Keywords
Adenocarcinoma; Lymph Nodes; Nomograms; Pancreas
Abbreviations
OS overall survival; PDAC pancreatic ductal
adenocarcinoma
INTRODUCTİON
Pancreatic cancer inflicts more than 400,000 deaths
annually worldwide [1] and ranks fourth among the most
common killer cancers in the United States [2, 3]. Exocrine
pancreatic cancers, dominated by pancreatic ductal
adenocarcinoma (PDAC), remain a dreadful finding for
only 20% of patients are determined eligible for a curative
surgical resection at the time of diagnosis [4] and all are
expected to eventually succumb to this disease.
Our current knowledge of PDAC indicates that lymph
node status is one of the most significant predictors of local
recurrence, and subsequently disease-free and overall
survival (OS) [5, 6, 7]. The adequate extent of prognostic
lymphadenectomy in PDAC of the head and neck of the pancreas currently follows the recommendations
of the consensus meeting of the International Study
Group on Pancreatic Surgery (ISGPS) [8] to include the
hepatoduodenal ligament nodes (stations 5, 6, 12b1,
12b2, 12c), the hepatic artery nodes (station 8a), the
posterior pancreatic head nodes (stations 13a and 13b),
the superior mesenteric artery nodes (14a and 14b) and
anterior pancreatic head nodes (stations 17a and 17b)
[9]. For PDAC of the body or tail, the standard extent of
lymphadenectomy entails the removal of the hilar splenic
nodes (station 10), splenic artery nodes (station 11), and
inferior pancreatic nodes (station 18) [10]. Adherence to
the standardized description of lymphadenectomy in PDAC
is expected to yield ≥12 nodes per the recommendation of
the American Joint Committee on Cancer (AJCC) during
pancreatic resection for adequate nodal stating of this
disease [11].
In some instances, however, the number of retrieved
lymph nodes does not meet this requirement despite
the surgeon’s best effort to comply with the technical
guidelines. Therefore, several studies attempted to
compensate for this shortage by addressing the ratio,
rather than the absolute number, of positive lymph nodes [12, 13, 14, 15]. The main criticism of this approach
revolved around the repeated need for a large number
of lymph nodes to yield a precise ratio, which results in a
possible inflation in survival due to stage migration [16, 17]. It was suggested in some reports that the retrieval of a
higher number of negative nodes, thus decreasing the ratio
of positive nodes, might outline an improved local control
or surgical downstaging of the disease [18, 19]. However,
a large body of evidence generated a broad agreement that
extended lymphadenectomy in PDAC resections carries
higher rates of morbidity without evidence of survival
benefit [8, 10, 20, 21, 22, 23, 24].
In this study, we use the National Cancer Database
(NCDB), a large population-based cancer registry
collected and maintained by the American College of
Surgeons Committee on Cancer (ACS-CoC), which captures
approximately 70% of the cancer cases nationwide, to
develop a clinicopathological nomogram that predicts
nodal metastasis in PDAC. This nomogram can be utilized
as a tool for nodal staging in cases where the retrieval of
the required 12 nodes is not achieved.
METHODS
The NCDB for PDAC between 2004-2015 was used for
the analysis. A series of inclusion and exclusion criteria
were applied as follows:
• Only patients who were found to have pancreatic
duct adenocarcinoma (PDAC) on final pathology were
included.
• Patients with metastatic disease (M1) were excluded.
• Patients who were reported to receive any type of
treatment with a palliative intent were excluded.
• Only patients who received a surgical treatment with a
curative intent for their diagnosed PDAC and achieved
R0 resection were included.
• All patients were staged in compliance with the
American Joint Committee on Cancer (AJCC) 7th edition
for PDAC as reported in the NCDB for the years of data
collection.
• Only patients who had a known T stage to be T1-T3
were included in the analysis. Patients with T0, Tis, TX,
and T4 (unresectable disease per the AJCC 7th edition
TNM staging) were excluded.
• Only patients who had a known number of retrieved
nodes and a known number of positive nodes were
included.
• After conclusion of the predictive variables of N1 in the
logistic regression model, patients who had missing
data of any of the predictive variables were excluded
from the analysis for that would affect the calculation
of the predicted probability of that case.
Binary univariate and multivariate logistic regressions
were applied to identify the predictors of nodal involvement
in PDAC (N0 vs. N1). This regression model was used as the basis of our nomogram. The nomogram model was then
constructed following the formula:

Patients whose data of the predictive variables were
missing were excluded from the final analysis. Given
the relatively large size of the study population, we
internally validated the derived model using the 10-fold
cross-validation method where 1/10 of observations are
removed and the reduced, fixed dataset is used to exercise
the model (i.e. training group). The results derived from
the larger training group are then applied to predict the
nodal involvement in the smaller group that was left out
(validation group).
To protect the analysis from random splitting, this
cross-validation was repeated 200 times to conclude the
bias-corrected concordance index (CI) of our database.
Kaplan-Meier method was used to compare the OS
of our patient population. Log-rank test was utilized the
compare the survival results between patient groups based
on the status of their nodal involvement and treatment
modalities. Significance was set at <0.05 throughout the
analysis.
RESULTS
The NCDB reported 340,780 patients with pancreatic
malignancies between 2004-2015. After application of
the inclusion criteria, 9,153 patients were identified to
have non-metastatic PDAC of stages T1-T3, for which
they received R0 surgical resection with a curative intent
and a known number of retrieved and positive nodes.
Of these patients, 6,422 (70.2%) had at least 12 lymph
nodes retrieved during surgery. Table 1 summarizes the
demographics and clinical characteristics of the selected
population.
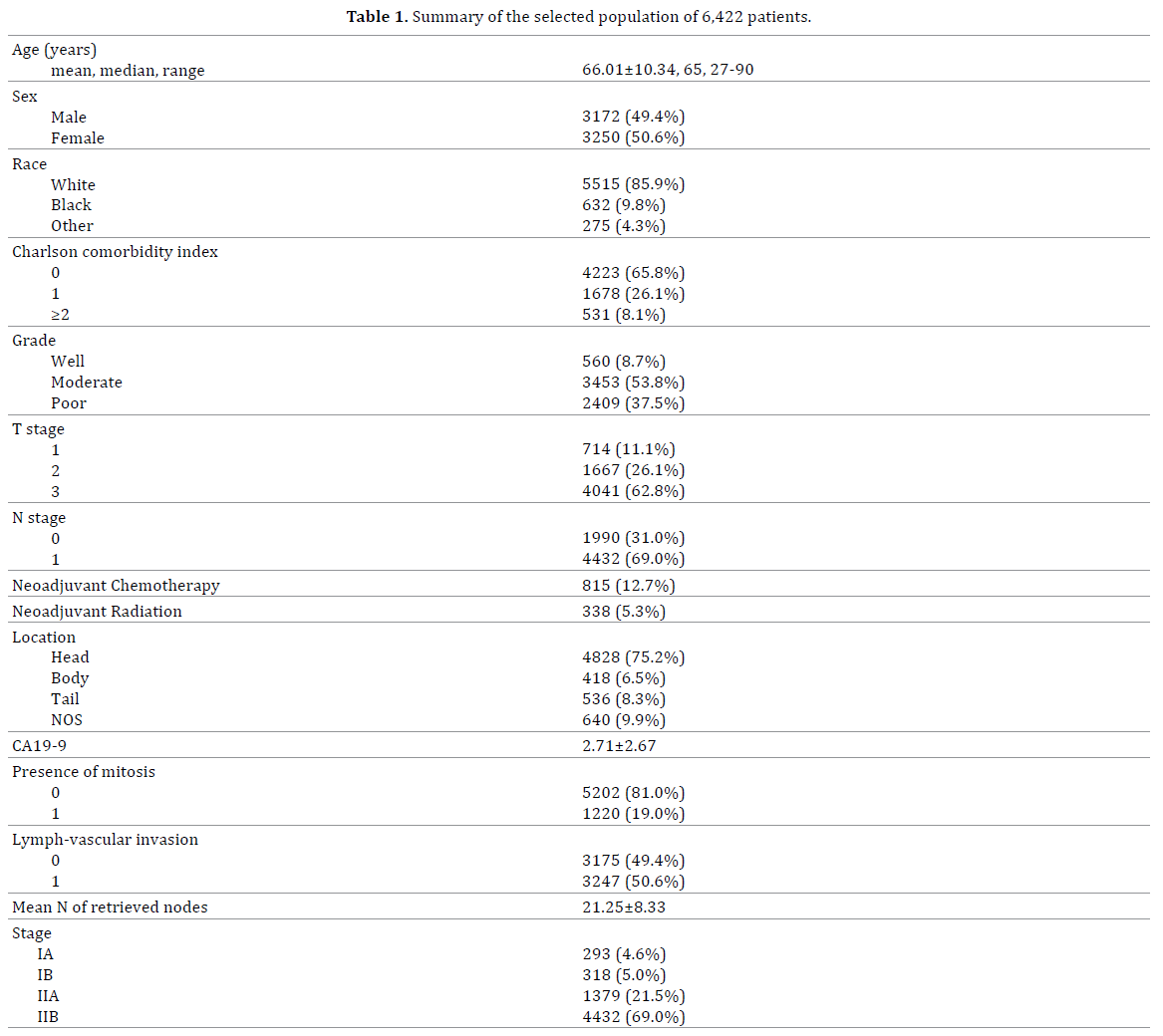
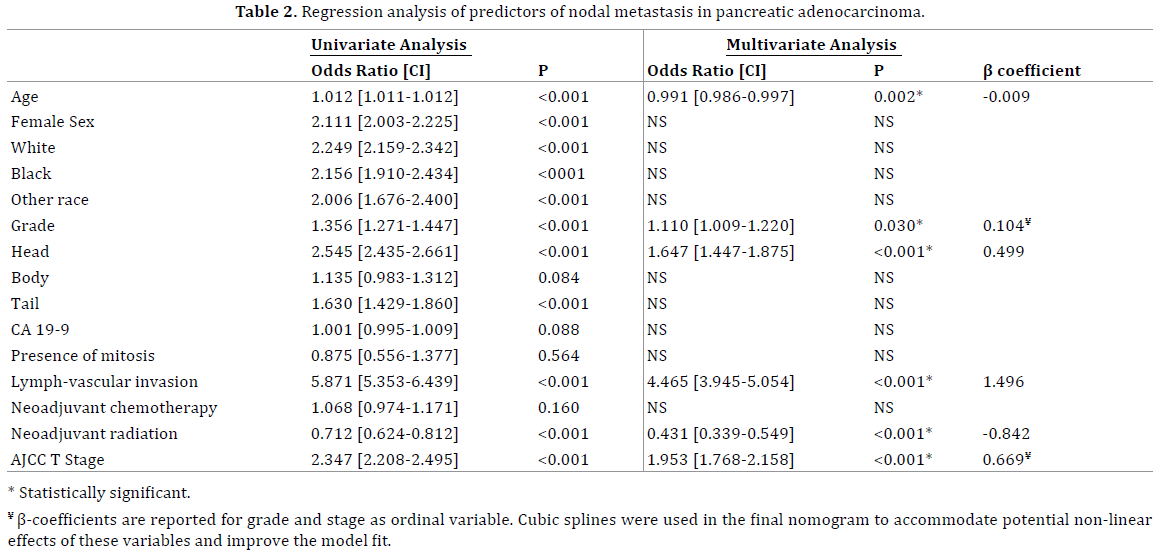
Table 2 demonstrates the results of the binary logistic
regression analysis. Our results show that age, as a
continuous variable, and receiving neoadjuvant radiation
are favorable predictors of nodal involvement, whereas
pancreatic head cancers, lymph-vascular invasion (LVI),
histologic grade, and pathologic T stage represent risk
factors of nodal metastasis. Sex, race, neoadjuvant
chemotherapy, mitotic rate, CA 19-9 and Chromogranin
A (CgA) levels did not demonstrate significant predictive
values. Odds Ratio (OR) with 95% confidence interval
are reported as a parameter of effect size in the logistic
regression model.
Upon calculation of predicted probabilities of nodal
involvement, age was modeled as a continuous variable,
whereas for grade and stage, the ordinal variables in
the model, cubic splines were applied to accommodate
potential non-linear effects of increasing grade or stage
and improve the model fit. The dataset was randomly split
into training and validation subsets as described above;
the training group was used to derive the predictors’
coefficients to be included in the nomogram’s final model, which was then tested for prediction of nodal involvement
in the validation group. The process was repeated 200
times. The bias-corrected CI for the nomogram was
0.756 (95% confidence interval 0.743-0.769; asymptotic
significance <0.001). The Receiver Operating Curve (ROC)
for the nomogram performance is shown in Figure 1A.
Figure 1. (a). Receiver Operating Curve (ROC) for the final nomogram
(Area Under the Curve = 0.756; asymptotic significance <0.0001). (b). Calibration plot comparing the nomogram performance for each decile to
the ideal prediction line.
Calibration of this predictive model was tested. The
dataset was divided into deciles based on the predictive
value of the nomogram for each case. Within each decile,
the predicted outcomes were compared to the observed
outcomes and plotted on the calibration curve shown in Figure 1B. Hosmer-Lemeshow goodness-of-fit test was
conducted on the decile groups and showed no statistical
difference between the observed and expected nodal
involvement (p=0.804).
Based on the final model of the nomogram, a scoring
table was designed which can be used as a tool to calculate
the predicted probability of N1 in any given patient who meets the inclusion criteria of our study. The nomogram
table is shown in Figure 2.
Figure 2. Scoring table for the nomogram.
For cutoff determination, we used the Youden index (J
statistic) to define the optimum of sensitivity and specificity
on the ROC. Our results indicate that the optimal point for a
cutoff is at Youden’s index of 0.394, which correlates with
a predicted probability of 53.40%.
We then used the 2,731 patients who had inadequate
sampling (<12 nodes retrieved) for indirect external
validation of the nomogram. We compared the OS of these
patients based on their predicted nodal status, which was
determined per the aforementioned cutoff, to those who
have a confirmed nodal status from the adequately sampled
patients. Median OS of nomogram-predicted N0 vs. N1
patients was 29.90±1.41vs. 20.57±0.72 months (p<0.001)
which are comparable to those of the adequately sampled
patients. Figures 3A and 3B show the Kaplan-Meier plots
of OS between the predicted N0 and N1 patients.
Figure 3. Kaplan-Meier survival graphs. (a). overall survival in PDAC patients treated with R0 resections and adequate node sampling: median survival of
N0 patients 35.15±1.45 months, N1 patients 21.82±0.44 months; p<0.001. (b). overall survival in PDAC patients treated with R0 resections and inadequate
node sampling: median survival of nomogram-projected N0 patients 29.90±1.41 months, N1 patients 20.57±0.72 months; p<0.001.
DISCUSSION
According to the 7th edition of the AJCC TNM staging,
prognosis of nodal involvement follows a binary system
of N0 vs. N1, where any nodal involvement advances the
stage into IIB at least, with a detrimental regression in
survival and a significantly poorer prognosis.
In this study, we explore the NCDB for PDAC to study
the surgically managed patients with a focus on the
associated lymphadenectomy. Interestingly, the NCDB
reports a remarkable nationwide compliance with the
recommended retrieval of ≥12 nodes during surgical
resection (~70%). These cases of ‘adequate’ lymph node
sampling were used to derive the nomogram assuming
that nodal staging is then accurate.
Our analysis identified a group of clinicopathological
factors that can serve as predictors of nodal involvement;
increasing age and neoadjuvant radiation were favorable
predictors of nodal involvement, whereas head PDAC,
LVI, grade, and T stage were negative prognosticators of
nodal metastasis. Modeling these factors in a predictive
nomogram yielded an AUC of 0.756, which indicates a very
good discrimination, along with acceptable calibration of
the model.
The clinicopathological factors used to build the model
are simple and routinely available for patients undergoing
surgical resections of their PDAC. The inversely
proportional relationship between age and local recurrence
has been demonstrated previously in the Memorial-Sloan
Kettering nomogram [25], hence it would be reasonable to
observe less likelihood of node metastases as patients age
since nodal involvement is a predictor of local recurrence.
Moreover, the logical correlation between LVI, poorer
tumor differentiation, and large tumors (i.e. higher T stage)
and node metastasis has been repeatedly demonstrated
in overall and disease-specific survival predictor models
[25, 26, 27, 28, 29]. Having higher rates of positive nodes
in pancreatic head tumors compared to body/tail tumors is evident for neuroendocrine tumors [30], in accord with
our findings for PDAC, perhaps due to the abundant blood
and lymph supply of the head of the pancreas. The role of
neoadjuvant radiation has been an area of extensive study
for borderline resectable pancreatic tumors; nonetheless,
receiving neoadjuvant radiation has proven to facilitate
higher rates of R0 resection and yield higher rates of N0
staging at final pathology [31]. In our analysis, neither
sex, race, neoadjuvant chemotherapy, nor any of the
conventional tumor markers had a predictive role of nodal
metastasis in PDAC.
We realize that the shortcomings of this study are
several. The retrospective nature of the analysis and using
a national databank have inherent weaknesses including,
but not limited to, inconsistent reporting and missing datapoints which generally lead to exclusion of potentially
important variables in the model. Also, the NCDB reports
the absolute numbers of retrieved and positive nodes
without reporting the nodal stations included in the
lymphadenectomy. In light of the growing evidence on the
prognostic role of para-aortic lymph nodes in PDAC [32, 33, 34], this technical detail becomes of high importance
to improve the function of the model. Most importantly,
the main question that arises is the impact of nodal
status on guiding the decision on adjuvant treatments.
All PDAC patients are recommended to undergo adjuvant
chemotherapy based on randomized trials with variable
regimens [35, 36, 37] regardless of the nodal staging,
whereas the role of adjuvant radiation remains an area
of debate and ongoing research. Our analysis suggests that neoadjuvant radiation reduces the risk of disease
dissemination to the lymph nodes. But if nodal involvement
is evident in that particular case, offering adjuvant
radiation would be out of question.
Nonetheless, we believe that the main value of this
nomogram lies in its ability to better predict the prognosis
of PDAC patients based on readily available factors in
case of inadequate node sampling, a scenario that is not
uncommon. Prognosis stratification in patients with PDAC,
especially in face of uncertain nodal staging, can also play
a critical role in patients’ eligibility for certain ongoing
clinical trials, which might offer a potential of altering the
disease course and prolonging survival in some individuals.
Any nomogram or predictive model entails several
external validations in different patient populations
before concurring its soundness. In our study, the internal
validation was incorporated in the steps of nomogram
development given the relatively satisfactory population
size, in addition to an indirect external validation to the
group of ‘inadequate sampling’ by comparing the survival
or predicted N0 vs. N1 to the confirmed N0 vs. N1, with an
acceptable correlation.
CONCLUSION
Prediction of nodal status in PDAC is critical. Herein,
we establish a nomogram based on clinicopathological
features to predict nodal involvement. This nomogram can
be used to better predict patients’ prognosis following R0
resection of PDAC in light of inadequate nodal sampling.
Adding more variables to the model might increase its
accuracy, bearing in mind the availability of the factors
and the generalizability of its application. Further external
validations are warranted to confirm the accuracy of this
nomogram.
Acknowledgement
We acknowledge Dr. Shaun Dougherty from the
Department of Public Policy at the University of
Connecticut for ensuring the technical soundness of the
statistical analysis.
Conflict of Interest
The authors have no conflicts of interests to declare.
References
- Mortality GBD, Causes of Death C. Global, regional, and national life
expectancy, all-cause mortality, and cause-specific mortality for 249 causes
of death, 1980-2015: a systematic analysis for the Global Burden of Disease
Study 2015. Lancet 2016; 388(10053):1459-544. [PMID: 27733281]
- Hariharan D, Saied A, Kocher HM. Analysis of mortality rates for pancreatic
cancer across the world. HPB(Oxford) 2008; 10:58-62. [PMID: 18695761]
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin
2018; 68:7-30. [PMID: 29313949]
- Bilimoria KY, Bentrem DJ, Ko CY, Stewart AK, Winchester DP,
Talamonti MS, et al. National failure to operate on early stage pancreatic
cancer. Ann Surg 2007; 246:173-80. [PMID: 17667493]
- Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman
J, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: A singleinstitution
experience. J Gastrointest Surg 2006; 10:1199-210; discussion
210-1. [PMID: 17114007]
- Allema JH, Reinders ME, van Gulik TM, Koelemay MJ, Van
Leeuwen DJ, de Wit LT, et al. Prognostic factors for survival after
pancreaticoduodenectomy for patients with carcinoma of the pancreatic
head region. Cancer 1995; 75:2069-76. [PMID: 7697596]
- Lim JE, Chien MW, Earle CC. Prognostic factors following curative resection
for pancreatic adenocarcinoma: a population-based, linked database analysis of
396 patients. Ann Surg 2003; 237:74-85. [PMID: 12496533]
- Pedrazzoli S, DiCarlo V, Dionigi R, Mosca F, Pederzoli P, Pasquali
C, et al. Standard versus extended lymphadenectomy associated with
pancreatoduodenectomy in the surgical treatment of adenocarcinoma of
the head of the pancreas: a multicenter, prospective, randomized study.
Lymphadenectomy Study Group. Ann Surg 1998; 228:508-17. [PMID: 9790340]
- Glanemann M, Shi B, Liang F, Sun XG, Bahra M, Jacob D, et al. Surgical
strategies for treatment of malignant pancreatic tumors: extended, standard
or local surgery? World J Surg Oncol 2008; 6:123. [PMID: 19014474]
- Tol JA, Gouma DJ, Bassi C, Dervenis C, Montorsi M, Adham M, et al.
Definition of a standard lymphadenectomy in surgery for pancreatic
ductal adenocarcinoma: a consensus statement by the International
Study Group on Pancreatic Surgery (ISGPS). Surgery 2014; 156:591-600.
[PMID: 25061003]
- Edge SB, Compton CC. The American Joint Committee on Cancer: the
7th edition of the AJCC cancer staging manual and the future of TNM. Ann
Surg Oncol 2010; 17:1471-4. [PMID: 20180029]
- Huebner M, Kendrick M, Reid-Lombardo KM, Que F, Therneau T, Qin
R, et al. Number of lymph nodes evaluated: prognostic value in pancreatic
adenocarcinoma. J Gastrointest Surg 2012; 16:920-6. [PMID: 22421988]
- Opfermann KJ, Wahlquist AE, Garrett-Mayer E, Shridhar R, Cannick
L, Marshall DT. Adjuvant radiotherapy and lymph node status for
pancreatic cancer: results of a study from the Surveillance, Epidemiology,
and End Results (SEER) Registry Data. Am J Clin Oncol 2014; 37:112-6.
[PMID: 23211221]
- Robinson SM, Rahman A, Haugk B, French JJ, Manas DM, Jaques BC,
et al. Metastatic lymph node ratio as an important prognostic factor in
pancreatic ductal adenocarcinoma. Eur J Surg Oncol 2012; 38:333-9.
[PMID: 22317758]
- Sierzega M, Popiela T, Kulig J, Nowak K. The ratio of metastatic/
resected lymph nodes is an independent prognostic factor in patients
with node-positive pancreatic head cancer. Pancreas 2006; 33:240-5.
[PMID: 17003644]
- Schwarz RE, Smith DD. Extent of lymph node retrieval and pancreatic
cancer survival: information from a large US population database. Ann
Surg Oncol 2006; 13:1189-200. [PMID: 16955385]
- House MG, Gonen M, Jarnagin WR, D'Angelica M, DeMatteo RP, Fong Y, et
al. Prognostic significance of pathologic nodal status in patients with resected
pancreatic cancer. J Gastrointest Surg 2007; 11:1549-55. [PMID: 17786531]
- Mirkin KA, Hollenbeak CS, Wong J. Greater lymph node retrieval and
lymph node ratio impacts survival in resected pancreatic cancer. J Surg
Res 2017; 220:12-24. [PMID: 29180173]
- Elshaer M, Gravante G, Kosmin M, Riaz A, Al-Bahrani A. A systematic
review of the prognostic value of lymph node ratio, number of positive
nodes and total nodes examined in pancreatic ductal adenocarcinoma.
Ann R Coll Surg Engl 2017; 99:101-6. [PMID: 27869496]
- Yeo CJ, Cameron JL, Sohn TA, Coleman J, Sauter PK, Hruban RH, et
al. Pancreaticoduodenectomy with or without extended retroperitoneal
lymphadenectomy for periampullary adenocarcinoma: comparison
of morbidity and mortality and short-term outcome. Ann Surg 1999;
229:613-22; discussion 22-4. [PMID: 10235519]
- Yeo CJ, Cameron JL, Lillemoe KD, Sohn TA, Campbell KA, Sauter PK,
et al. Pancreaticoduodenectomy with or without distal gastrectomy
and extended retroperitoneal lymphadenectomy for periampullary
adenocarcinoma, part 2: randomized controlled trial evaluating survival,
morbidity, and mortality. Ann Surg 2002; 236:355-66; discussion 66-8.
[PMID: 12192322]
- Sun J, Yang Y, Wang X, Yu Z, Zhang T, Song J, et al. Meta-analysis of the
efficacies of extended and standard pancreatoduodenectomy for ductal
adenocarcinoma of the head of the pancreas. World J Surg 2014; 38:2708-
15. [PMID: 24912627]
- Michalski CW, Kleeff J, Wente MN, Diener MK, Büchler MW, Friess
H, et al. Systematic review and meta-analysis of standard and extended
lymphadenectomy in pancreaticoduodenectomy for pancreatic cancer.
Br J Surg 2007; 94:265-73. [PMID: 17318801]
- Nimura Y, Nagino M, Takao S, Takada T, Miyazaki K, Kawarada
Y, et al. Standard versus extended lymphadenectomy in radical
pancreatoduodenectomy for ductal adenocarcinoma of the head of the
pancreas: long-term results of a Japanese multicenter randomized controlled
trial. J Hepatobiliary Pancreat Sci 2012; 19:230-41. [PMID: 22038501]
- Ferrone CR, Kattan MW, Tomlinson JS, Thayer SP, Brennan MF,
Warshaw AL. Validation of a postresection pancreatic adenocarcinoma
nomogram for disease-specific survival. J Clin Oncol 2005; 23:7529-35.
[PMID: 16234519]
- Hsu CC, Wolfgang CL, Laheru DA, Pawlik TM, Swartz MJ, Winter JM,
et al. Early mortality risk score: identification of poor outcomes following
upfront surgery for resectable pancreatic cancer. J Gastrointest Surg
2012; 16:753-61. [PMID: 22311282]
- Botsis T, Anagnostou VK, Hartvigsen G, Hripcsak G, Weng C. Modeling
prognostic factors in resectable pancreatic adenocarcinomas. Cancer
Inform 2010; 7:281-91. [PMID: 20508721]
- Hartwig W, Hackert T, Hinz U, Gluth A, Bergmann F, Strobel O, et al.
Pancreatic cancer surgery in the new millennium: better prediction of
outcome. Ann Surg 2011; 254:311-9. [PMID: 21606835]
- Groot VP, Gemenetzis G, Blair AB, Rivero-Soto RJ, Yu J, Javed AA, et al.
Defining and Predicting Early Recurrence in 957 Patients With Resected
Pancreatic Ductal Adenocarcinoma. Ann Surg 2018. [PMID: 29578908]
- Hashim YM, Trinkaus KM, Linehan DC, et al. Regional lymphadenectomy
is indicated in the surgical treatment of pancreatic neuroendocrine tumors
(PNETs). Ann Surg 2014; 259:197-203. [PMID: 24253141]
- Breslin TM, Hess KR, Harbison DB, Jean ME, Cleary KR, Dackiw AP, et
al. Neoadjuvant chemoradiotherapy for adenocarcinoma of the pancreas:
treatment variables and survival duration. Ann Surg Oncol 2001; 8:123-
32. [PMID: 11258776]
- Paiella S, Malleo G, Maggino L, Bassi C, Salvia R, Butturini G. et al.
Pancreatectomy with Para-Aortic Lymph Node Dissection for Pancreatic
Head Adenocarcinoma: Pattern of Nodal Metastasis Spread and
Analysis of Prognostic Factors. J Gastrointest Surg 2015; 19:1610-20.
[PMID: 26160322]
- Paiella S, Sandini M, Gianotti L, et al. The prognostic impact of paraaortic
lymph node metastasis in pancreatic cancer: A systematic review
and meta-analysis. Eur J Surg Oncol 2016; 42:616-24. [PMID: 26916137]
- Agalianos C, Gouvas N, Papaparaskeva K, Dervenis C. Positive paraaortic
lymph nodes following pancreatectomy for pancreatic cancer.
Systematic review and meta-analysis of impact on short term survival
and association with clinicopathologic features. HPB (Oxford) 2016;
18:633-41. [PMID: 27485057]
- Oettle H, Neuhaus P, Hochhaus A, Hartmann JT, Gellert K, Ridwelski K,
et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes
among patients with resected pancreatic cancer: the CONKO-001
randomized trial. JAMA 2013; 310:1473-81. [PMID: 24104372]
- Regine WF, Winter KA, Abrams R, Safran H, Hoffman JP, Konski A,
et al. Fluorouracil-based chemoradiation with either gemcitabine or
fluorouracil chemotherapy after resection of pancreatic adenocarcinoma:
5-year analysis of the U.S. Intergroup/RTOG 9704 phase III trial. Ann Surg
Oncol 2011; 18:1319-26. [PMID: 21499862]
- Neoptolemos JP, Moore MJ, Cox TF, Valle JW, Palmer DH, McDonald
AC, et al. Effect of adjuvant chemotherapy with fluorouracil plus folinic
acid or gemcitabine vs observation on survival in patients with resected
periampullary adenocarcinoma: the ESPAC-3 periampullary cancer
randomized trial. JAMA 2012; 308:147-56. [PMID: 22782416]




