Sjoukje Nauta1, Iris Knoester1, Monica van Zanten2, Erwin van Geenen1
1Department of Gastroenterology and Hepatology, Radboud University Medical Center, Nijmegen, The Netherlands
2Department of Pathology, Radboud University Medical Center, Nijmegen, The Netherland
*Corresponding Author:
Sjoukje Nauta
Radboud University Medical Center
Department of Gastroenterology and Hepatology
455, PO Box 9101, 6500 HB, Nijmegen
The Netherlands
Phone +31-24-3611111
Fax +31-24-3635129
E-mail sjoukje.nauta@radboudumc.nl
Received November 13th, 2015 - Accepted December 30th, 2015
Keywords
Carcinoma, Pancreatic Ductal; Carcinoma, Signet Ring Cell; Mesenteric Ischemia; Pancreatic Neoplasms
Abbreviations
CBD common bile duct; CT computed tomography; ERCP endoscopic retrograde cholangiopancreatography; PCI percutaneous coronary intervention
INTRODUCTION
Signet ring cell carcinoma is a very rare cause of malignancy of the pancreas. We present a case of primary signet ring cell carcinoma of the pancreas complicated by portal and mesenteric vein thrombosis with a rather prolonged course.
CASE REPORT
A seventy-one–year-old Caucasian male presented at a teaching hospital with icterus and malaise. His medical history included coronary heart disease with percutaneous coronary intervention (PCI) 10 years earlier and also an episode of abdominal pain and transient icterus 10 months previously, which had been diagnosed as pancreatitis. At that time, abdominal ultra-sonography had shown no gallstones or other abnormalities. At this presentation, the laboratory results showed elevated cholestatic liver enzymes with a total bilirubin concentration of 634 μmol/L (reference range <17 μmol/L), direct bilirubin of 539 μmol/L (reference range <5 μmol/L) and alkaline phosphatase 268 IU/L (reference range <115 U/L). Carbohydrate antigen 19.9 was just slightly elevated 53 E/ mL (reference range <37 E/mL). Abdominal computerized tomography (CT) revealed a tissue mass in the head of the pancreas with compression and dilation of the common bile duct (CBD), which was confirmed by endoscopic retrograde cholangiopancreatography (ERCP). During the ERCP a sphincterotomy and brush of the CBD was performed, followed by placement of a metal stent to ensure biliary drainage. Brush cytology showed no signs of malignancy. On suspicion of distal cholangiocarcinoma or carcinoma of the pancreatic head, the patient was referred to the surgical department for a pancreatoduodenectomy (Whipple procedure). During the operation, invasion of pathologic tissue was found around the portal vein. On site histopathology of the tissue revealed inflammation and no cancer cells. Taking these histopathology results and the invasion of the portal vein into account, instead of pancreatoduodenectomy a gastroenterostomy was performed. The resected surgical specimen showed diffuse inflammation. The icterus gradually resolved and the patient was discharged in good condition, with a working diagnosis of autoimmune pancreatitis.
Four months later, he presented with abdominal pain but no signs of icterus or fever. An abdominal CTscan showed thrombosis of the portal vein. The size of the tissue mass around the celiac artery, portal vein and pancreatic head had remained stable (Figure 1). IgG4 was 0.74 g/L (reference range 0.08-1.40 g/L). Because IgG4-negative autoimmune pancreatitis (AIP) was suspected, corticosteroid treatment (prednisone 40 mg once daily) was started. In addition, treatment with oral anticoagulants was started for the thrombosis of the portal vein. This combined treatment resulted in the restoration of the well-being of the patient. Three months later the oral anticoagulants had to be discontinued due tosevere rectal blood loss from extensive colorectal varicose veins, and the patient was referred to our university hospital for a second opinion. An abdominal CT scan to evaluate the prednisone response showed enlargement of the venous thrombus in the portal vein with expansion into the superior mesenteric vein and even into the inferior mesenteric vein, as well as some minor ascites. In addition, the size of the pancreatic head tissue mass was found to be stable. Cytological examination of the ascites revealed no malignancy.
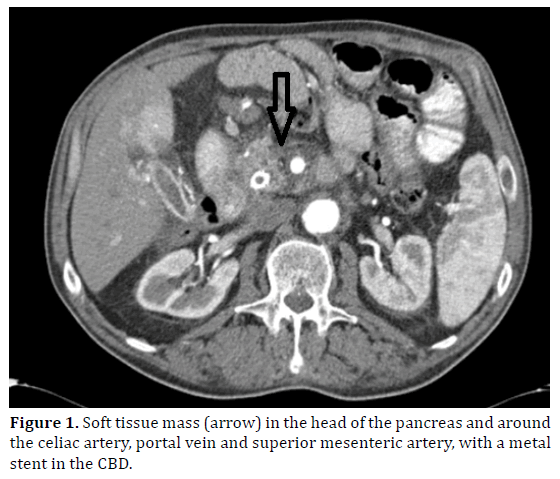
Figure 1. Soft tissue mass (arrow) in the head of the pancreas and around the celiac artery, portal vein and superior mesenteric artery, with a metal stent in the CBD.
A Positron Emission Tomography (PET) scan to detect or rule out malignancy in the pancreatic head or elsewhere, showed only staining of the tissue mass of the pancreatic head and portal vein region. Two attempts at fine needle aspiration (FNA) under endoscopic ultrasound guidance were madein order to get new material for cytology, but both were unsuccessful as neither the pylorus nor the anastomosis of the gastroenterostomy could be passed. Total parenteral nutrition was started for severe weight loss-27 kg in 6 months-due to abdominal pain caused by the mesenterial thrombosis. Even so, the patient died about one-and-a-half years after he first presented. A postmortem examination was performed.
On macroscopic examination at autopsy, the pancreatic head was seen to be enlarged and fibrous. Thorough examination showed no other suspected tumor foci, in particular no stomach, breast or colon lesions were detected. Histopathological examination of the soft tissue mass in and around the head of the pancreas revealed an adenocarcinoma. The tumor consisted of poorly cohesive round tumor cells with intracytoplasmic mucin and a peripherally placed, flattened nucleus (Figure 2). Because over 50% of the tumor showed this characteristic differentiation, it was classified as signet ring cell carcinoma. There was invasion of the celiac artery and the superior mesenteric artery, but no tumor cells were found in regional lymph nodes. There were no signs that the neoplasia was of ampullary or duodenal origin. Histopathological tissue specimens obtained at the operation 18 months previously were re-examined, but no signet ring cells were identified in these tissues (Figure 3).
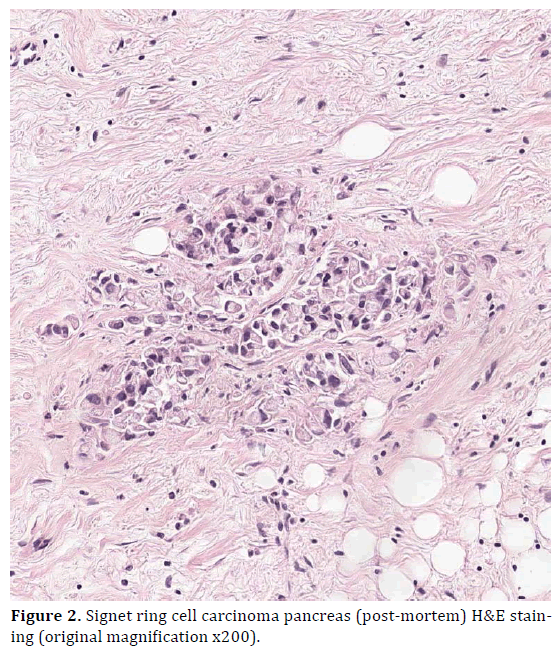
Figure 2. Signet ring cell carcinoma pancreas (post-mortem) H&E staining (original magnification x200).
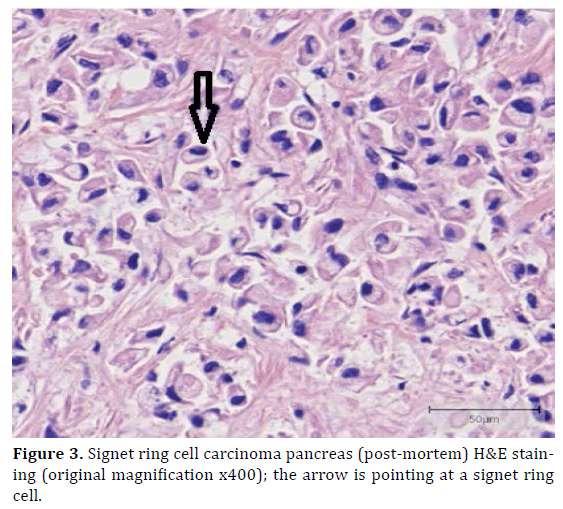
Figure 3. Signet ring cell carcinoma pancreas (post-mortem) H&E staining (original magnification x400); the arrow is pointing at a signet ring cell.
DISCUSSION
Carcinoma of the pancreas is a common malignancy, the incidence rate in the Netherlands in 2014 was 23:1000 persons per year [1]. Ninety-percent of pancreatic tumors are ductal adenocarcinomas; other histological types are relatively rare. When intracytoplasmatic mucin is abundant, it pushes aside the nucleus of the cell, resulting in a so-called signet ring cell. If more than 50% of the tumor is made up of cells of this type, it is classified as signet ring cell carcinoma (Figure 4).
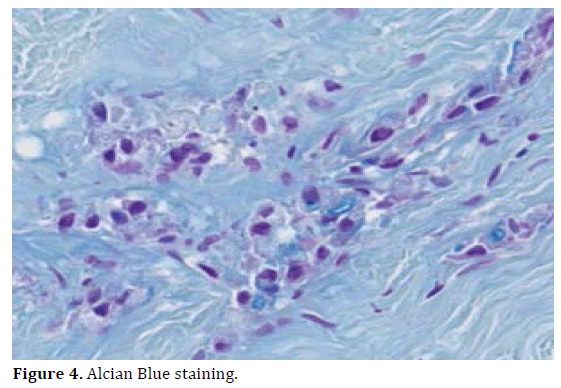
Figure 4. Alcian Blue staining.
Signet ring cell carcinoma is a very rare cause of malignancy of the pancreas, occurring in less than 1% of pancreatic carcinoma, and on which only 5 case reports have ever been published [2,3,4,5,6]. Signet ring cell carcinomas occur most frequently in the stomach and account for 15-30% of all gastric cancers. The tumor is uncommon in the colon, representing approximately 1-2 % of all colorectal cancers [6,7,8]. In the colon and stomach, signet ring cell carcinomas are an aggressive adenocarcinoma subtype with a poor prognosis overall [9,10,11,12,13].
We present a case of signet ring cell carcinoma of the pancreas which was only revealed at post-mortem examination. All other published cases of pancreatic signet ring cell carcinoma had a fulminant course [2,3,4,5,6] Conversely, in our patient, it had an unusually prolonged course. Although true histology was obtained at laparotomy, it was not conclusive. The final diagnosis was determined by post-mortem histopathological examination. The abnormal soft tissue mass in and around the head of the pancreas remained stable in size during our observation period, which could be consistent with a type 2 IgG4-negative AIP. However, as no improvement was observed after corticosteroid therapy, this diagnosis was rejected. Even after careful review of the first tissue specimen of the pancreatic head, we were unable to find any tumor cells. This can be explained by sampling of the inflammatory matrix surrounding the pancreatic carcinoma. At autopsy, no other primary tumor sites were noted. The pathologist particularly looked for lesions of the gastric or duodenal wall, and of the ampullary region as signet ring cell carcinoma is more common at these sites. Reflecting on our case, we would like to underline the presence of a peri-tumoral stromal fibrosis in patients with pancreatic carcinoma, which is a hallmark of this disease and can cover up the truth. A pancreatic mass should always be considered to be malignant, until proven otherwise.
Conflict of Interest
The authors have no potential conflicts of interest.
References
- https://www.cijfersoverkanker.nl
- Tracey KJ, O'Brien MJ, Williams LF, Klibaner M, George PK, Saravis CA, Zamcheck N. Signet ring carcinoma of the pancreas, a rare variant with very high CEA values. Immunohistologic comparison with adenocarcinoma. Dig Dis Sci 1984; 29:573-6. [PMID: 6327210]
- Chow LT, Chow WH. Signet-ring mucinous adenocarcinoma of the pancreas. Chin Med Sci J 1994; 9:176-8. [PMID: 7865839]
- McArthur CP, Fiorella R, Saran BM. Rare primary signet ring carcinoma of the pancreas. Mo Med 1995; 92:298-302. [PMID: 7643842]
- Marcy M, Chetaille B, Charafe-Jauffret E, Giovannini M, Delpéro JR, Monges G. Signet ring cell carcinoma of the pancreas: a case report. Ann Pathol 2002; 22:314-6. [PMID: 12410154]
- Lee NK, Kim S, Kim HS, Jeon TY, Kim GH, Kim DU, Park do Y, et al.,Spectrum of mucin-producing neoplastic conditions of the abdomen and pelvis: cross-sectional imaging evaluation.World J Gastroenterol 2011; 17:4757-71. [PMID: 22147976]
- Gopalan V, Smith RA, Ho YH, Lam AK. Signet-ring cell carcinoma of colorectum– current perspectives and molecular biology. Int J Colorectal Dis 2011; 26:127-133. [PMID: 20686774]
- Bosman FT, Carneiro F,Hruban RH, Theise ND. WHO Classification of Tumours of the Digestive System, 4th edn., Geneva, Switzerland: World Health Organization, International Agency for Research on Cancer; 2010.
- Piessen G, Messager M, Leteurtre E, Jean-Pierre T, Mariette C. Signet ring cell histology is an independent predictor of poor prognosis in gastric adenocarcinoma regardless of tumoral clinical presentation. Ann Surg 2009; 250:878. [PMID: 19855261]
- Hyung WJ, Noh SH, Lee JH, Huh JJ, Lah KH, Choi SH, Min JS. Early gastric carcinoma with signet ring cell histology. Cancer 2002; 94:78. [PMID: 11815962]
- Green JB, Timmcke AE, Mitchell WT, Hicks TC, Gathright JB Jr, Ray JE. Mucinous carcinoma--just another colon cancer? Dis Colon Rectum 1993; 36:49. [PMID: ]
- Nissan A, Guillem JG, Paty PB, et al., Signet-ring cell carcinoma of the colon and rectum: a matched control study. Dis Colon Rectum 1999; 42:1176. [PMID: 8380140]
- Psathakis D, Schiedeck TH, Krug F, Oevermann E, Kujath P, Bruch HP. Ordinary colorectal adenocarcinoma vs. primary colorectal signet-ring cell carcinoma: study matched for age, gender, grade, and stage. Dis Colon Rectum 1999; 42:1618. [PMID: 10613484]

