of centralization in high
volume center [27].
This procedure has never been described in the
literature to our knowledge. We advocate an algorithm’s
management in Figure 3. In case of POH, first consideration
should be the hemodynamic status of the patient. As
reported in the literature, interventional radiology has
to be performed for stable patients. On the other hand, a
salvage surgery is needed for patients with hemodynamic
instability. We recommend, after the surgical procedure,
to secure the vascular repair with a secondary stenting by
interventional radiology. This technique could reduce the
risk of potential fatal rebleeding.
Figure 3. Algorithm’s management.
CONCLUSION
Sometimes POH require prompt reintervention.
However, ligature in adverse local condition could explain
that re-bleeding is not rare notably if the pancreatic
anastomosis/remnant is preserved. IR following POH was
a safe procedure and might decrease re-bleeding rate after
reintervention. However, this attitude had to be discussed
case by case to not induce IR-direct related morbidity.
We needed more patients undergoing this original
sequence to determine if it’s strongly impact re-bleeding rate.
Conflict of Interest
Authors declare no conflict of interests for this article.
References
- Puppala S, Patel J, McPherson S, Nicholson A, Kessel D. Hemorrhagic
complications after Whipple surgery: imaging and radiologic intervention.
AJR Am J Roentgenol 2011; 196:192–197. [PMID: 21178067]
- Grobmyer SR, Kooby DA, Hochwald SN, Blumgart LH. Blumgart
anastomosis for pancreaticojejunostomy minimizes severe complications
after pancreatic head resection. Br J Surg 2009; 96:741–750.
[PMID: 20013921]
- Beyer L1, Bonmardion R, Marciano S, Hartung O, Ramis O, Chabert L,
Léone M, et al. Results of non-operative therapy for delayed hemorrhage
after pancreaticoduodenectomy. J Gastrointest Surg 2009; 13:922–928.
[PMID: 19224299]
- de Castro SM, Kuhlmann KF, Busch OR, van Delden OM, Laméris
JS, van Gulik TM, Obertop H, et al. Delayed massive hemorrhage after
pancreatic and biliary surgery: embolization or surgery? Ann Surg 2005;
241:85–91. [PMID: 15621995]
- Blanc T, Cortes A, Goere D, Sibert A, Pessaux P, Belghiti J, Sauvanet A,
et al. Hemorrhage after pancreaticoduodenectomy: when is surgery still
indicated? Am J Surg 2007; 194:3–9. [PMID: 17560900]
- Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki
JR, et al. Postpancreatectomy hemorrhage (PPH): an International Study
Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007; 142:20–25. [PMID: 17629996]
- Choi SH, Moon HJ, Heo JS, Joh JW, Kim YI. Delayed hemorrhage
after pancreaticoduodenectomy. J Am Coll Surg 2004; 199:186–191.
[PMID: 15275871]
- Farley DR, Schwall G, Trede M. Completion pancreatectomy for
surgical complications after pancreaticoduodenectomy. Br J Surg 1996;
83:176–179. [PMID: 8689156]
- Sato N, Yamaguchi K, Shimizu S, Morisaki T, Yokohata K, Chijiiwa
K, Tanaka M. Coil embolization of bleeding visceral pseudoaneurysms
following pancreatectomy: the importance of early angiography. Arch
Surg 1998; 133:1099–1102. [PMID: 9790208]
- Jilesen AP, Tol JA, Busch OR, van Delden OM, van Gulik TM, Nieveen
van Dijkum EJ, Gouma DJ. Emergency management in patients with late
hemorrhage after pancreatoduodenectomy for a periampullary tumor.
World J Surg 2014; 38:2438–2447. [PMID: 24791669]
- Tol JA, Busch OR, van Delden OM, van Lienden KP, van Gulik TM,
Gouma DJ. Shifting role of operative and nonoperative interventions
in managing complications after pancreatoduodenectomy: what
is the preferred intervention? Surgery 2014; 156:622–631.
[PMID: 25017138]
- Mañas-Gómez MJ, Rodríguez-Revuelto R, Balsells-Valls J, Olsina-Kissler JJ, Caralt-Barba M, Pérez-Lafuente M, Charco-Torra R. Post-pancreaticoduodenectomy
hemorrhage. Incidence, diagnosis, and
treatment. World J Surg 2011; 35:2543–2548. [PMID: 21882027]
- Rajarathinam G, Kannan DG, Vimalraj V, Amudhan A, Rajendran
S, Jyotibasu D, Balachandar TG,et al. Post pancreaticoduodenectomy
haemorrhage: outcome prediction based on new ISGPS Clinical severity
grading. HPB 2008; 10:363–370. [PMID: 18982153]
- Büchler MW, Wagner M, Schmied BM, Uhl W, Friess H, Z'graggen
K. Changes in morbidity after pancreatic resection: toward the end of
completion pancreatectomy. Arch Surg 2003; 138:1310–1314; discussion
1315. [PMID: 14662530]
- Yoshida T, Matsumoto T, Morii Y, Aramaki M, Bandoh T, Kawano
K, Kitano S. Delayed massive intraperitoneal hemorrhage after
pancreatoduodenectomy. Int Surg 1998; 83:131–135. [PMID: 9851330]
- Ding X, Zhu J, Zhu M, Li C, Jian W, Jiang J, Wang Z, et al. Therapeutic
management of hemorrhage from visceral artery pseudoaneurysms
after pancreatic surgery. J Gastrointest Surg 2011; 15:1417–1425.
[PMID: 21584822]
- Boufi M, Hashemi AA, Azghari A, Hartung O, Ramis O, Moutardier V, Alimi
YS. Endovascular management of severe bleeding after major abdominal
surgery. Ann Vasc Surg 2013; 27:1098–1104. [PMID: 23790760]
- Wang MQ, Liu FY, Duan F, Wang ZJ, Song P, Fan QS. Stent-grafts
placement for treatment of massive hemorrhage from ruptured hepatic
artery after pancreaticoduodenectomy. World J Gastroenterol WJG 2010;
16:3716–3722. [PMID: 20677346]
- Pottier E, Ronot M, Gaujoux S, Cesaretti M, Barbier L, Sauvanet A,
Vilgrain V. Endovascular management of delayed post-pancreatectomy
haemorrhage. Eur Radiol 2016; 26:3456–3465. [PMID: 26815369]
- Paye F, Lupinacci RM, Kraemer A, Lescot T, Chafaï N, Tiret E,
Balladur P. Surgical treatment of severe pancreatic fistula after
pancreaticoduodenectomy by wirsungostomy and repeat pancreaticojejunal
anastomosis Am J Surg 2013; 206:194–201. [PMID: 23706258]
- Ribero D, Amisano M, Zimmitti G, Giraldi F, Ferrero A, Capussotti L.
External tube pancreatostomy reduces the risk of mortality associated
with completion pancreatectomy for symptomatic fistulas complicating
pancreaticoduodenectomy. J Gastrointest Surg 2013; 17:332–338.
[PMID: 23207684]
- Turrini O, Moutardier V, Guiramand J, Lelong B, Bories E, Sannini A,
Magnin V, et al. Hemorrhage after duodenopancreatectomy: impact of
neoadjuvant radiochemotherapy and experience with sentinel bleeding.
World J Surg 2005; 29:212–216. [PMID: 15654661]
- Camerlo A, Turrini O, Marciano S, Sarran A, Berdah S,
Delpero JR, Moutardier V. Delayed arterial hemorrhage after
pancreaticoduodenectomy: is conservation of hepatic arterial flow vital?
Pancreas 2010; 39:260–262. [PMID: 20182313]
- Yekebas EF, Wolfram L, Cataldegirmen G, Habermann CR, Bogoevski
D, Koenig AM, Kaifi J, et al. Postpancreatectomy hemorrhage: diagnosis
and treatment: an analysis in 1669 consecutive pancreatic resections.
Ann Surg 2007; 246:269–280. [PMID: 17667506]
- Fujii Y, Shimada H, Endo I, Yoshida K, Matsuo K, Takeda K, Ueda M,
et al. Management of massive arterial hemorrhage after pancreatobiliary
surgery: does embolotherapy contribute to successful outcome? J
Gastrointest Surg 2007; 11:432–438. [PMID: 17436126]
- Baker TA, Aaron JM, Borge M, Pierce K, Shoup M, Aranha GV. Role
of interventional radiology in the management of complications after
pancreaticoduodenectomy. Am J Surg 2008; 195:386–390; discussion
390. [PMID: 18308043]
- Enomoto LM, Gusani NJ, Dillon PW, Hollenbeak CS. Impact of
surgeon and hospital volume on mortality, length of stay, and cost of
pancreaticoduodenectomy. J Gastrointest Surg 2014; 18:690–700.
[PMID: 24297652]




