Keywords
complications; Enteral Nutrition; Pancreatectomy
Abbreviations
NJ: nasojejunal; PJ: percutaneous transperitoneal jejunal; PTGJ: percutaneous transgastric jejunal
INTRODUCTION
Postoperative nutrition is a well recognised aspect of care in recent years and has been shown to reduce the incidence of complications and to reduce hospital stay. Enteral nutrition has clearly been shown to be superior to parenteral nutrition as it is cheaper, safer, more physiological and early enteral nutrition has been confirmed to reduce postoperative morbidity [1, 2, 3, 4].
Following pancreatic resection, early postoperative jejunal nutrition was shown to be safe and positively affect outcomes including nutritional status and wholebody protein kinetics. Furthermore, it was found to contribute to a significantly lower incidence of pancreatic fistula, resulting in a shorter duration of hospitalization compared to patients receiving late postoperative enteral nutrition [5, 6].
Enteral nutrition is normally administered via a fine bore tube placed in the proximal small intestine. In our center this is achieved either via the percutaneous route (percutaneous transperitoneal jejunal feeding tube or percutaneous transgastric jejunal feeding tube) or via a nasojejunal feeding tube.
Several complications have been reported using the percutaneous methods [7, 8, 9] and in a recent randomized trial the nasoenteral route has been found to be safer in patients after oesophagogastrectomy [10]. However, following major pancreatic resection, where a good part of the stomach is normally left and long segments of small bowel are normally involved in the procedure, there is no clear consensus yet, as to the most efficacious and safest route for postoperative feeding.
We have retrospectively compared the three methods in use in terms of efficiency and safety in a large cohort of patients undergoing pancreatic resections. The main endpoints were efficacy and complications.
PATIENTS AND METHODS
Data were retrospectively reviewed from a prospectively maintained database for all patients undergoing pancreatic resection (n=100: 93 Whipple’s pancreaticoduodenectomy and 7 total pancreatectomy) between January 2007 and June 2008. Clinical records were consulted when any clarifications were needed. Table 1 shows the patient characteristics and summary data, as well as, the distribution of cases by the type of feeding tube used.
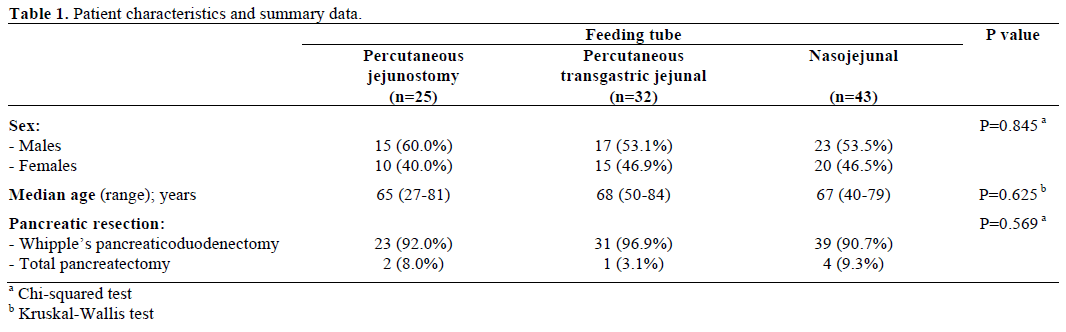
Three techniques of feeding tube placement were employed: percutaneous jejunostomy feeding tube (PJ); percutaneous transgastric jejunal feeding tube (PTGJ); and nasojejunal feeding tube (NJ). All three surgeons had used more than one technique, the choice was based on surgeon’s preference and intraoperative judgment.
The PJ was performed with the needle catheter jejunostomy technique as originally described [11] using the Freka FCJ 9 Fr tube (Fresenius Kabi, Bad Homburg, Germany). PTGJ was performed through the anterior gastric wall just before completion of the gastrojejunal anastomosis and a nasogastric tube was passed into the efferent jejunal loop beyond all anastomoses. The extragastric part of the tube was buried in the gastric wall with the Witzel technique before reaching the anterior abdominal wall [12, 13].
Two types of NJ tubes were used. For the first 27 cases, the Medicina® double lumen nasogastric feeding tube without guide wire (Maxter Catheters, Marseille, France) was used and for the remaining 16 cases, the Corscope® nasojejunal tube (Viasys Medsystems, Wheeling, IL, USA) with a guidewire in situ was used. The NJ tube was inserted nasally by the anaesthetist to reach the stomach and just before completion of the gastrojejunal anastomosis; the tube was manipulated past the anastomosis to lie well into the jejunum. The tube was then securely taped in place around the nose by the anaesthetist. Additionally, a nasogastric drainage tube was placed in all patients having PJ and PTGJ and patients in the NJ group having the Corscope® tube. This tube was left on free drainage and was removed when less than 500 mL was drained in 24 hours.
Normal saline was administered via the feeding tube at 10 mL/h post operatively. Enteral feeding with Nutrison® standard (Nutricia, Trowbridge, United Kingdom) to provide 1 kcal/mL was started at 10 mL/h, 24 hours postoperatively. This was increased daily as tolerated by 20 mL to a maximum of 80 mL/h. Most patients were allowed to commence oral intake when enteral nutrition was in progress; enteral nutrition feeding was stopped when patients were able to tolerate full oral intake containing solid food. The feeding tube was removed in the NJ group at this stage, whereas in patients with percutaneous (PJ, PTGJ) tubes, the feeding catheter was removed in the outpatients at 4-6 weeks.
The primary outcome measure was tube related complications defined by any feeding tube related event leading to ineffectual feeding or to increase in morbidity/patient discomfort. Other information collected included patient demographics, type of procedure, type of reconstruction, hospital stay, type of feeding tube used, nasogastric aspirates, time to return of bowel function, time to stop enteral feeding, postoperative surgical and general complications.
ETHICS
All patients gave voluntary written informed consent for their data to be analysed in the study. The consent obtained was routinely incorporated in the standard consent form completed at the time of preoperative discussion with the patient. The study was conducted in accordance with “Guidelines on Good Clinical Practice” and the principles of the Declaration of Helsinki following approval of the Institutional Review Board.
STATISTICS
Measures of central tendency for continuous variables were compared using the Kruskal-Wallis test and categorical data were compared using the chi-squared test. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS v. 15.0) and MedCalc v9.3.9. Statistical significance was defined at the two-tailed 95% level.
RESULTS
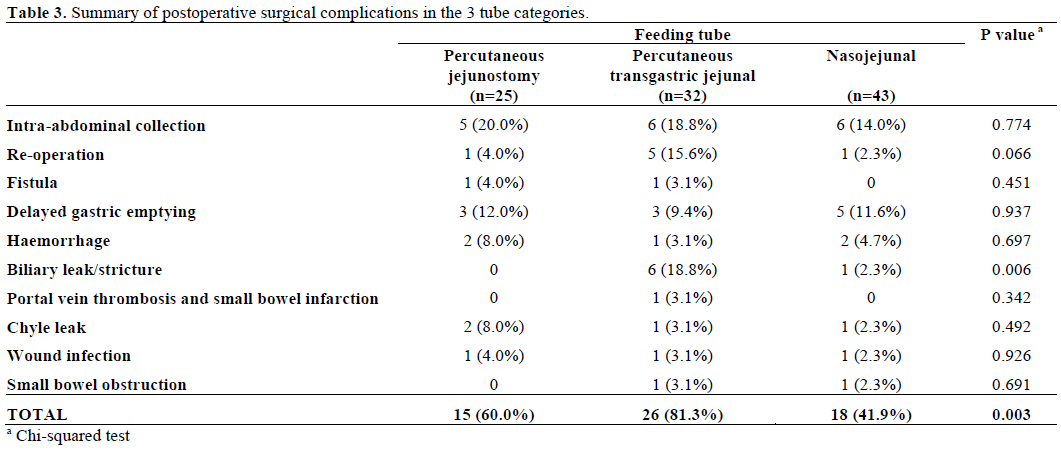
A total of 118 complications were encountered in 64 patients (64.0%) (Table 2). In the PJ group, 16 of 25 patients (64.0%) had 30 complications. In the PTGJ group, 24 of 32 patients (75.0%) developed 50 complications. In the NJ group, 24 of 43 patients (55.8%) developed 38 complications (P=0.231). The frequency of surgical complications was significantly different (P=0.003) among the three different feeding tubes. Table 3 summarizes the postoperative surgical complications in the three tube categories. Biliary leak/stricture was significantly higher (P=0.006) in patients with the PTGJ tube. We would be cautious in our conclusion of significantly higher overall surgical complications and biliary complications/strictures in the PTGJ group. All 3 surgeons have been involved in this group and hence it is difficult to put it to surgeon or technical related complications and we find that the small number, although significant is difficult to justify firm conclusions. However, this could be addressed by randomization in a prospective trial. Altogether 7 patients underwent re-laparotomy. One patient in each of the PJ and the NJ groups (4.0% and 2.3%, respectively) and 5 in the PTGJ group (15.6%) required re-operation. No re-operation was for a catheter or feeding related problem (Table 4).


Two patients died (Tables 4 and 5): one in PTGJ group for biliary peritonitis followed by ventilatory failure, and one in the NJ group for multiple operations for fulminant intra-abdominal sepsis following perforation of obstructed small bowel from pelvic adhesions following previous surgery. No deaths were catheter related.
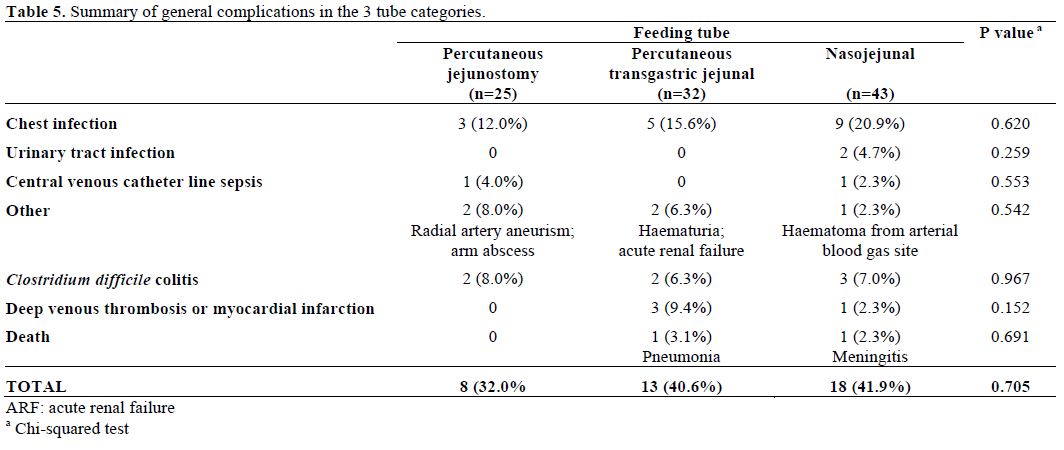
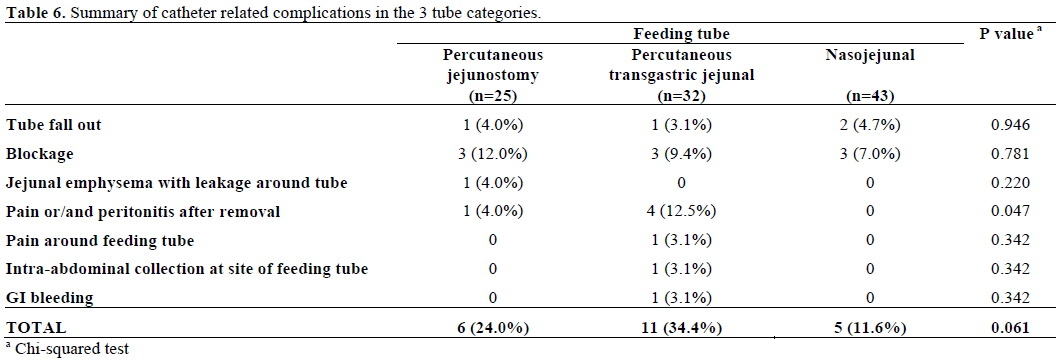
Nine patients (20.9%) in the NJ feeding group developed chest infection, as against 3 (12.0%) in PJ and 5 (15.6%) in the PTGJ groups (P=0.620) (Table 5). Six patients (24.0%) in the PJ group had catheterrelated complications, 11 (34.4%) in the PTGJ group and 5 patients (11.6%) in NJ group (P=0.061) (Table 6). Only 1 patient had a blocked NJ tube when the Corscope® NJ tube was used, whereas in the patients who had Medicina® double-lumen NJ tube, the tube fell out early in 2 patients and was blocked in 2 other patients. Pain or/and peritonitis after removal was significantly higher in the PTGJ group (P=0.047). The key here is whether there is more pain or more peritonitis as clearly pain alone would be a point for patient concern but peritonitis could lead to further investigations/microbiological morbidity or even relaparotomy. It is prudent to note that while the result was significant it did not lead to a significant rate of relaparotomy (P=0.066; Table 3) between groups although this could be a concern.
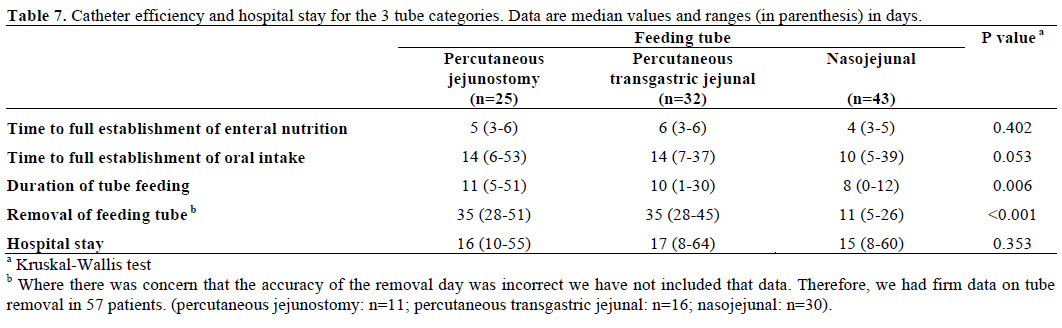
The median duration of enteral feeding was 11 days (range: 5-51 days) in the PJ group, 10 days (range: 1- 30 days) in the PTGJ group and 8 days (range: 0-12 days) in the NJ group (Table 7). The median hospital stay was similar in the three groups (P=0.303). Median time to resumption of normal diet was shortest in the NJ group at 10 days (range: 5-39 days), whereas it was 14 days respectively in the PJ (range: 6-53 days) and PTGJ (range: 7-37 days) groups (P=0.018).
DISCUSSION
Malnutrition is a significant problem in patients undergoing major gastrointestinal surgery. Patients subjected to pancreatic resection are at higher risk of multiple surgical and systemic complications as a result of the magnitude of operation and these problems are compounded in the presence of malnutrition. In several randomized trials and meta-analyses, postoperative enteral feeding has been shown to be safer than parenteral nutrition and associated with significantly lower postoperative morbidity [1, 2, 3, 4, 14]. Therefore, nutritional provision has become a vital part of conventional postoperative care and is a standard practice in many centers following major abdominal resections. Different routes have been used but the safest and most effective route for feeding is still unclear and the choice remains based on the surgeon’s familiarity with a specific technique. Percutaneous feeding jejunostomy is the most commonly used route; however, several complications related to this technique have been reported [7, 8, 9, 15, 16, 17]. As the main aim of enteral feeding is to reduce postoperative morbidity, it is inexpedient to have additional complications as a result of this procedure.
Herein we present a series of 100 consecutive major pancreatic resections where, three different routes were used. In our study, catheter related complications were frequently associated with the percutaneous techniques. These consisted of leakage and pain at the tube site at the time of removal of catheter 5-6 weeks postoperatively, requiring hospitalization for short periods. These episodes of pain were presumed to be related to leakage of small volumes of luminal content. Among the major complications of PJ reported in the literature are small bowel perforations, volvulus with infarction, bowel necrosis and pneumatosis intestinalis requiring re-operation and occasionally death as a result [9, 17, 18]. The NJ group had the lowest incidence of catheter-related complications with blockage and displacement being the most common. However, following a change in the purchase policy by the hospital, a different type of NJ feeding tube (Corscope® NJ tube) was used for 16 patients after November 2007. Surprisingly, only one patient, who had delayed gastric emptying requiring prolonged enteral feeding, had a blockage of catheter after 15 days of feeding and necessitated replacement.
A recent randomized trial comparing nasojejunal feeding and percutaneous jejunal feeding in oesophageal surgery reported 30% complication rate in the NJ group, tube dislocation being the most common [10]. In our study, it was possible to reduce the incidence of displacement and blockage of nasojejunal tubes by using a tube with a wider diameter enabling more secure fixation at the nostrils. Patient discomfort was not recorded in this study, but none of the patients reported any problems with having a tube in the nose for feeding purposes.
There was no significant difference in the duration of enteral feeding in the 3 groups; the majority of patients were able to tolerate full enteral feed by the 4th/5th postoperative day. None of our patients required reoperation as a result of feeding tube complications. Notably, the incidence of chest infections was marginally higher in patients having NJ feeding (21%), which may reflect interference with the cough mechanism by the presence of two tubes in the pharynx. However, this did not result in adverse effect on gut function or hospital stay of these patients.
In addition to being safer than percutaneous feeding techniques, NJ when compared to the PJ technique has the additional advantage of not risking damage to jejunum particularly as the jejunum is utilized for multiple anastomoses in pancreatic surgery. In our study, we observed a small, albeit non significant, difference in that patients who had NJ tube feeding took shorter time to full establishment of enteral nutrition and oral intake. They also required a significantly shorter duration of tube feeding. It is probable that the maneuvers of handling, puncturing and anchoring the jejunum to abdominal wall cause a degree of trauma in patients undergoing percutaneous techniques.
This study is limited by the non-random allocation of patients to the different feeding tube techniques. Although there appeared to be an obvious clinical difference in tube related complications, this did not achieve statistical significance (P=0.061). The PJ and PTGJ tubes were left in place for longer than NJ tubes (as policy) no significant differences were observed between the groups in time to establish enteral feeding or oral intake, as well as in hospital stay, while duration of feeding was significantly shorter in NJ patients. Further, the choice of method was surgeon related, introducing a possible source of bias, so differences in complication rates and in time to establish oral feeding or stop enteral nutrition should be viewed with caution. Our data do however provide sufficient information to enable calculation of an appropriate sample size for a randomized trial to compare NJ with percutaneous routes of administration.
CONCLUSION
NJ feeding is equally efficacious in comparison to percutaneous feeding in delivering enteral nutrition to patients undergoing major gastrointestinal surgery. In our study it is safer than percutaneous techniques and is associated with only minor complications. However, a randomized controlled trial is needed to establish the best feeding method in pancreatic surgery patients.
Acknowledgments
This paper was presented as a poster at the “XL Meeting of European Pancreatic Club” (Lodz, Poland; 25-28 June 2008) and as oral presentation at the “Pancreatic Society of Great Britain and Ireland” (Derby, England, United Kingdom; 30-31 October 2008)
Conflict of interest
The authors have no potential conflicts of interest
References
- Moore FA, Feliciano DV, Andrassy RJ, McArdle AH, Booth FV, Morgenstein-Wagner TB, et al. Early enteral feeding, compared with parenteral, reduces postoperative septic complications. The results of a meta-analysis. Ann Surg 1992; 216:172-83. [PMID 1386982]
- Mazaki T, Ebisawa K. Enteral versus parenteral nutrition after gastrointestinal surgery: a systematic review and meta-analysis of randomized controlled trials in the English literature. J GastrointestSurg 2008; 12:739-55. [PMID 17939012]
- Jeejeebhoy KN. Enteral nutrition versus parenteral nutrition--the risks and benefits. Nat ClinPractGastroenterolHepatol 2007; 4:260- 5. [PMID 17476208]
- Bozzetti F, Braga M, Gianotti L, Gavazzi C, Mariani L. Postoperative enteral versus parenteral nutrition in malnourished patients with gastrointestinal cancer: a randomisedmulticentre trial. Lancet 2001; 358:1487-92. [PMID 11705560]
- Okabayashi T, Kobayashi M, Nishimori I, Sugimoto T, Akimori T, Namikawa T, et al. Benefits of early postoperative jejunal feeding in patients undergoing duodenohemipancreatectomy. World J Gastroenterol 2006; 12:89-93. [PMID 16440423]
- Okabayashi T, Kobayashi M, Nishimori I, Sugimoto T, Onishi S, Hanazaki K. Risk factors, predictors and prevention of pancreaticfistula formation after pancreatoduodenectomy. J Hepatobiliary PancreatSurg 2007; 14:557-63. [PMID 18040620]
- Smith CD, Sarr MG. Clinically significant pneumatosisintestinalis with postoperative enteral feedings by needle catheter jejunostomy: an unusual complication. JPEN J Parenter Enteral Nutr 1991; 15:328-31. [PMID 1907684]
- Myers JG, Page CP, Stewart RM, Schwesinger WH, Sirinek KR, Aust JB. Complications of needle catheter jejunostomy in 2,022 consecutive applications. Am J Surg 1995; 170:547-50. [PMID 7491998]
- Holmes JH 4th, Brundage SI, Yuen P, Hall RA, Maier RV, Jurkovich GJ. Complications of surgical feeding jejunostomyin trauma patients. J Trauma 1999; 47:1009-12. [PMID 10608526]
- Han-Geurts IJ, Hop WC, Verhoef C, Tran KT, Tilanus HW. Randomized clinical trial comparing feeding jejunostomywith nasoduodenal tube placement in patients undergoing oesophagectomy. Br J Surg 2007; 94:31-5. [PMID 17117432]
- Delany H M, Carnevale N J, Garvey J W. Jejunostomy by a needle catheter technique. Surgery 1973; 73:786-90. [PMID 4697097]
- Witzel O. ZurTechnik der Magenfistulaeinlegung. ZblChir 1891; 18:601-4.
- Tapia J, Murguia R, Garcia G, de los Monteros PE, O?ate E. Jejunostomy: techniques, indications, and complications. World J Surg 1999; 23:596-602. [PMID 10227930]
- Gramlich L, Kichian K, Pinilla J, Rodych NJ, Dhaliwal R, Heyland DK. Does enteral nutrition compared to parenteral nutrition result in better outcomes in critically ill adult patients? A systematic review of the literature. Nutrition 2004; 20:843-8. [PMID 15474870]
- De Gottardi A, Kr?henb?hl L, Farhadi J, Gernhardt S, Sch?fer M, B?chler MW. Clinical experience of feeding through a needle catheterjejunostomy after major abdominal operations. Eur J Surg 1999; 165:1055-60. [PMID 10595610]
- Sonawane RN, Thombare MM, Kumar A, Sikora SS, Saxena R, Kapoor VK, Kaushik SP. Technical complications of feeding jejunostomy: a critical analysis. Trop Gastroenterol 1997; 18:127-8. [PMID 9385860]
- Ryan AM, Rowley SP, Healy LA, Flood PM, Ravi N, Reynolds JV. Post-oesophagectomy early enteral nutrition via a needle catheter jejunostomy: 8-year experience at a specialist unit. ClinNutr 2006; 25:386-93. [PMID 16697499]
- Sarr MG. Appropriate use, complications and advantages demonstrated in 500 consecutive needle catheter jejunostomies. Br J Surg 1999; 86:557-61. [PMID 10215836]

