Neha Varun1*and Renu Tanwar2
1Department of Obstetrics and Gynaecology, Hakeem Abdul Hameed Centenary Hospital and Hamdard Institute of Medical Sciences and Research, New Delhi, India
2Department of Obstetrics and Gynaecology, Lok Nayak Hospital and Maulana Azad Medical College, New Delhi, India
*Corresponding Author:
Varun N, Assistant Professor
Department of Obstetrics and Gynaecology
Hakeem Abdul Hameed Centenary Hospital
and Hamdard Institute of Medical Sciences and Research,
Tel: 9968604352
E-mail: drneha.ucms@gmail.com
Received date: February 22, 2017; Accepted date: March 20, 2017; Published date: March 23, 2017
Citation: Varun N, Tanwar R. A Rare Presentation of Endometriosis with Massive Haemorrhagic Ascites: A Case Report. Gynecol Obstet Case Rep 2017, 3:1. doi:10.21767/2471-8165.1000047
Keywords
Endometriosis; Haemorrhagic ascites
Introduction
Endometriosis is commonly found in approximately 10% to 15% of women between 25 to 44 years of age group and in infertile women incidence of endometriosis is almost 25% to 40% [1]. In this case report, we are presenting a patient with endometriosis presented with massive hemorrhagic ascites. Endometriosis is a gynaecological condition in which cells of the endometrium appears and develops outside the uterine cavity, most commonly on the peritoneum lining the abdominal cavity. The ectopic tissues of endometrium grow each month and causes bleeding. Unlike the lining of the uterus, ectopic endometrial tissues have no way of leaving the body and as a result moderate to severe internal bleeding occurs and leads to massive hemoperitoneum. Endometriosis associated with the massive haemorrhagic ascites is a very rare presentation and only few cases have been reported yet. Differential diagnosis of women with haemorrhagic ascites includes rupture of hemorrhagic ovarian cyst, spontaneous rupture of spleen, ovarian cancer, hepatoma, tuberculosis, endometriosis, ectopic pregnancy, Meigs syndrome and other haemorrhagic intraabdominal processes [2]. Other less frequent causes include mesothelioma, Budd Chiari syndrome, perforated duodenal ulcer, primary splenic lymphoma, mesenteric cyst, multiple myeloma, and cirrhosis. Endometriosis is an exceptionally rare cause of haemorrhagic ascites.
Case Presentation
Twenty-six-year-old nulliparous female attended gynaecology OPD with the chief complaints of abdominal distension since three months associated with the lower abdominal pain. Pain was gradual in onset, continuous in nature and not relieved with the medications. Bowel movements were normal and there was no history of nausea, vomiting, hematemesis and melena. She had no history of coagulation disorders and platelet dysfunction. She was admitted in some private hospital before she reported here, there she has received one unit blood and underwent extensive evaluation for abdominal distension. Her menarche was at 13 years of age. She had a regular normal flow with no history of dysmennorhoea or dyspareunia. She is a nulliparous female married for 1 year. Past and family history of patient was insignificant.
On examination, she was found to be well-nourished, anicteric, afebrile but had pale conjunctiva and buccal mucosa. Vitals were stable. On abdominal examination, free fluid was present and there was generalised tenderness and shifting dullness. On speculum examination, no abnormality detected. Uterus was midposition, normal in size, firm, mobile on prevaginal examination with fullness in the fornices and POD and no mass felt in the fornices. Haematological parameters including complete blood count and coagulation profile were within normal limit. Peripheral smear showed normocytic normochromic anaemia and no evidence of haemolysis. CA-125 was 36.30 U/ml and rests of the tumor markers were negative. D-Dimer, FDP and serum fibrinogen level were within normal limit.
On ultrasound examination, massive ascites was present with low level internal echoes, uterus was normal size, and in right adnexa 5.2 × 5.3 cm cystic lesion with mixed septations and peripheral vascularity was present and right ovary was not seen separately. Left ovary was bulky in size. Ultrasound upper abdomen was within normal limits.
Contrast enhanced computed tomography of whole abdomen showed an ill-defined heterogenously enhancing multiloculated solid cystic mass lesion measuring 4.5 × 5.5 cm in the right adnexa. The lesion was having papillary excrescences and showed enhancing solid component and irregular enhancing internal septa within. Left ovary was bulky. Gross ascites was present causing scalloping of liver margins. Findings were suggestive of mucinous cystic neoplasm of bilateral ovary with pseudomyxoma peritonei. Upper and lower gastrointestinal endoscopies were within normal limit.
Endometrial biopsy showed proliferative endometrium on histopathological examination and TB PCR was negative. Ascitic fluid tap showed grossly haemorrhagic fluid. Ascitic fluid gram stain, TB PCR and AFB were negative. Ascitic fluid biochemistry was within normal limit and adenosine deaminase was 38 μ/L (increased). No malignant cells were found. Presumptive diagnosis of ovarian tumor was made on the basis of history, examination and investigations. Exploratory laparotomy was planned.
In per-operative findings three litres of hemoperitoneum was drained and sent for cytology. Uterus and bilateral tubes were normal looking. B/L ovaries were enlarged with the cyst of approximately 5 × 4 cm in the right ovary containing chocolate colour fluid with thin septations. Right ovarian cystectomy was done and cyst wall was sent for histopathological examination. Left ovary was bulky. There were no endometriotic spots over the peritoneum. Omental and peritoneal biopsies were taken. Bowel was normal looking. Adhesions were present in the pouch of Douglas between posterior surface of the uterus and bowel.
Fluid cytology reported only blood and no atypical cells were found. Omental biopsy showed fibroadipose tissues with focal mild chronic inflammation, right ovarian biopsy showed ovarian tissue with evidence of endometriosis (Figure 1) and peritoneal biopsy showed fibrovascular tissues with areas of haemorrhage and findings suggestive of endometriosis (Figure 2).
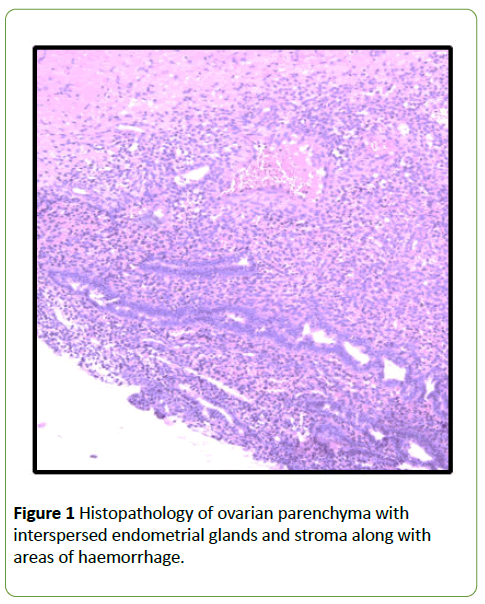
Figure 1:Histopathology of ovarian parenchyma with interspersed endometrial glands and stroma along with areas of haemorrhage.
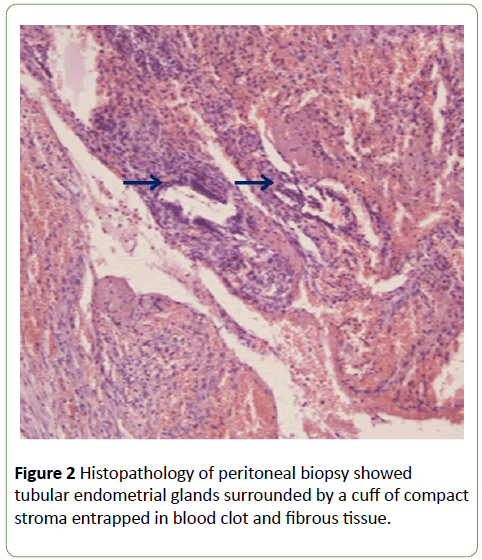
Figure 2:Histopathology of peritoneal biopsy showed tubular endometrial glands surrounded by a cuff of compact stroma entrapped in blood clot and fibrous tissue.
Post-operative period was uneventful. On repeat USG examination on POD-6 of laprotomy minimal free fluid was present in the abdomen. Injection leupride was given on POD-8 followed by two more doses of injection leupride at an interval of 28 days. Patient is under follow up.
Discussion
An estimated 10% to 15% of woman of child bearing age group have endometriosis. Presentation of endometriosis varies and it may present as infertility, dysmenorrhoea, chronic pelvic pain, deep dyspareunia or bleeding at external sites like the umbilicus [2]. Endometriosis presenting as a recurrent haemorrhagic ascites is an unusual occurrence, more than 60 cases have been reported since 1954 [3,4], and these patients are usually noncritical with minimal significant complications [5,6]. Predominant theories regarding the pathophysiology of haemorrhagic ascites includes peritoneal irritation from ruptured endometriotic implants, sub diaphragmatic obstruction of lymphatics and retrograde menstruation [7]. Here we are reporting an additional case, in order to draw attention towards this rare condition. Diagnosis of endometriosis requires that the clinician should differentiate it from neoplastic or other inflammatory conditions [8]. In general, asymptomatic lesions of endometriosis which are found incidentally at laparotomy done for other conditions require no treatment. Hemorrhagic ascites is characterized by bloody appearance of ascitic fluid and is defined as a ascitic fluid with an erythrocyte count of more than 50,000/ μL.
Hemorrhagic ascites should be considered a complication of endometriosis, especially in nulliparous women of childbearing age group with an abdominal distention, a pelvic mass, dysmenorrhea, abdominal pain, weight loss and eventual pleural effusion, suggesting a diagnosis of ovarian malignancy [9]. Similar to this patient, a recent review and analysis of previous cases found that 63% of women were of African ancestry, and 82% were nulliparous [8]. 38% of patients previously described in the literature also had a pleural effusion [5]. Although massive ascites has been reported as a manifestation of endometriosis, but it can be seen in patients with acute abdomen with shock also [10]. Other known causes of bloody ascites, especially a malignant process, must be excluded. In addition to endometriosis involving various gastrointestinal organs, other findings such as adhesions and fibrosis are frequently encountered at laparotomy [11]. The diagnosis must be confirmed histologically. Recurrences have been seen commonly with severe complications and usually required multiple laparotomies and thoracotomies for associated pulmonary involvement [12].
Definitive management consists of surgical resection of endometriotic tissue combined with the complete surgery or long term hormonal suppression therapy [13]. Long-term hormonal suppression therapy is generally reserved for young nulliparous patients because it usually obviates the need for complete surgery and it can preserve fertility in some cases. The response of hormonal therapy including GnRH agonists in patients of endometriosis with ascites is often unsatisfactory according to the case studies. Oral contraceptive pills or leuprolide injection used for long term management reduces the amount of follicle stimulating hormone and luteinizing hormone, results in hypoestrogenism suppressing the growth of native and ectopic endometrial tissues. Ruptured ectopic pregnancy is the most common gynecological cause of hemoperitoneum in a reproductive-age woman, endometriosis should also be considered as a cause, especially after excluding pregnancy [14]. Long term follow-up is advised to the patients who underwent conservative treatment because of the high risk of recurrence of disease.
Conclusion
Presentation of endometriosis varies and it can present with significant internal bleeding. Endometriosis should be considered in the differential diagnosis when bloody ascites and a pelvic mass are present, particularly in young female patients, for which there is no obvious explanation. A very high level of clinical suspicion is required if the diagnosis of severe endometriosis is not to be missed. The surgeon should therefore be very vigilant and alert to localize and diagnose rare sites of internal bleeding due to endometriosis.
References
- Talbert LM, Kauma SM. Endometriosis (1990) In: Danforth DN, ScottJR(Eds). Danforth's obstetrics and gynecology. (5thedn), Philadelphia: JB Lippincott.
- Otolorin EO, Ojengbede O, Falase AO (19987) Laparoscopic evaluation of the tubo-peritoneal factor in infertile Nigerian women. Int J Gynecol Obstet 25:47-52.
- Trent LM, Eric BT, Jason DH (2013) Endometriosis presenting with hemorrhagic ascites,severe anaemia, and shock: Case report. AmJ Emerg Med 31: e1272-e3 272.
- Ekoukou D, Guilherme R, Desligneres S, Rotten D (2005) Endometriosis with massive hemorrhagic ascites: A case report and review of the literature. J Gynecol Obstet Biol Reprod(Paris) 34:351-359.
- Ussia A, Betsas G, Corona R, De Cicco C, Koninckx PR (2008) Pathophysiology of cyclic hemorrhagic ascites and endometriosis. J Minim Invasive Gynecol 15:677-681.
- Gungor T, Kanat-Pektas M, Ozat M, ZayifogluKaraca M (2011) A systematic review: Endometriosis presenting with ascites. Arch Gynecol Obstet 283:513-518.
- Palayekar M, Jenci J, Carlson Jr JA (2007) Recurrent hemorrhagic ascites: A rare presentation of endometriosis. Obstet Gynecol 110:521-522
- Mejia EM, Alvarez OA, Lee M (1997) Endometriosis with massive bloody ascites. JABFP 10:1.
- Dias CC, Andrade JM, Ferriani RA, Villanova MG, Meirelles RS (2000) Hemorrhagic ascites associated with endometriosis: A case report. J Reprod Med 45:688-690.
- Lin JN, Lin HL, Huang CK, Lai CH, Chung HC, et al. (2010) Endometriosis presenting as bloody ascites and shock. J Emerg Med 38:30-32.
- Jenks JE, Artman LE, Hoskins V, Miremadi AK (1984) Endometriosis with ascites. Obstet Gynecol 63:755-77S.
- Muneyyirci-Delale O, Neil G, Serur E, Gordon D, Maiman M, et al. (1998) Endometriosis with massive ascites. Gynecol Oncol 69:42-46.
- el-Newihi HM, Antaki JP, Rajan S, Reynolds TB (1995) Large bloody ascites in association with pelvic endometriosis:Case report and literature review. Am J GastroenteroI90:632-634.
- Harmanli OH, Chatwani A, Caya JG (1998) Massive hemoperitoneum from endometriosis of the fallopian tube: A case report. J Reprod Med 43:716-718.

