Keywords
Pancreatic Fistula; Pancreatectomy
Abbreviation
PF Pancreatic fistula
INTRODUCTION
Pancreatic fistula (PF) remains a serious complication after distal pancreatectomy, despite the development of various useful devices and techniques. Several stapler techniques for the transection of the pancreas to reduce the incidence of PF have been reported, although postoperative results remain unsatisfactory. Moreover, the usefulness of stapler closure for distal pancreatectomy compared with that of hand-sewn closure was not proven in a randomized, controlled multicenter trial [1]. Accordingly, the clinical benefits of closure using a stapler remain controversial.
In 2012, we performed a modified transection approach in which a stapler was used to compress the pancreas. We initially compressed the pancreas through a slow compression technique using an intestinal clamp. Additionally, we caudally shifted the transection line to avoid capsule injury during transection. Here, we report that the outcomes of pancreatic closure were improved through our proposed techniques for transection of the pancreas.
PATIENTS AND METHODS
We retrospectively reviewed the records of 50 patients who underwent open distal pancreatectomy for pancreatic cancer, intraductal papillary mucinous neoplasms, pancreatic neuroendocrine tumors, solid pseudopapillary neoplasms, and resectable non-malignant tumors from April 2007 to September 2015 at Osaka Medical College Hospital (Osaka, Japan). For the first 20 patients, who underwent surgery from April 2007 to June 2012, a stapler was used to compress the pancreas before transection, whereas slow compression using an intestinal clamp was performed for the remaining 27 patients from July 2012 to September 2015. Three patients with pancreatic cancer who underwent additional resection with a scalpel after firing of the stapler were excluded.
The drain was removed when the drain amylase level became lower than three times the upper limit of the normal serum amylase level. Clinical grading of PF was performed according to the International Study Group on Pancreatic Fistula Definition [2, 3]. A diagnosis of grade B or C, which are associated with a poorer clinical outcome, was evaluated according to the following criteria: (i) continuous drainage of >3 weeks, (ii) the diagnosis of infection, including sepsis, (iii) reinsertion of a drainage tube for fluid collection with an elevated drain amylase level more than three times the upper limit of normal amylase levels, (iv) the use of octreotide acetate, (v) perioperative re-drainage, and (vi) intravascular treatment for bleeding.
Intestinal Clamp
A ratchet-type intestinal clamp with nine teeth, as shown in Figure 1, was used in all procedures.
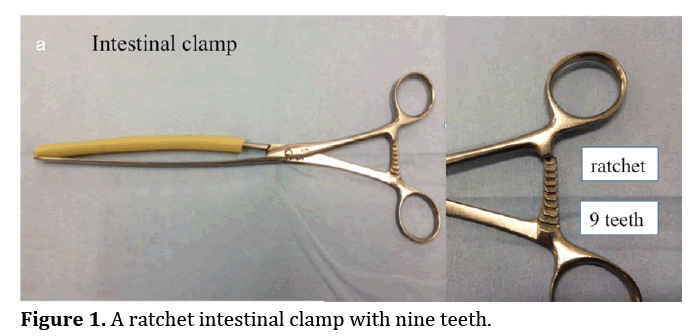
Figure 1. A ratchet intestinal clamp with nine teeth.
Conventional Transection
From April 2007 to June 2012, the pancreas was directly compressed using one of three staplers: model TL 60, Echelon_ or Endo GIA_. Transection was performed within 20 min while maintaining compression.
Slow Compression Using the Intestinal Clamp
From July 2012 to September 2015, slow compression using an intestinal clamp was performed according to the following method. First, the pancreas was compressed for 3 min using the intestinal clamp with three clicks out of nine clicks. Then, an additional three clicks for 3 min. Finally, the last three clicks were used for 3 min. After removing the intestinal clamp, the compression line was visible. After caudally shifting the transection line on the compression site, the stapler was fired for approximately 1 min. During this period, either the Echelon_ or Endo GIA_ stapler was used.
Statistical Analysis
Data are expressed as a mean values ± standard deviation and were compared using the Wilcoxon test. All analyses were performed using SAS version 10 software (SAS Institute, Cary, NC, USA). Values of p<0.05 were considered significant.
RESULTS
In Figure 2, conventional transection using a sausage as a high stress model is demonstrated (Figure 2a). When the sausage was transected with a stapler without compression with the intestinal clamp, it was deformed (Figure 2b–e), not only the stump, but also the capsule of the pancreatic remnant (arrow). In contrast, when using the intestinal clamp, the sausage was not deformed, but rather flattened by compression in a step by step manner (Figure 3a–c). After caudally shifting the transection line on the compression site (Figure 3d), the sausage was transected without any injuries (Figure 3e).
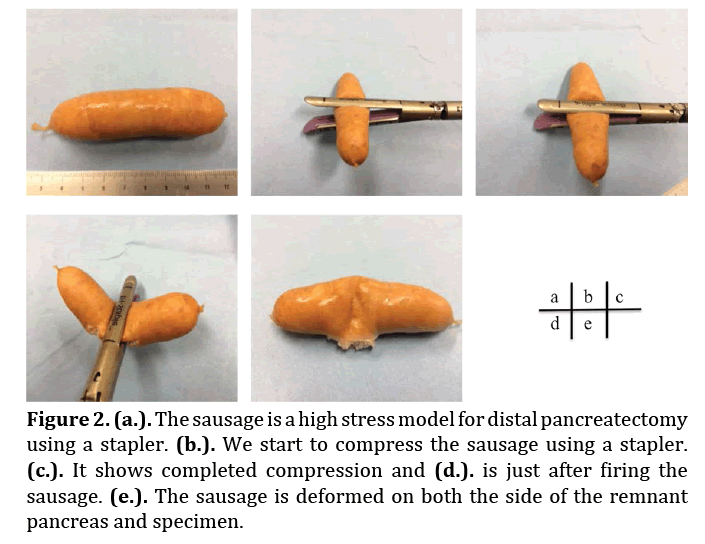
Figure 2. (a.). The sausage is a high stress model for distal pancreatectomy using a stapler. (b.). We start to compress the sausage using a stapler. (c.). It shows completed compression and (d.). is just after firing the sausage. (e.). The sausage is deformed on both the side of the remnant pancreas and specimen.
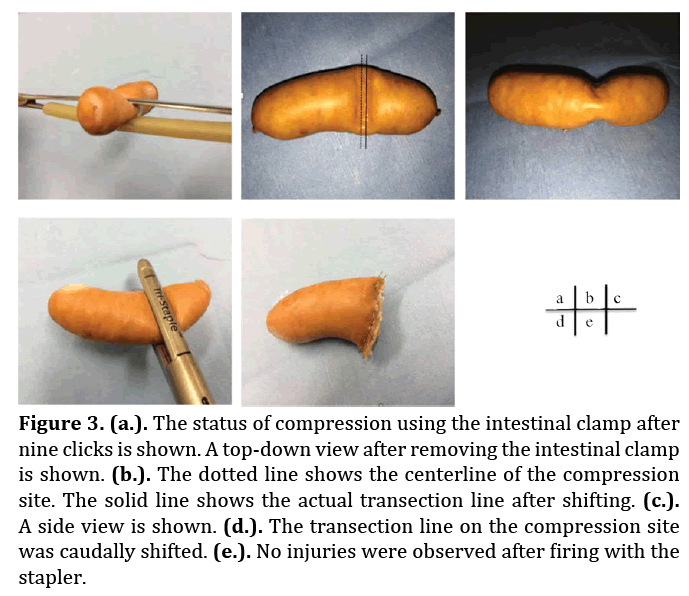
Figure 3. (a.). The status of compression using the intestinal clamp after nine clicks is shown. A top-down view after removing the intestinal clamp is shown. (b.). The dotted line shows the centerline of the compression site. The solid line shows the actual transection line after shifting. (c.). A side view is shown. (d.). The transection line on the compression site was caudally shifted. (e.). No injuries were observed after firing with the stapler.
Figure 4 illustrates our actual clinical procedure based on the above theory. Patient demographics are summarized in Table 1. The most common indication for distal pancreatectomy was pancreatic cancer in both groups. Regarding pancreatic texture, there was no significant difference among patients in our series.
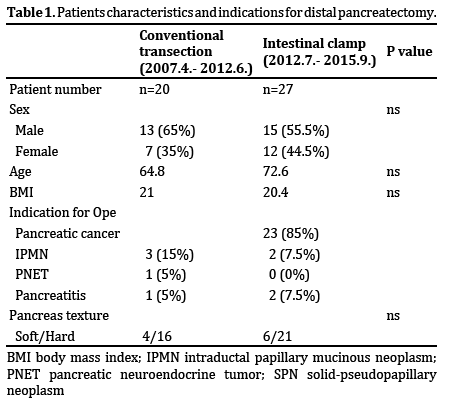
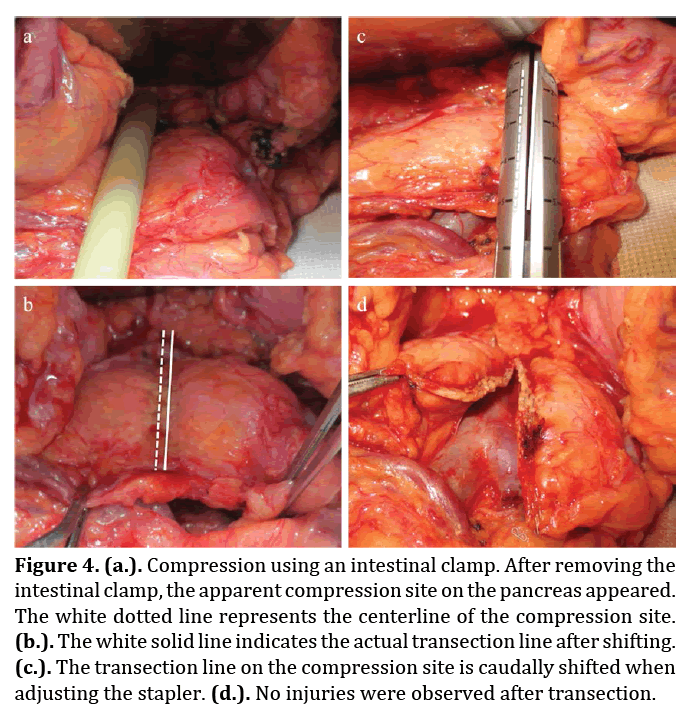
Figure 4. (a.). Compression using an intestinal clamp. After removing the intestinal clamp, the apparent compression site on the pancreas appeared. The white dotted line represents the centerline of the compression site. (b.). The white solid line indicates the actual transection line after shifting. (c.). The transection line on the compression site is caudally shifted when adjusting the stapler. (d.). No injuries were observed after transection.
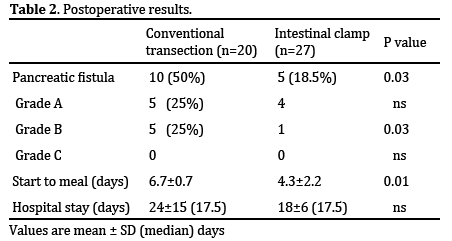
The incidence of PF is shown in Table 2. Ten patients in the conventional transection group developed PF of which five were grade B. On the other hand, only five patients in the intestinal clamp group developed PF (p = 0.03) of which only one was grade B. The median time for the patient to consume a meal was shorter in the intestinal clamp group than conventional resection group. There was no significant difference in postoperative hospital stay between groups.
DISCUSSION
PF is the most severe complication of distal pancreatectomy with an incidence of 5%–40% [4-6], although according to the classification of the International Study Group of Pancreatic Fistula, this rate is still high. Transection using a stapler has rapidly spread since Pachter [7] first reported the use of the TA-55 stapler (Tyco Healthcare–Covidien Ltd.) for distal pancreatectomy in 1979 [7]. Since then, many devices have been developed that differ in size and the number of rows of stapler. Numerous attempts using these devices, such as the GIA- 80 (Tyco Healthcare), Endo GIA_ (Tyco Healthcare), and Endo SGIA staplers, have been employed to prevent the development of PF. However, almost all attempts have substantially failed to decrease the incidence of PF. Also, many reports have addressed strategies to manage stump closure. A possible cause of PF can be explained as resulting from insufficient closure of unrecognized or unsealed pancreatic branches on the stump. However, Nakamura et al. [8] recently reported that peri-firing compression using a stapler in laparoscopic distal pancreatectomy was sufficient to prevent PF. This transection method included compression of the pancreas before transection to tightly seal the pancreatic branches on the stump, thus focusing on the managemsent of the stump. Our main purpose in conventional transection was the same; however, our method was unable to decrease the incidence of PF in our institution. Therefore, we developed the following hypothesis regarding the mechanism of PF after distal pancreatectomy in cases for which we used a linear stapler. First, the site of PF may not always be the stump, but can also be caused by the laceration of the capsule of the pancreatic remnant. Second, slow compression or gradual equal compression may prevent laceration of the capsule of the pancreatic remnant rather than completely biting the pancreas using only one action with the stapler. Finally, by caudally shifting the transection line, while maintaining compression, it may be possible to reduce tension on the capsule of the pancreatic remnant and to more tightly seal the branches on the stump. In accordance with the above hypothesis, we changed the compression method and achieved satisfactory results, which indicated that our procedure was sufficient to avoid deforming both recognized and unrecognized pancreatic ducts on the stump and to reduce the tension on the capsule of the pancreatic remnant.
Various procedures for the surgical management of the stump of the pancreatic remnant have been reported. For example, Sudo et al. [9] reported the effectiveness of ductto- mucosa pancreaticogastrostomy with an incidence of grade B and C PF of 0% and grade A PF of 29%. Similarly, Meniconi et al. [10] reported no cases of PF among patients who underwent pancreaticojejunostomy. In addition, a low incidence of PF was achieved in the management of the stump using a patch, such as the greater omentum [11] or the falciform ligament [12]. However, these procedures are relatively complicated compared with our procedure.
Compared with hand-sewn closure, stapler closure did not improve the rate of PF development following distal pancreatectomy in a randomized, controlled multicenter trial [1]. However, the use of a formal transection method, such as the procedure described in this report, which was certainly able to reduce the incidence of PF, may spread in the future.
Here, we described a new technique using an intestinal clamp to decrease the incidence of PF. Two important points of our procedure should be considered: first, slow compression was able to reduce laceration of the remnant pancreas and second, caudally shifting the transection line enabled us to avoid deforming the stump of the pancreatic remnant. Moreover, surgeons with little experience will be able to easily perform our technique in less time.
CONCLUSION
In conclusion, our technique provides many advantages, as it is a simple, convenient, and quick technique to reduce the incidence of PF. Also, our technique may be useful for patients with either a soft or hard pancreas. Of course, this new technique needs more detailed research, especially randomized controlled studies because the limitations of our study are its retrospective nature and small number of patients.
Conflict of Interest
The authors declare that they have no competing interests.
References
- Diener MK, Seiler CM, Rossion I, Kleeff J, Glanemann M, Butturini G, Tomazic A, et al. Efficacy of stapler versus hand-sewn closure after distal pancreatectomy (DISPACT): a randomised, controlled multicentre trial. Lancet 2011; 377:1514-22. [PMID: 21529927]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005;138:8-13. [PMID: 16003309]
- Pratt WB, Maithel SK, Vanounou T, Huang ZS, Callery MP, Vollmer CM Jr. Clinical and economic validation of the International Study Group of Pancreatic Fistula (ISGPF) classification scheme. Ann Surg 2007;245:443-51. [PMID: 17435552]
- Knaebel HP, Diener MK, Wente MN, Büchler MW, Seiler CM. Systematic review and meta-analysis of technique for closure of the pancreatic remnant after distal pancreatectomy. Br J Surg 2005;92:539-46. [PMID: 15852419]
- Zhou W, Lv R, Wang X, Mou Y, Cai X, Herr I. Stapler vs suture closure of pancreatic remnant after distal pancreatectomy: a meta-analysis. Am J Surg 2010; 200:529-36. [PMID: 20538249]
- Oláh A, Issekutz A, Belágyi T, Hajdú N, Romics L Jr. Randomized clinical trial of techniques for closure of the pancreatic remnant following distal pancreatectomy. Br J Surg 2009;96:602-7. [PMID: 19434697]
- Pachter HL, Pennington R, Chassin J, Spencer FC.Simplified distal pancreatectomy with the Auto Suture stapler: preliminary clinical observations.Surgery 1979;85:166-70. [PMID: 369013]
- Nakamura M, Ueda J, Kohno H, Aly MY, Takahata S, Shimizu S, Tanaka M. Prolonged peri-firing compression with a linear stapler prevents pancreatic fistula in laparoscopic distal pancreatectomy. Surg Endosc 2011; 25:867-71. [PMID: 20730447]
- Sudo T, Murakami Y, Uemura K, Hayashidani Y, Hashimoto Y, Nakashima A, Ohge H, et al. Distal pancreatectomy with duct-to-mucosa pancreaticogastrostomy: a novel technique for preventing postoperative pancreatic fistula. Am J Surg 2011;202:77-81. [PMID: 21600558]
- Meniconi RL, Caronna R, Borreca D, Schiratti M, Chirletti P.Pancreato-jejunostomy versus hand-sewn closure of the pancreatic stump to prevent pancreatic fistula after distal pancreatectomy: a retrospective analysis. BMC Surg 2013; 2:13-23. [PMID: 23819892]
- Wang M, Zhu F, Peng F, Tian R, Shi C, Xu M, Li X, et al. Greater omentum binding: a simple technique to cover the pancreatic remnant after distal pancreatectomy. J Am Coll Surg 2014;219:e19-23. [PMID: 25038967]
- Fujino Y, Sendo H, Oshikiri T, Sugimoto T, Tominaga M. A novel surgical technique to prevent pancreatic fistula in distal pancreatectomy using a patch of the falciform ligament.Surg Today 2015;45:44-9. [PMID: 24909496]

