Keywords
Quality improvement; Healthcare; Mortality
Abbreviations
MD: Medical Doctor, RN: Registered Nurse, NA: Nursing Assistant, RP: Registered Pharmaceutical, LA: Laboratory Analyst, IA: Information Analyst: Master of Science, MSc: Master of Business Administration, MBA: Posgraduate Certificate, PGCert, Posgraduate Diplomas, PGDip: Quality Improvement Model, QIM: Managed Sepsis Protocol, MSP: Multidisciplinary Work Teams, MWTs: Driver Diagrams, DDs.
Introduction
Local problem and rationale
Sepsis remains as an important public health problem all over the world, but particularly, in Brazil. Its prevalence has been increasing together with the associated high mortality rates, especially in the Intensive Care Units (ICUs) of public hospitals [1-3], despite the related international efforts to raise awareness [4-5] and the creation of initiatives to improve the performance of sepsis care programs [6-10].
Our concern was centered on the poor adherence to the Surviving Sepsis Campaign (SSC) guidelines [10] and the apparent inadequate compliance with the directives of its threeand six-hour care-bundles by health professionals from Brazilian public hospitals described in previous studies. These failures led to delays in the onset of correct diagnosis and management and contributed to augment mortality [11]. Adequate adherence to SSC guidelines results in significant reduction of mortality rates [12-14].
The Municipal Hospital of Vila Santa Catarina (HMVSC) is a general and tertiary referral center, located in the southern region of São Paulo city, capital of the São Paulo State in Brazil, and recently established through a public-private partnership. In activity since June 2015, its forecast is for 14,000 admissions per year; the available inpatient services are: general surgery, internal medicine (including adult ICUs), obstetrics (including an Obstetric Emergency Room), pediatrics (including pediatric and neonatal ICUs), oncology and transplantation (including outpatient).
A specific recognition system of septic patients, which would facilitate the triggering of a coordinated, gradual and rapid response, was needed in face of the characteristics of the HMVSC. Our research group believed that its recent inauguration and recently hired personnel would be a suitable ground to implement the SSC guidelines. In addition, the personnel and the economic and structural resources of HMVSC are those common to other institutions of the Brazilian Unified Health System (SUS).
The present article reports our experience with the QIM in the implantation of a MSP in the public hospital HMVSC over an eighteen months period.
Background
There are no consistent data on the incidence of sepsis in Latin American ICUs [1]. In Brazil a few reviews report an incidence of 57 cases per 1000 patients and it continues to increase [3,11].
According to the Latin American Sepsis Institute (LASI) data that were obtained from a total of 230 ICUs, the mean mortality due to sepsis was 55% [3]. Mortality has been increasing because of several factors such as: longer time between suspected dysfunction and diagnosis, lower adherence to the guidelines of early and proper blood sampling for cultures and lactate levels, lower frequency of diagnosed patients in the first hour after admission, higher score in the "Sequential Multiorganic Failure Assessment" (SOFA) at the time of diagnosis, greater number of organ dysfunctions [3,12], hospital infection acquired in the ICU itself, delayed administration of antibiotics and general lack of resources [3,13].
Studies in the area of quality improvement in sepsis suggest that the implementation of SSC care bundles in different hospital contexts has had different degrees of success [14-16]. Successful programs are largely based on the use of approaches that describe, develop and evaluate specific interventions that have a real, direct and sustainable effect on the care of sepsis patients. The strategies aim to change the prevalent culture and the organizational processes. Specifically they are designed to induce higher awareness in the attending personnel towards the early recognition and the rapid onset of basic care in the first 3 hours. In order to achieve this goal, efficient and effective collaboration among assistance teams involved in the initial evaluation is required.
Therefore, our research group decided to conduct a quality improvement project with emphasis on the use of strategies proposed by the IHI that should facilitate higher adherence to the SSC guidelines. The specific focus was in meeting the quality standards of the basic set of interventions, known as "resuscitation" (3h-bundle) [17], which have shown a 40-60% relative risk reduction in mortality [18-21].
Methods
Context and baseline measurement
The data were extracted from a prospective audit of hospitalized adult patients diagnosed with sepsis and septic shock between January 2016 and June 2017, including: medical records the Department of Medical and Statistical Archive Services, laboratory screening records (reported panic alerts and organ perfusion related blood tests) and the Hospital Infection Control Service (HICS) screening records (registry of patients on intravenous antibiotic use).
The patients who were considered eligible to be included in the study fulfilled the criteria The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) of 2016 [22]. Ineligible patients were those under 18 years of age, and patients in palliative care and /or patients with a medical order of non-resuscitation.
Design
This is a longitudinal, prospective, non-randomized study lasting 18 months.
It was conducted in three hospital service areas: 1) ICU, 2) inpatient areas (including internal medicine, general surgery, oncology, transplantation and obstetrics) and 3) the obstetrics emergency service.
The study is based mainly on three questions that were put forward by the scientific method popularized by the IHI: (1) what are we trying to accomplish? (2) how will we know if a change is a true improvement? (3) which changes can be made that would result in a real improvement? These issues were addressed by three main actions:
(a) establishing a clear and specific goal; (b) defining a set of outcomes, processes, and balancing measures regarding healthcare personnel opinions (c) selection of specific interventions conceived to eliminate the perceived gaps in the care of critically-ill patients [23-26].
Team and interventions
Following the directions of QIM of IHI, we created Multidisciplinary Work Teams (MWTs), capable of creating a work plan that contained a multifaceted set of strategies and interventions to improve the management of sepsis. This approach allowed the identification of the causes of inadequate sepsis management particular to the HMVSC and the problem-solving proposals.
The MWTs of quality improvement in sepsis were assigned by invitation to participate in the project made by the research group following to the hospital's senior leaderships of each area. In turn, the board indicated the medical and nursing coordinators. These identified a clinical representative of reference in the recognition, diagnosis and treatment of sepsis.
Thus, a total of 3 MWTs were formed consisting of: representatives of senior management (director), a specialist in the care of sepsis (intensive care physician), day-to-day personnel (medical coordination and nursing), front line staff (an internist, a registered nurse and a nursing technician or assistant), as well as members of the research group (specialists in quality improvement and hospital management, clinical and experimental research, and a postgraduate student in the area of health sciences).
An Ishikawa diagram was built with the identified main causes of septic shock and of the sepsis-caused hospital lethality (Figure 1).
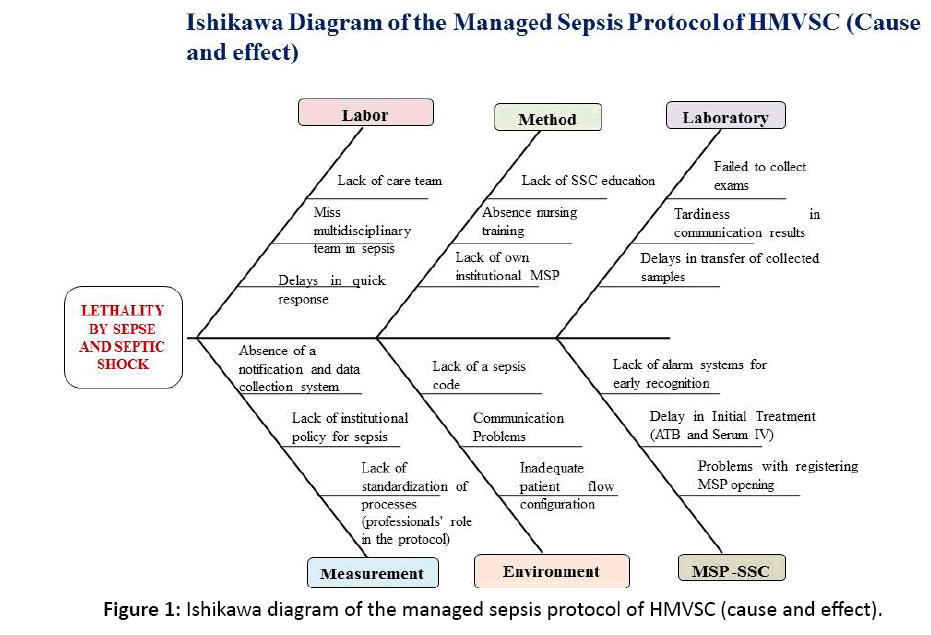
Figure 1: Ishikawa diagram of the managed sepsis protocol of HMVSC (cause and effect).
The Driver Diagrams (DDs) elaborated by the MWTs containing the key interventions that would trigger the specific actions which could result in true improvements in the care for the septic patient. The actions were conceived to be safe, rapid, focused and to be executed in a standardized manner (Figure 2).
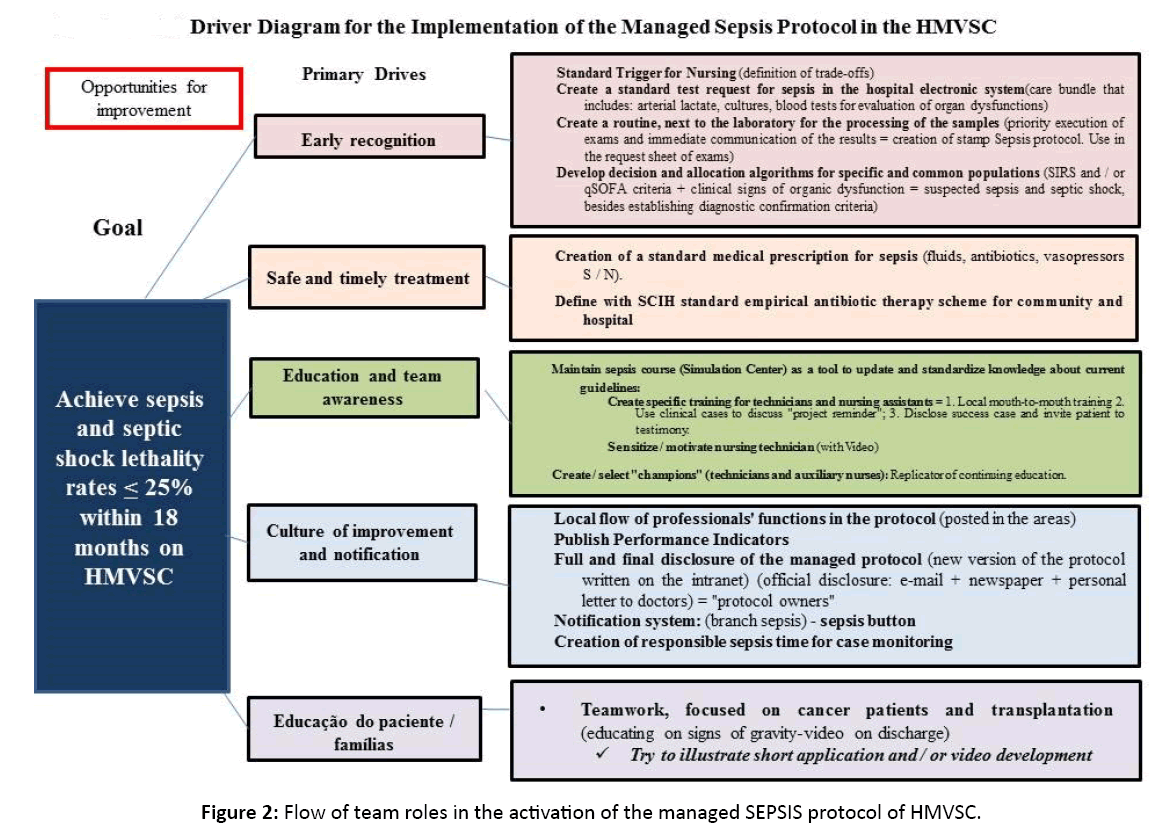
Figure 2: Flow of team roles in the activation of the managed SEPSIS protocol of HMVSC.
Study of the interventions
The interventions were carried out as follows: (1) ICU during 5 months (January-May 2016); (2) inpatient areas during 7 months (June-December 2016) and (3) emergency obstetrics service during 5 months (January- June 2017).
The data collection was monthly and continuous during the implementation of the interventions. The maintenance of these with time was also evaluated. The data as well as sepsis parameters were recorded in a database to be later analyzed by statistical methods.
Quantified parameters
The following parameters were recorded: (1) outcomes (sepsis lethality and septic shock rates ≤ 25%); (2) process (compliance rates to the 3-hour SSC care bundles) and (3) balancing measures (self-reported staff workloads among MWTs participants during the implementation and related satisfaction assessment with the MSP).
Analysis
For the qualitative data, the published reports on the use of the QIM methodology by a number of American and Great Britain Hospitals were analyzed in order to achieve a systematic approach to explain, interpret and understand the functionality and usefulness of all instruments or tools created and designed in DDs.
This manuscript was developed according to the guidelines SQUIRE V.2.0.13.
Design of the strategy
This was achieved by applying procedures based on the QIM methodology. The QIM methodology, originally used in the industry, has been also employed in hospitals and health care services. It proved to be practical and helped, in the present application of its principles, to solve problems related to the management and care of sepsis-suspected and sepsis patients. The method improved work performance, making it more organized, faster, and more timely and standardized.
The first step was to improve the early recognition of sepsis.
An early warning system for the sepsis detection (standard trigger tool for use by nursing staff) was created. This tool, called "suspected sepsis", had the function of immediately triggering the MSP (yellow code). This tool’s menu includes a mixture of the Criteria of Systemic Inflammatory Response Syndrome (SIRS) and the "quick-SOFA" Scale (qSOFA) (Figure 3).
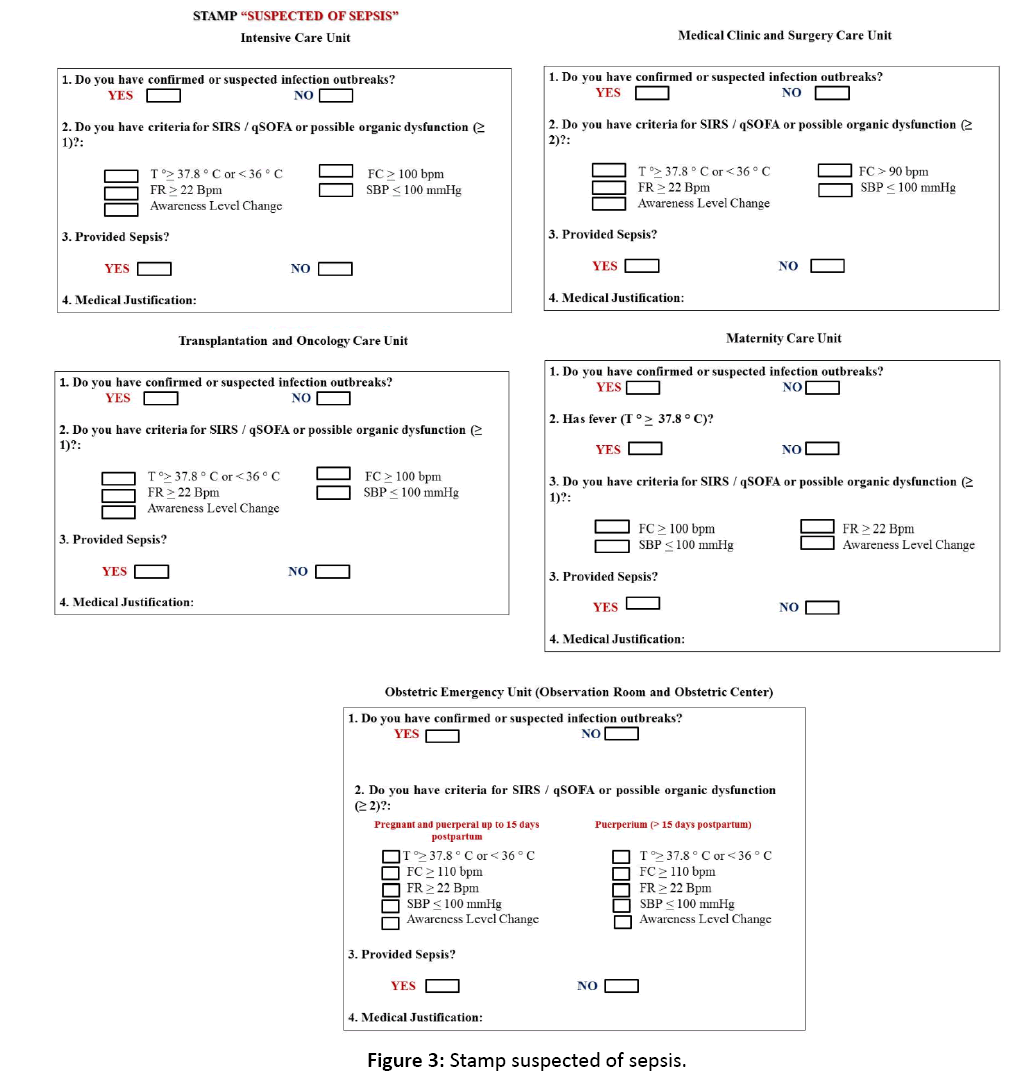
Figure 3: Stamp suspected of sepsis.
We introduced decision and allocation algorithms for the ICU septic patients (common or special groups or those with risk factors). They were based on SSC guidelines and were reproduced in poster format and displayed in all areas participant in the hospital study. Such algorithms would act as visual reminders of the procedures related to the recognition and diagnostic confirmation of sepsis–suspected patients, ideally within the first hour after the initial evaluation (Figure 4, Figure 5).
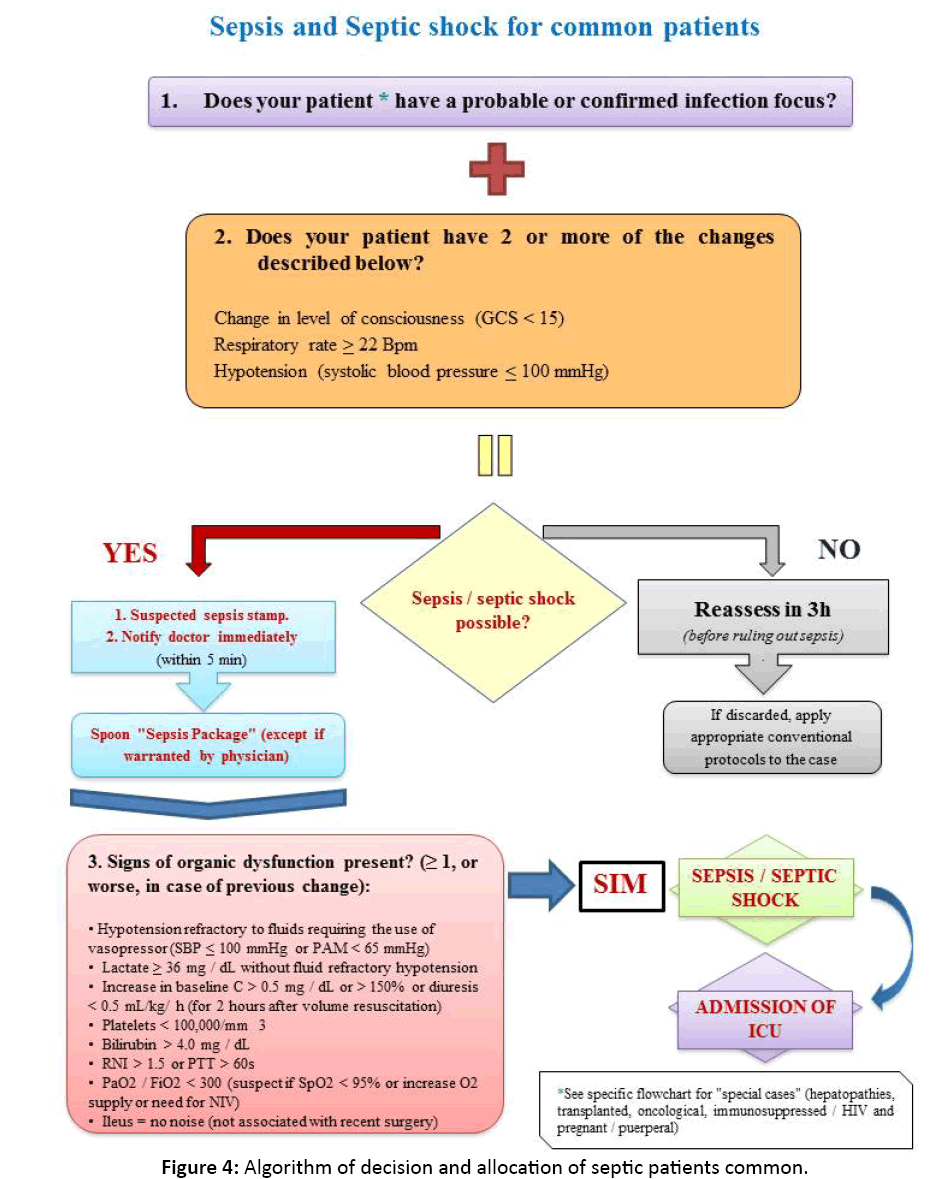
Figure 4: Algorithm of decision and allocation of septic patients common.
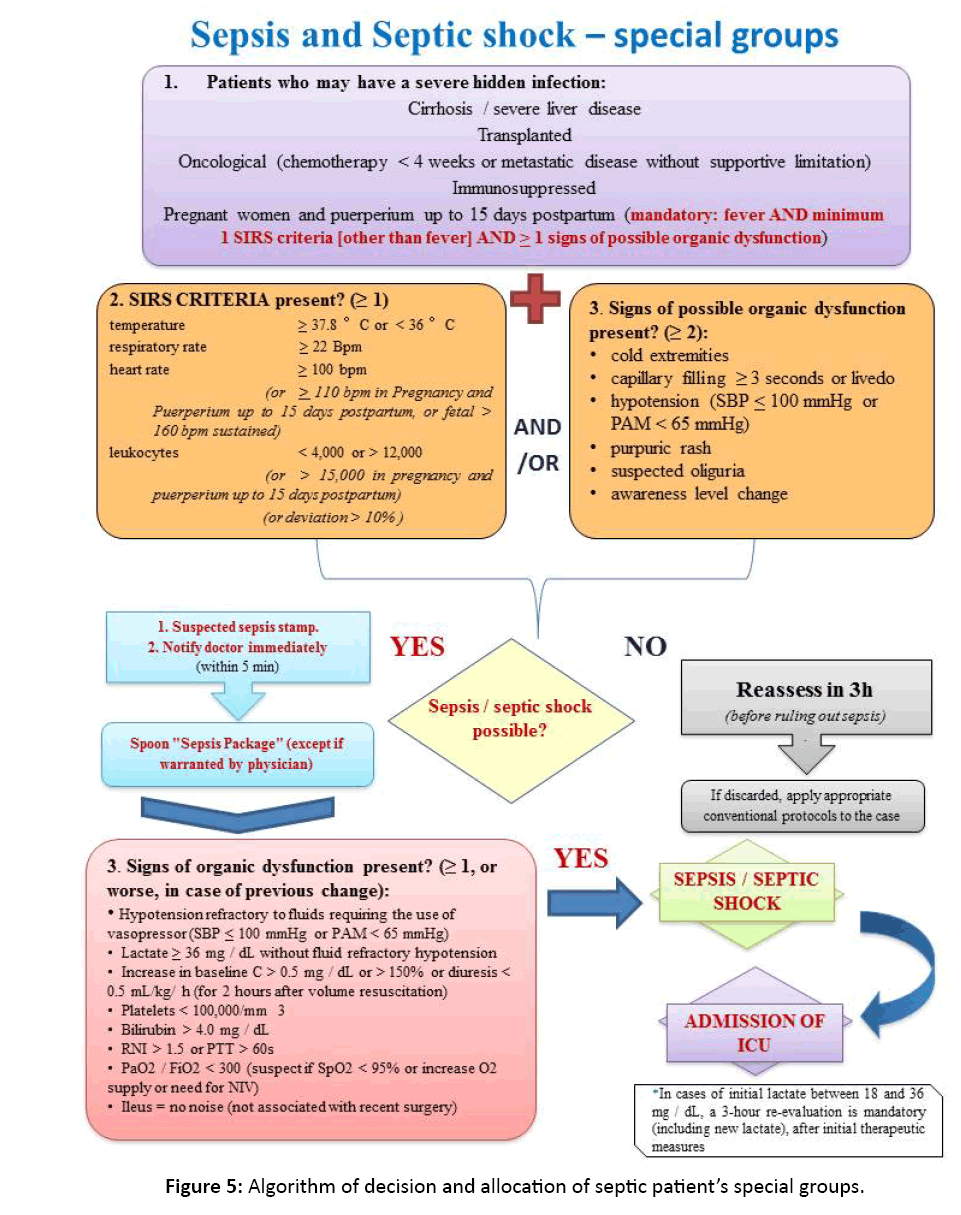
Figure 5: Algorithm of decision and allocation of septic patient’s special groups.
A set of standard tests called the HMVSC sepsis care bundle was established within the electronic Hospital Management System (HMS), which should be requested by the physician to confirm sepsis-related organ dysfunction.
For the rapid processing of the samples taken from septic patients a red stamp called "sepsis protocol" was created. This stamp signaled the laboratory that the samples should have priority in processing and sending the results.
Each sector of the hospital received standard kits for sample collection called the "sepsis collection kit".
The ICU sepsis MWT and the HICS created a Standard Medical Order Set for Sepsis to be completed by the attending medical doctor at the opening of the MSP (Supplement 1).
We contacted the pharmacy and diagnostic imaging services inform them about the study. Pharmacy coordination was committed to prioritizing the dispensing of antibiotics, serum and vasopressors. Likewise, the coordination of diagnostic imaging service established a maximum period of 2 hours for carrying out the examinations (radiology, ultrasound and computed tomography) for the identification of infectious foci.
The Wards sepsis MWTs redesigned the vital signs form giving it a new color format. This new proposed form has "color control knobs" and operates as an auxiliary alarm system, helping the technicians and nurse assistants to improve the monitoring, reinforcing the identification of high-risk patients who may progress to sepsis and, therefore, possibly avoids hours of decompensation and complications (Supplement 2).
Another proposition was to call attention of the frontline medical and nursing staff to the implications of poor management of septic patients and to the novel strategies created by sepsis MWTs. This was implemented through a series of short presentations and informal discussions of the related inpatients’ clinical cases: they were offered over a period of 1 month in each intervention area of the program.
The new MSP was also spread through letters sent by the hospital medical board to be personally delivered to all medical personnel. In addition, the hospital’s quality and safety department posted on the institutional intranet the new MSP document depicting in a flow chart each person’s task in the MSP (Supplement 3).
We chose, among the nursing personnel and technicians, leaders who were called "sepsis champions". These were in charge of spreading their acquired knowledge on early recognition of sepsis and of ensuring the routine functioning of the new MSP (good utilization of tools) so as to maintain the dynamics of our project.
An educational video was also created for patients that have risk factors for sepsis (see link: https://www.youtube.com/watch?v=uQfe6D2hFKg). This video is also shown, on the day of hospital discharge, to all patients who were hospitalized for sepsis and / or septic shock; it should facilitate the nursing home care.
Finally, a notification system was established for suspected sepsis and septic shock. This system, called the "Sepsis Key", is activated by the attending staff via telephone connection to an institutional branch.
In addition it is important to mention that the breaking of bureaucratic barriers imposed by the existing internal hospital care procedures was only possible because reports on audits of clinical cases were brought to the attention of the higher administration levels.
Ethical considerations
The present study was submitted and approved by the research ethics council of the Hospital Israelita Albert Einstein and by the Municipal Health Department of the city of São Paulo. It was a localized quality improvement project with no potential harm to patients.
Results
Cycle 1 PDSA: The meetings with each MWTs were held once a week in the first two months and every two weeks during the following months to elaborate the DDs. Once the DDs were completed, the MWT met every eight weeks to monitor the implementation process. In this first cycle, the research group tested the routine care of 3 septic patients in real time between the ICU, pharmacy, diagnostic image and laboratory. It was shown that monitoring of these cases should be increased by 50% to be fully effective. The feedback received after this initial testing process allowed us to create the cause and effect diagram of sepsis lethality in the hospital.
Cycle 2 PDSA: In order to increase the awareness towards the diagnostic criteria and initial recognition of sepsis, the team worked with the front-line staff several "suspected sepsis" drafts including the process of decision making and algorithms allocation for septic patients as well as the prescription according to the SMPS. This procedure facilitated the collection of quality indicators related to compliance with the SSC 3 and 6 hours care bundles. The team stated that these instruments achieved the objectives of fast identification and offering a quick guide for the diagnosis and treatment of sepsis-suspected patients in a safe and organized way. Such a protocol allows rational treatment of such patients and increased compliance by 70% to the SSC first 3 hours care bundle.
Cycle 3 PDSA: With the of notification system "Key Sepsis" notification of suspected cases increased by 60%.
The stamp “sepsis protocol” accelerated, from the routine 120 minutes to 30 minutes, the processing and the delivery of arterial lactate test results. The processing and the delivery of laboratory results of other organic dysfunction blood tests were ready 60 minutes after MSP start on.
The MWTs, as evaluated by semi-structured interviews of their members, reported that they did not perceive an increase in workload and expressed a good level of satisfaction with the methodology used, as they became active participants in decision-making processes.
The study's quantitative results will be available by the end of 2017.
Discussion
Interpretation
The most important aspect of this project was the possibility of implementing the SSC guidelines in a public hospital situated in a developing country. To accomplish this, the research team interacted and successfully involved all hospital staff members who directly or indirectly take care for sepsis or sepsis-suspected patients. In addition, the team had to be able to teach and, at the same time, to understand how to monitor and control in a quick, simple and effective way the required procedures to best treat these critical patients.
Certainly, there is no magic in providing correct management of sepsis in accordance to SSC guidelines. It requires an orderly effort of a dedicated and motivated multidisciplinary team in the execution of a diversity of tasks. Continuous adjustments of the protocols will be needed in order maintain the already achieved gains in the treatment of such severe medical conditions [27- 31]. According to the published experiences from other similar studies, the maintenance of projects in the area of quality improvement is a constant challenge due to the constant change and / or rotation of the care staff [13,27-29].To counteract that, a permanent Sepsis Team was created, with representatives of different areas. It will be henceforward responsible to by the protocol.
Nevertheless these 18 months allowed us to obviate obstacles and create solutions applicable to the different areas of inpatient care in the public hospital HMVSC, in a standardized, fast, effective and safe way.
Lessons
The most important learned lessons were:
• IHI QIM methodology seems to be a suitable method to implement sepsis protocols.
• Teamwork is absolutely essential to address the problems and to negotiate solutions.
• In order to achieve success at the implantation of a protocol, it is necessary to investigate the experience of other hospitals that have carried out quality improvement projects, since this offers some assurance that the project can be effectively executed and will be successful.
Understanding what really works as upgrade at each of the several steps of the new protocol and applying the PDSA cycle’s method as a refinement strategy ensures that the study remains focused towards achieving a specific goal.
Limitations
It has to be stated the large limitations of this study, starting from its descriptive and qualitative nature, performed only in one center in Brazil, and without a control group.
The report of this experience is intended to show that the IHI QIM methodology seems to be suitable, fast and robust to implement a sepsis protocol in a tertiary hospital, and should be considered by researchers, quality improvement professionals, managers or hospital policy-makers.
Long-term sustainability was not evaluated and it is one of the most important challenges for the future.
The HMVSC sepsis MWTs need to consolidate, stay alive and depend on highly motivated and dedicated medical and nursing staff. A larger flow of patients to the hospital and insufficient new hiring of needed personnel to cope with may limit the execution of some aspects of the MSP.
A larger flow of patients to the hospital and insufficient new hiring of personnel to cope with may limit the execution of some aspects of the MSP.
Conclusion
Although the conclusions are based on only qualitative data and descriptive observations, they suggest that all the assistant staff members and especially those on the front line gained the necessary knowledge on sepsis management.
Such reports indicated the malfunctioning of the existing clinical protocol and stressed the positive aspects of changing to new management protocols for sepsis.
Although these took at first some time to establish, they became incorporated synchronously to the work routine and offered real improvements for health care.
We hope that the working teams (MWTs) strengthen their leadership in order to make this quality improvement process a continuous one.
Finally, we conclude that the IHI quality-improvement model seems to be a suitable tool to implement sepsis management protocols in a tertiary hospital.
Acknowledgments
We would like to acknowledge the sepsis MWTs and their contribution to the development of this study: Guilherme de Paula Pinto Schettino, MD, PhD; Leonardo Jose Rolim Ferraz, MD, PGDip; Ana Paula Metran Nascente Pereira, MD, PhD; Rosana Mandelbaum, MD, PGDip, PGCert; Adolfo Wenjaw Liao, MD, PhD; Monica Andrade de Carvalho, MD, PGDip, MSc, MBA; Fernanda Domingos Giglio Petreche, MD, PGDip; Cristina Tiemi Amadatsu, MD, PGDip; Carolina Devite Bittante, MD, PGDip; Midgley Gonzales, MD, PhD; Gabriela Sato, RN, PGDip, MBA; Maitê Augusta C. C. Rossetto, RN, PGCert; Adriana Martins da Silva, RN, MBA; Silvana Aparecida Eleodoro dos Santos, RN; Marcia Galluci Pinter, RN, MSc; Samira Scalso de Almeida, RN, PGDip; Eliton Paulo Leite Lourenco, RN, MBA, PGDip; Maria Aparecida Machado, RN, PGDip; Priscilla Santini Ramalho, RN; Érika Brosco Lima, RN; Marcelo Longarezi Valvassora, RN, PGDip, MSc; Caroline Gusmão Alves Santos, RN, PGDip; Camila de Carvalho Gambin, RN, PGDip; Natalia Nunez de Souza, RN, PGDip; Maria Caroline de Oliveira, RN; Denise Simas Lamarão, RP, MBA; Francisco Neves Pereira, LA; Ana Paula Doria Santos, NA; Ernane Cruz da Silva, IA; and Ana Paula de Oliveira Ribeiro, IA.
Contributors
Ises de Almeida Abrahamsohn, MD, PhD, assisted in the editing and correction of the English language of the manuscript.
Funding
This study represents an independent research without public or private financing; however LKCN is supervised under a master's studentship funded by a Brazilian Ministry of Education foundation (CAPES) that is unrelated to this study.
References
- Silva E, Pedro M de A, Sogayar AC, Mohovic T, Silva CL, et al. Brazilian Sepsis Epidemiological Study (BASES study). Crit Care 2004. Aug; 8(4):R251-60.
- Conde KAP, Silva E, Silva CO, Ferreira E, Freitas FGR, et al. (2013) Differences in sepsis treatment and outcomes between public and private hospitals in Brazil: A multicenter observational study. PLoS ONE 8: e64790.
- https://www.ilas.org.br/materiais-adulto.php.
- https://www.survivingsepsis.org/Resources/Pages/Media.aspx.
- https://www.ihi.org/topics/Sepsis/Pages/default.aspx.
- https://www.england.nhs.uk/ourwork/part-rel/sepsis/.
- https://www.cdc.gov/sepsis/index.html.
- https://www.nes.scot.nhs.uk/about-us/whats-new/introducing-the-nhsscotland-
- Giuliano KK, Lecardo M, Staul LA. Impact of protocol watch on compliance with the surviving sepsis campaign. Am J Crit Care 2011; 20: 330-331.
- Berg GM, Vasquez DG, Hale LDS, Nyberg SM, Moran DA. Evaluation of process variations in noncompliance in implementation of evidence-based sepsis care. J Healthc Qual 2013; 35: 60-69.
- Siqueira-Batista R, Gomes AP, Calixto-Lima L, Vitorino RR, Perez MCA, et al. Sepsis: An update. Rev Bras Ter Intensiva 2011; 23: 207-216.
- news-and-sepsis-screening-tool-app.aspx.
- Sogayar AM, Machado FR, Rea-Neto A, Dornas A. A multicentre, prospective study to evaluate costs of septic patients in Brazilian intensive care units. Pharmacoeconomics 2008; 26: 425-434.
- Kafle S, Nath N. Improving management of severe sepsis and uptake of sepsis resuscitation bundle in an acute setting. BMJ Qual Improv Rep 2014; u204152.w1807
- Adcroft L. Improving sepsis management in the acute admissions unit. BMJ Qual Improv Rep 2014; u204974. w2091.
- McGregor C. Improving time to antibiotics and implementing the “Sepsis 6”. BMJ Qual Improv Rep 2014; u202548. w1443.
- https://www.ilas.org.br/costs-ii.php.
- Andrew R. The surviving sepsis campaign bundles and outcome: Results from the international multicentre prevalence study on sepsis (the IMPreSS study). Intensive Care Medicine 2015; 41: 1620-1628.
- Robson WP, Daniels R. The sepsis six: Helping patients to survive sepsis. Br J Nurs 2008; 17: 16-21.
- Robson W, Nutbeam T, Daniels R. Sepsis - A need for prehospital intervention? Emerg Med J 2009; 26: 535-538.
- Daniels R, Nutbeam T, McNamara G, Galvin C. The sepsis six and the severe sepsis resuscitation bundle: A prospective observational cohort study. EMJ 2011; 28: 507-512.
- Singer M, Deutschman CS, Seymour CW. The Third International Consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016; n315: 801-810.
- https://www.survivingsepsis.org/Improvement/Pages/default.aspx.
- Lloyd P, Provost SKM. The heath care data guide: Learning from data for improvement. Jossey-Bass, San Francisco 2011.
- Schofield T, Duero Posada J, Foroutan F. A local quality initiative to improve follow-up times for patients with heart failure. BMJ Open Qual 2017; 6: e000052.
- Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Healthc 2004; 13: 17- 32.
- Kumar P, Jordan M, Caesar J. Improving the management of sepsis in a district general hospital by implementing the 'Sepsis Six' recommendations. BMJ Open Qual 2015; 4: u207871.w4032.
- Peake SL, Delaney A, Bailey M. Goal-directed resuscitation for patients with early septic shock. N Engl J Med 2014; 371: 1496-1506.
- Quenot JP, Binquet C, Kara F. The epidemiology of septic shock in French intensive care units: The prospective multicentre cohort EPISS study. Crit Care 2013; 17: R65.
- Yealy DM, Kellum JA, Huang DT. A randomized trial of protocol-based care for early septic shock. N Engl J Med 2014; 370: 1683-1693.
- Daniels R. Surviving the first hours in sepsis: Getting the basics right (an intensivist's perspective). J Antimicrob Chemother 2011; 66: 11-23.

