Muhammad Wasif Saif1, Kristin Kaley2, Marianne Brennan2, Marie Carmel Garcon3, Gladys Rodriguez3 and Teresa Rodriguez3
1Section of GI Cancers and Experimental Therapeutics, Tufts University School of Medicine.
Boston, MA, USA. 2Yale School of Medicine. New Haven, CT, USA.
3Columbia University Medical Center. New York, NY, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Section of GI Cancers and Experimental Therapeutics; Tufts
University School of Medicine; 800 Washington Street; Boston,
MA 02111; USA
Phone: +1-617.636.5627
Fax: +1-617.636.8535
E-mail: wsaif@tuftsmedicalcenter.org
Received May 13th, 2013 – Accepted August 2nd, 2013
Keywords
Neuroendocrine tumors; pancreatic cancer; capecitabine; temozolomide
Abbreviations
CAPTEM: capecitabine and temozolomide; RECIST: Response Evaluation Criteria in Solid Tumors Correspondence Muhammad Wasif Saif
INTRODUCTION
Pancreatic neuroendocrine tumors (pNETs) account for 3 to 5% of pancreatic malignancies with an incidence of around 1,000 cases per year in the United States [1]. However, the incidence of these tumors seems to be rising, partly due to earlier detection of asymptomatic lesions [2]. They represent a heterogeneous group of tumors with varying biology and clinical behavior based in their functionality and differentiation. Most of these tumors are sporadic although a link with hereditary syndromes including MEN1, von Hippel-Lindau (VHL), neurofibromatosis type1 and tuberous sclerosis deserves mention as they reveal the underlying carcinogenesis [3].
The neuroendocrine tumors are classified by WHO (Table 1) based on their differentiation in order to assess their biological behavior and their potential for a malignant phenotype.

The well differentiated pNETs can be further classified based on their functionality and are divided into functioning and non-functioning tumors. The functioning tumors include insulinomas, gastrinomas, glucagonomas, VIPomas and somatostatinomas. The non-functioning tumors are more frequent and account for almost 60% of these tumors.
Unresectable pNETs have a poor prognosis with a median survival of 24 months with distant metastatic disease [2]. pNETs are notoriously resistant to currently available chemotherapy agents [4]. Streptozocin based regimens, including streptozocin-doxorubicin and streptozocin-5-FU, have shown efficacy in the past but come with the burden of toxicity and cumbersome regimens [5]. Recently, the oral alkylating agent temozolomide has emerged as a promising agent in this setting. A phase II trial consisting of the combination of temozolomide and thalidomide demonstrated an objective response rate of 45% in pNETs versus only 7% in metastatic carcinoid tumors [5]. Another study combined temozolomide with bevacizumab yielded a response rate of 24% [6]. In vitro studies have suggested a synergistic activity with the combination of capecitabine, an oral form of 5-FU, with temozolomide [7]. The data also suggests that the synergy is dependent on the sequence of how the drugs are administered. It requires that temozolomide be administered after exposure of neuroendocrine tumor cells to capecitabine. Investigators believe that this synergy is due to depletion of the DNA repair enzyme, methylguanine DNA methyltransferase (MGMT) by capecitabine, thereby potentiating the effect of temozolomide [8]. These in vitro data have been supported by clinical reports that demonstrated high objective response rates with CAPTEM in patients with metastatic neuroendocrine tumor [9, 10].
Inspired by these data, CAPTEM regimen has been explored in metastatic neuroendocrine tumor patients. We here report a retrospective data on seven patients with metastatic low- and intermediate-grade pNETs, who were treated with a modified regimen as detailed below.
PATIENTS AND METHODS
We conducted a retrospective chart review of patients with advanced neuroendocrine tumors. We selected patients with metastatic pNET who had progressive cancer prior to treatment despite therapy, including long-acting release octreotide (60 mg/month; Sandostatin LARTM, Novartis Pharmaceuticals Co., East Hanover, NJ, USA). We identified 7 patients who were treated with the CAPTEM regimen between 2006 and 2013. Pharmacy database was done to indicate patients for who were treated with CAPTEM for PTENs during this period. Review of electronic charts was performed. The data including age, sex, diagnoses, dose of CAPTEM, and CT scan results were collected. Patients received capecitabine at a flat dose of 1,000 mg orally twice daily on days 1-14 and temozolomide 200 mg/m2 in two divided daily doses on days 10-14 of a 28-day cycle (Figure 1). Ondansetron 8 mg was prescribed before each dose of temozolomide. Doses were adjusted to minimize the number of tablets required.
Figure 1. Schema of CAPTEM regimen.
Imaging was performed every two cycles, and serum tumor markers were measured every cycle. Response to treatment was assessed using Response Evaluation Criteria in Solid Tumors (RECIST) parameters [11], and toxicity was graded using the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), version 3.0 [12]. Progression-free survival was defined as time from initiation of treatment until disease progression or death. Overall survival was defined as time from initiation of treatment until death or last known follow-up.
RESULTS
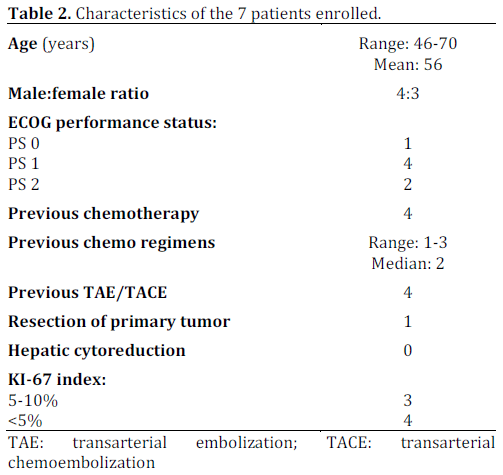
We identified 7 patients (4 males and 3 females) with metastatic pNET (low- and intermediategrade) who were treated with CAPTEM (Table 2). The time from diagnosis until onset of treatment with CAPTEM ranged between 1 year and 3.5 years. All patients had evidence of disease progression before initiation of treatment with CAPTEM. The chemotherapeutic agents previously used included doxorubicin, streptozocin, cisplatin and gemcitabine.
This CAPTEM regimen was generally well tolerated. Grade 3 and 4 toxicities included only grade 3 thrombocytopenia in one patient and grade 3 fatigue in one patient. The most common toxicities were grade 1 and 2 neutropenia, grade 1 fatigue, grade 1 and 2 hand-foot syndrome. There were no grade 4 toxicities, hospitalizations, opportunistic infections or deaths. Two patients required dose reductions because of grade 2 hand-foot syndrome.
Using RECIST parameters, three patients achieved a partial response, and 2 patients had stable disease. Total response rate was 43%, and clinical benefit (responders and stable disease) was 71%. Median duration of response was 8 months (range: 4-12 months). Median progression-free survival was 12 months (range: 10-16 months). Median overall survival was 24 months, with three patients still living.
DISCUSSION
The only potential cure for localized pNET is surgical resection. Until recently, the only standard option for advanced disease was a somatostatin analogue, most commonly used in only functional tumors to control symptoms associated with the carcinoid syndrome. It was the PROMID study, a prospective, randomized placebo-controlled study which demonstrated a median time to tumor progression of 14.3 months in the long-acting release (LAR) octreotide group versus 6 months with the placebo group [13]. The overall survival benefit was limited by crossover of patients in the placebo group to octreotide LAR at tumor progression. As expected, octreotide LAR did not produce significant tumor regression. More recently, two new drugs, everolimus and sunitinib, were approved by FDA for the treatment of advanced pNETs [14]. Everolimus, a mammalian target of rapamycin (mTOR) inhibitor, improved progression-free survival when compared to placebo: median 11.4 months versus 5.4 months, respectively. Analysis of secondary endpoints showed a response rate by RECIST criteria of 5% in patients who received everolimus. Sunitinib, a multi-tyrosine kinase inhibitor, demonstrated an improved progression-free survival when compared to placebo: median 11.4 months versus 5.5 months, respectively [15]. In addition, there was a 9.3% tumor response rate in patients treated with sunitinib [16].
Our unique dosing of CAPTEM resulted in a well tolerated oral regimen with a good safety profile in this retrospective review. Though the number of patients is small, it triggers interest for future studies. The toxicity profile is also superior to chemotherapy regimens, in particular those observed with streptozocin-based regimens. Future prospective trials should assess temozolomide monotherapy versus CAPTEM to test the hypothesized synergy between these two agents. In addition, a randomized study comparing temozolomide versus streptozocin-based regimens should be considered too in order to establish a standard of care for this disease. We also suggest that CAPTEM offers a viable option with potential for a high rate of response in a neoadjuvant therapy for locally advanced, unresectable pNETs.
Conflict of interest
The authors have no potential conflict of interest
References
- Dimou AT, Syrigos KN and Saif MW. Neuroendocrine tumors of the pancreas: what's new. Highlights from the "2010 ASCO Gastrointestinal Cancers Symposium". Orlando, FL, USA. January 22-24, 2010. JOP. J Pancreas (Online) 2010; 11:135-8. [PMID 20208321]
- Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, et al. One hundred years after "carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008; 26:3063-72. [PMID 18565894]
- Stevenson R, Libutti SK, Saif MW. Novel agents in gastroenteropancreatic neuroendocrine tumors. JOP. J Pancreas (Online) 2013; 14:152-4. [PMID 23474560]
- Oberstein PE, Remotti H, Saif MW, Libutti SK. Pancreatic neuroendocrine tumors: entering a new era. JOP. J Pancreas (Online) 2012; 13:169-73. [PMID 22406593]
- Cheng PN, Saltz LB. Failure to confirm major objective antitumor activity for streptozocin and doxorubicin in the treatment of patients with advanced islet cell carcinoma. Cancer 1999; 86:944-8. [PMID 10491519]
- Kulke MH, Stuart K, Enzinger PC, Ryan DP, Clark JW, Muzikansky A, et al. Phase II study of temozolomide and thalidomide in patients with metastatic neuroendocrine tumors. J Clin Oncol 2006; 24: 401-6. [PMID 16421420]
- Kulke MH, Stuart K, Earle CC, Bhargava P, Clark JW, Enzinger PC, et al. A phase II study of temozolomide and bevacizumab in patients with advanced neuroendocrine tumors. J Clin Oncol 2006; 24(18S): Abstract 4044.
- Murakami J, Lee YJ, Kokeguchi S, Tsujigiwa H, Asaumi J, Nagatsuka H, et al. Depletion of O6-methylguanine -DNA methyltransferase by O6-benzylguanine enhances 5 -FU cytotoxicity in colon and oral cancer cell lines. Oncol Rep 2007; 17:1461-7. [PMID 17487405]
- Isacoff WH, Moss RA, Pecora AL, Fine RL. Temozolomide/ capecitabine therapy for metastatic neuroendocrine tumors of the pancreas. A retrospective review. J Clin Oncol 2006; 24(18S): Abstract 14023.
- Strosberg JR, Fine RL, Choi J, Nasir A, Coppola D, Chen DT, et al. First-line chemotherapy with capecitabine and temozolomide in patients with metastatic pancreatic endocrine carcinomas. Cancer 2011; 117:268-75. [PMID 20824724]
- Julka PK, Doval DC, Gupta S, Rath GK. Response assessment in solid tumours: a comparison of WHO, SWOG and RECIST guidelines. Br J Radiol 2008; 81:444-9. [PMID 18316345]
- Cancer Therapy Evaluation Program. Common Terminology Criteria for Adverse Events (CTCAE) v4.0. National Cancer Institute at the National Institute of Health: Bethesda, MD, USA.
- Rinke A, Müller HH, Schade-Brittinger C, Klose KJ, Barth P, Wied M, et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin Oncol 2009; 27:4656-63. [PMID 19704057]
- Oberstein PE and Saif MW. Safety and efficacy of everolimus in adult patients with neuroendocrine tumors. Clin Med Insights Oncol 2012; 6:41-51. [PMID 22253554]
- Yao JC, Shah MH, Ito T, Bohas CL, Wolin EM, Van Cutsem E, et al. Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med 2011; 364:514-23. [PMID 21306238]
- Raymond E, Dahan L, Raoul JL, Bang YJ, Borbath I, Lombard-Bohas C, et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med 2011; 364:501-13. [PMID 21306237]


