Keywords
Control Studies; Laparoscopy; Pancreatectomy
INTRODUCTION
Minimally invasive techniques provide surgeons with the option of a laparoscopic approach for benign and borderline tumors in the distal pancreas [1]. The laparoscopic approach of left side pancreatic resection has gained popularity since the first case reported more than 20 years ago by Cuschieri et al. [2], because of its reproducibility, absence of complex reconstruction, and the traditional benefits of a minimally invasive procedure such as reduced pain and rapid recovery. However, laparoscopic surgery has shortcomings, including limited two-dimensional views and instrument maneuverability, fixed instrument tips, and possible hand and instrument misalignment. Given these limitations, spleen preservation is challenging because of the difficulties in effectively controlling bleeding from the splenic vessels during dissection. Usually concomitant en bloc splenectomy is performed for the sake of technical simplicity making resection easier, shortening operative time (OT), and reducing blood loss [3]. Therefore, especially in the hands of non-experienced surgeons, a laparoscopic approach is often associated with a high risk of conversion to handassisted laparoscopic surgery (HALS), open surgery, or spleen sacrifice [4]. It has been well accepted that function-preserving surgery is thought to be an optimal approach in case of oncological safety. In particular, patients with benign pancreatic tumors can develop critical post-splenectomy infections even many years after surgery, confirming the need to preserve the spleen whenever indicated [5]. Moreover, the rule of the spleen has gradually become recognized in developing cancer or cardiovascular disease.
The Da Vinci surgical system (Intuitive Surgical, Sunnyvale, California, USA) in this setting has been theoretically indicated for overcoming some drawbacks of standard laparoscopy. This system translates the surgeon’s hand movements into corresponding instrument delicate micro-movements within narrow spaces. Giulianotti et al. [6] reported the first case of robotic-assisted (RA) pancreatic surgery and since then over two hundred cases of RA distal pancreatectomy have been reported. However, there are few reports [7-12] about robotic spleen-preserving left sided pancreatectomy (R-SPLP) and few comparative studies between the two approaches. In the present study, we compare the peri-operative and midterm functional aspects of R-SPLP versus L-SPLP in a casematched comparison.
PATIENTS AND METHODS
Between January 2010 and June 2014, 15 patients with benign tumors of the body and tail of the pancreas underwent R-SPLP at the first General Surgery Unit, University of Pisa. Selection criteria for R-SPLP were: no history of previous major, open, upper abdominal surgery, no general medical conditions that would limit prolonged anesthesia with concurrent carbon dioxide pneumoperitoneum, body mass index not exceeding 35 kg/m2, and preoperative imaging consistent with a nonmalignant tumor or suspected malignant tumor without suspected involvement of splenic vessels. A control group of patients undergoing laparoscopic spleen-preserving left-sided pancreatectomy (L-SPLP), who met the inclusion criteria for R-SPLP was randomly selected from the pool of patients available in a prospectively maintained Institutional Review Board-approved pancreatic neoplasms database in our department. Patients were selected using a case-matched methodology where each patient in the R-SPLP group was matched with one of the L-SPLP group according to the following matching criteria: age, gender, body mass index (BMI), American Society of Anesthesiologists score (ASA), and imaging tumor size. The preoperative work-up included abdominal ultrasonography, chest radiography, abdomen CT scan and/or magnetic resonance imaging.
Patients were considered for RA approach based on robot availability. All operations were performed by two surgeons (LM and AP), both with substantial experience in minimally invasive surgery.
Peri-operative data including operative time, estimated blood loss, need for blood transfusions, rate of conversion were collected. Cumulative spleen and splenic vessels preservation rate, first liquid diet received, hospital length of stay, and morbidity were noted and evaluated. Morbidity data included postoperative complications such as intraabdominal fluid collection, wound infection, pancreatic fistula, bowel obstruction, pulmonary or urinary tract infections and 90-day hospital readmissions. Post operative complications were graded using the Clavien- Dindo classification [13]. Pancreatic fistula was defined and classified by International Study Group on Pancreatic Surgery criteria [14].
After discharge, patients were followed up every six months with a physical examination, blood work, and diagnostic ultrasound during the first postoperative year. All the patients considered eligible for this case matched study had at least a 1 year follow-up period, and were retrospectively interviewed in order to evaluate the impact of minimally invasive SPLP on QoL, using the EORTC QLQ-C30 questionnaire [15]. This questionnaire assesses global health and functional status, where higher scores indicate better quality of life, and evaluates symptoms related to overall and psychological health and gastrointestinal function, in which lower scores are desirable. For the purpose of this study, the last follow up was scheduled in June 2015.
Technical Notes
Spleen preservation was pursued according the splenic vessel conservation technique described by Kimura et al [16]. Parenchymal transection and closure was carried out using electrocautery and the stump was oversewn with intracorporeal knotting or with an endostapler.
Laparoscopic SPLP: Patients were placed in the supine or left sided position, dependent upon the tumor site, with both arms along the sides of the body and tilted in partial reverse Trendelenburg position. Four/five ports were used (4, 5 mm; 1, 12 mm). After the placement of ports and the establishment of pneumoperitoneum, an exploration of the abdomen was performed. The lesser sac then was entered (through greater gastrocolic omentum). The splenic flexure of the colon was mobilized if necessary. An intra-operative diagnostic ultrasound with laparoscopic probe was always performed in order to evaluate the pancreatic lesion and its correct position. The superior and inferior borders of the pancreas were defined, and splenic vessels were identified and preserved. The gland was mobilized and then transected using a stapler (ETS Flex 45 Endoscopic Articulating Staple, Johnson & Johnson, USA). Two drains were left near the pancreatic stump.
Robotic SPLP:All procedures were performed using the Da Vinci Si system. For this approach, a five-port technique was used. Patient position was similar to that of the L-SPLP. The robot was placed in front of the patient’s head. The camera arm was docked to the corresponding trocar, and a robotic three-dimensional (3D) high-definition laparoscope was inserted. Three robotic arms were docked and robotic instruments were mounted. For dissection and retraction monopolar scissor and Cadier grasper were used. Energy robotic devices were Gyrus PK SuperPulse.Generetor (Olympus, Center Valley, PA, USA) or Maryland bipolar forceps (Intuitive Surgical, Sunnyvale, California, USA). The assistant’s trocar was then inserted and used for suture insertion or suction. The surgical steps were similar to the laparoscopic approach. The pancreas was divided with robotic monopolar curved scissors and then with the forth arm the body of the pancreas was pulled up in order to expose the posterior attachments of the organ. The special pulse-modulating robotic device (PK™) or the Maryland bipolar forceps were used to seal all small tributary splenic vessels. The remnant pancreatic stump was predominantly oversewn with 4 or 5 interrupted sutures using robotic needle drivers with selective ligation of Wirsung duct. In case of thickness of the pancreas, the parenchyma was transected with an endostapler. Once the gland was divided and fully free from the attachments, the robot was undocked, and the specimen was placed in a plastic bag for extraction laparoscopically through a suprapubic incision. Two drains were left near the pancreatic stump.
Statistical Analysis
Variables of interest were analyzed retrospectively after Institutional Review Board approval. Sample characteristics were assessed using descriptive statistics. Categorical variables are expressed as percentages. Comparison of pre-operative characteristics for L-SPLP and R-SPLP was performed using an independent T test for continuous data and Chi-squared or Fisher’s exact test for categorical data. With the aim to evaluate the outcomes of the two surgical treatments, binary logistic models were performed. Results are reported as odds ratios (OR) with a 95 % confidence interval (adjusted for sex and age). We defined as a dependent variable the “surgical approach” (1= L-SPLP; 0= R-SPLP) and as independent variables the peri and post-operative events: operative time as a continuous variable (minutes); length of hospital stay as a continuous variable (Days); post operative complications (0= absence of complication; 1= complication); Fistula (0= absence of fistula; 1= fistula); Splenectomy (0= absence of splenectomy; 1= splenectomy). A t test for two independent populations was performed to compare the global health status/QoL total score test between groups (L-SPLP and R-SPLP). Comparison of the global health status/QoL total score and QoL subscales in L-SPLP and R-SPLP, repeated measure analysis of variance (rm-ANOVA) models and post-hoc tests (Bonferroni) were performed. The statistical package SPSS® Version 17 (SPSS Inc., Chicago, IL, USA) was used for the analysis.
RESULTS
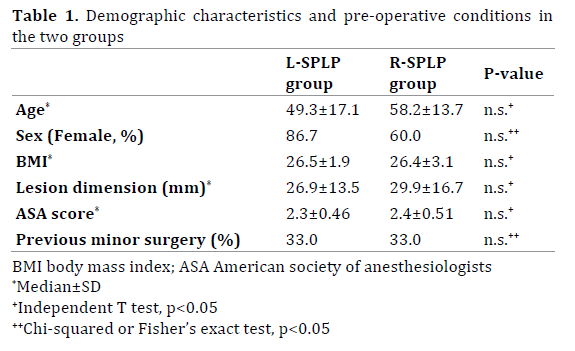
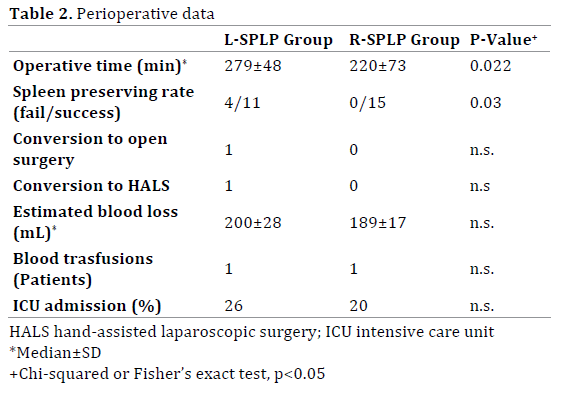
Demographic characteristics and pre-operative conditions, without significant differences between the two groups, are shown in Table 1. In the R-SPLP group there were no conversion to conventional laparoscopy, hand-assisted laparoscopy surgery (HALS) or open surgery. Conversion to open surgery occurred in one L-SPLP patient and conversion to HALS occurred in another L-SPLP patient (for a conversion rate of 13.3% vs. 0% in R-SPLP; p=n.s.). The spleen-preserving rate of the R-SPLP group was superior to that of the L-SPLP group (fail/success, 0/15 vs. 4/11, p=0.03, Fischer’s exact test; <0.05). Operative time was somewhat longer in the L-SPLP group when compared to the R-SPLP group (220±73 vs. 279±48 min; p=0.027). This significant time difference was still observed when only cases of successful SPLP were considered and converted cohort was excluded in both groups (220±73 vs. 276±54 min, p=0.04). Estimated blood loss (189±17 vs. 200±28 ml; p=n.s.) and rate of intensive care unit admission (20% vs. 26%; p=n.s.) was similar between groups. Patients undergoing R-SPLP received their first liquid diets (2.8±0,9 vs.4,3±1,3 days; p=0.03) and full oral diets (4.2±1.0 vs.5.8±1.8 days; p=0.01) sooner than patients undergoing L-SPLP Table 2. The mean hospital stay was 6.5±1.9 days for patients in the R-SPLP group and 8.8±3.8 days for patients in the L-SPLP group (p=0.04).
No high grade, Clavien-Dindo complications were recorded after R-SPLP. Only one patient in the L-SPLP group required ultrasound guided percutaneous catheter drainage to drain a fluid collection, Clavien-Dindo grade IIIA (complications rate 6.6% vs. 0%; p=n.s.). Pancreatic fistulas occurred in 7 patients in the L-SPLP group (46% of total). Four were graded A and three graded B. In the R-SPLP group, pancreatic fistula developed in 3 cases (20% of total): two were graded A and one graded B; there were no grade C fistulas. No significant differences were noted in the overall pancreatic fistula rate between the two study groups (46% vs. 20%; p=n.s.). The other post-operative and pathology results are summarized in Table 2. The 30-day mortality rate was zero. No blood transfusions, re-admissions or repeated surgery were observed in our series. The multivariate analysis (binary logistic model) shows association between single covariates and two surgical treatments Table 3. Operative time (OR: 1.018 [IC95% 1.001-1.035]) and length of hospital stay (OR: 1.686 [IC95% 1.050-2.708]) were longer in the L-SPLP. The probability of incurring postoperative complications and fistula was the same for the two types of treatment.

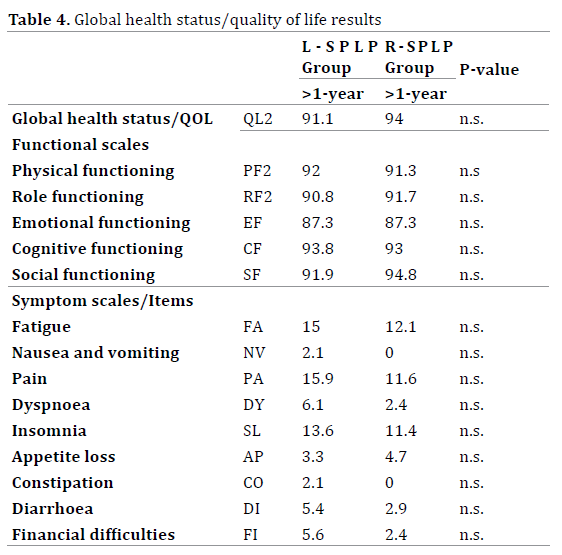
Repeated measure ANOVA comparing QoL total score and QoL subscales after at least 1 year indicated for both groups the same significant effect on time. Following surgery, for both techniques, the global health status score was over 90 points after one year (R-SPLP; >1 year 94/ L-SPLP; >1 year 91.1). Similar good values were observed for the physical functioning subscale, role functioning subscale, emotional functioning subscale and for the symptom scales (fatigue, pain, insomnia, appetite loss). For the cognitive functioning and social functioning subscale and for nausea and vomiting, dyspnea, constipation, diarrhea, and financial difficulties, Bonferroni post-hoc correction did not detect a significant different trend Table 4.
DISCUSSION
During spleen-preserving left pancreatectomy, a fine and delicate laparoscopic technique is required because even a small break in the tributary vessels from the splenic artery and vein can potentially obscure the surgical field, which might result in intra-operative bleeding subsequently resulting in splenectomy or requiring conversion to open approach to control of hemorrhage. In fact, in a large series, some investigators have showed a conversion rate up to 30% during L-SPLP [17] and recent meta-analyses have demonstrated that the rate of conversion to HALS was 37% and that from laparoscopy to open procedure range from 9% to 11% with significantly higher post-operative complications among patients requiring conversion [18]. About spleen sacrifice, a multicenter comparison reported a spleen preservation rate of only 30% during L-SPLP [19].
Robotic assistance facilitates surgical plane manipulation and fine dissection, and good results have been reported in previous studies of R-SPLP in terms of spleen preservation, conversion rate, operative time and length of hospital stay [8-11]. Furthermore, Waters et al [7] showed that the higher intra-operative costs of robotic technology due to the longer operative times were offset by a shorter hospital stay. In a recent structured matched cohort study, Chen and colleagues [12] have demonstrated that robotic assistance in left side pancreatectomy increased the chances of spleen preservation and offered real benefits such as faster recovery and reduced operative time and blood loss
The present study confirmed a shorter operative time and hospital stay with lower risk of spleen sacrifice in the R-SPLP group, even though laparoscopic were the older cases, the differences could be partly related to a learning curve. Conversion rate was lower in R-SPLP although not statistically significant. The other data were equivalent suggesting that robotic assistance is a suitable technique based on surgical cure. We believe that by retaining wristlike movements of the effector instruments, the surgeon during R-SPLP can bluntly dissect the body of the pancreas and identify the pedicle of the spleen early in the dissection. The use of special robotic devices (PK™ or Maryland bipolar force) can be an advantage when performing very fine surgery such as dissecting the small branches of the splenic artery and applying bipolar energy precisely. Moreover, by using a stable camera and filtered tremor provided by a Da Vinci system we were able to identify and securely ligate even a small breakage of tributary vessels using a robot-assisted suturing technique. With the aid of robot assistance, this surgical phase is facilitated and can be accomplished in a faster and safer manner, resulting in a high rate of spleen preservation. In R-SPLP fine dissection of posterior attachments of the pancreas to the retroperitoneal space can usually be accomplished even in circumstances of limited space by laparoscopic straight instruments because of 7° degrees of freedom with a robotic technique. Suturing the main pancreatic duct with the sole assistance of pure laparoscopy is not only complex because of the restricted view and limited mobility but also has the risk of breaking the capsule of the pancreas [20]. The enhanced operative abilities of the robotic system may allow surgeons to perform such complex surgical maneuvers safety and in a more natural manner, further reducing the time needed for this step of the procedure.
Some studies have shown that use of a surgical microscope and robot assistance may decrease the incidence of pancreatic fistula after pancreatectomy [21, 22]. The Da Vinci system offers a stereoscopic highdefinition view with image magnification up to ×15, tremor filtration and scaled motion that translates larger movements of the surgeon’s hand into finer movements of the wristed instruments. These technical improvements would seem ideal for reducing the rate of clinically significant pancreatic fistulas after R-SPLP. In our practice during robotic procedures, when possible we prefer using cautery scissors with anterior-to-posterior pancreatic resection, suture or ligate selectively the main duct and close the pancreatic gland with stitches. A stapler device was used three times during robotic procedures due to thickness of parenchyma as suggested by Eguchi et al [23] in their retrospective series. There were no grade C fistulas and only 1 grade B in our 15 robotic surgical procedures, also in cases with soft gland and small ducts, with better results over standard laparoscopy although not statistically significant.
Another objective of our study was to to quantify the impact of different surgical techniques on QoL after spleen-preserving left side pancreatectomy. This theme remained largely overlooked in the literature even if some studies have dealt with QoL and long-term symptoms after pancreatic surgery in a specific setting [24-26]. In our experience the QoL scores do not show differences among patients in R-SPLP and L-SPLP groups. However, other studies demonstrated that, during minimally invasive left side pancreatectomy, spleen sacrifice and conversion to open surgery were associated with long term disadvantages such as poor diabetes control, vulnerability to infection and poor general health condition [27]. We were not able to confirm these findings although in the L-SPLP group a higher percentage of conversion and spleen sacrifice was observed; this may partially reflect the small sample of our study. However spleen preservation is advised for its known benefits related to severe infections, risks of thromboembolism and cancer [28]. Quite interesting the score at 12 months in both arms was not different from that in the general population [29]. In fact, the vast majority of our patients did not experience situations requiring clinical treatment or functional impairment and certainly, overcoming an operation makes them more hopeful, resulting in high social and emotional scores. These data also suggest that minimally invasive left side pancreatectomy, performed either laparoscopically or robotically, has a low impact on mid term quality of life.
We believe that robotic assistance could provide advantages over laparoscopy in this particular type of procedure in which fine and delicate dissection is required. Some peri-operative aspects like operative time and hospital length of stay seem to be in favor of R-SPLP group. Moreover, we have confirmed that the robotic approach has other positive aspects in this setting such as higher spleen preservation and lower conversion rate, even if not statistically significant. The main limiting factors of the present work are the small sample size and the fact that it is retrospective and not randomized, so to some degree a certain amount of bias exists and the statistical power is not very high. Another drawback is that we were not able to accurately estimate the additional costs of robotic assistance. Even if an economical study comparing the whole process would be interesting, it is reasonable to assume that direct operative costs were increased compared with pure laparoscopy. However, in other operations in which functional results are key for quality of life and may be rewarding in terms of indirect costs [30], robotic assistance has found one of its main fields of use. Diabetes mellitus, long term QoL, spleen preservation are important factors that should be taken into consideration when costs are evaluated during left side pancreatectomy.
Due to all these limitations no definitive conclusions can be drawn up and a meaningful evaluation of this difficult issue deserves specific studies with well defined outcome measures, clearly identified comparative treatments, and exact definition of direct and indirect costs.
Acknowledgement
Study supported by ARPA foundation. www. fondazionearpa.it
Author contributions
Study concept and design: Morelli, Guadagni, Di Franco, Palmeri, Di Candio and Mosca. Acquisition of data: Morelli, Guadagni, Caprili, D’Isidoro, Di Franco, Pietrabissa and Palmeri. Analysis and interpretation of data: Bastiani, Morelli, Di Candio and Mosca. Drafting of the manuscript: Morelli, Guadagni and Palmeri. Critical revision of the manuscript for important intellectual content: Morelli, Di Candio, Pietrabissa and Mosca. Final approval of the version to be published: Morelli, Guadagni, Palmeri, Di Franco, Bastiani, Di Candio, Pietrabissa and Mosca
Conflicts of Interest
The authors have no conflicts of interest or financial ties to disclose
References
- Song KB, Kim SC, Park JB, Kim YH, Jung YS, Kim MH, Lee SK, et al. Single-center experience of laparoscopic left pancreatic resection in 359 consecutive patients: changing the surgical paradigm of left pancreatic resection. SurgEndosc 2011; 25:3364–3372. [PMID: 21556993]
- Cuschieri A, Jakimowicz JJ, van Spreeuwel J. Laparoscopic distal 70% pancreatectomy and splenectomy for chronic pancreatitis. Ann Surg 1996; 223:280–285. [PMIC: 1235116]
- Yoon YS, Lee KH, Han HS, Cho JY, Ahn KS. Patency of splenic vessels after laparoscopic spleen and splenic vessel-preserving distal pancreatectomy. Br J Surg 2009; 96:633–640. [PMID: 19434700]
- Nigri GR, Rosman AS, Petrucciani N, Fancellu A, Pisano M, Zorcolo L, Ramacciato G, Melis M. Meta-analysis of trials comparing minimally invasive and open distal pancreatectomies. SurgEndosc 2011; 25:1642-1651. [PMID: 21184115]
- Dalla Bona E, Beltrame V, Liessi F, Sperti C. Fatal pneumococcal sepsis eleven years after distal pancreatectomy with splenectomy for pancreatic cancer. JOP 2012; 13:693–695. [PMID: 23183404]
- Giulianotti PC, Coratti A, Angelini M et al. Robotics in general surgery: personal experience in a large community hospital. Arch Surg 2003; 138:777–784. [PMID: 12860761]
- Waters JA, Canal DF, Wiebke EA, Dumas RP, Beane JD, Aguilar-Saavedra JR, Ball CG, et al. Robotic distal pancreatectomy: cost effective? Surgery 2010; 148:814–823. [PMID: 20797748]
- Kang CM, Kim DH, Lee WJ, Chi HS. Conventional laparoscopic and robot-assisted spleen-preserving pancreatectomy: does Da Vinci have clinical advantages? SurgEndosc 2011; 25:2004–2009. [PMID: 21136089]
- Hwang HK, Kang CM, Chung YE, Kim KA, Choi SH, Lee WJ. Robot-assisted spleen-preserving distal pancreatectomy: a single surgeon's experiences and proposal of clinical application. SurgEndosc 2013; 27:774-81. [PMID: 23052527]
- Daouadi M, Zureikat AH, Zenati MS, Choudry H, Tsung A, Bartlett DL, Hughes SJ, et al. Robot-assisted minimally invasive distal pancreatectomy is superior to the laparoscopic technique. Ann Surg 2013; 257:128–132. [PMID: 22868357]
- Butturini G, Damoli I, Crepaz L, Malleo G, Marchegiani G, Daskalaki D, Esposito A, et al. A prospective non-randomised single-center study comparing laparoscopic and robotic distal pancreatectomy. SurgEndosc 2015. [PMID: 25552231]
- Chen S, Zhan Q, Chen JZ, Jin JB, Deng XX, Chen H, Shen BY, et al. Robotic approach improves spleen-preserving rate and shortens postoperative hospital stay of laparoscopic distal pancreatectomy: a matched cohort study. SurgEndosc 2015. [PMID: 25791063]
- Daniel D, Nicolas D, Pierre-Alain C. Classification of Surgical Complications A New Proposal with Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann Surg 2004; 240: 205–213. [PMID: 15273542]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, et al. Postoperative pancreatic fistula: an International Study Group (ISGPF) definition. Surgery 2005; 138:8. [PMID: 16003309]
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, et al. The European Organisation for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. Journal of the National Cancer Institute 1993; 85: 365-376. [PMID: 8433390]
- Kimura W, Inoue T, Futakawa N et al. Spleen-preserving distal pancreatectomy with conservation of the splenic artery and vein. Surgery 1996; 120:885–890. [PMID: 8909526]
- Jayaraman S, Gonen M, Brennan MF, D'Angelica MI, DeMatteo RP, Fong Y, Jarnagin WR, Allen PJ. Laparoscopic distal pancreatectomy: evolution of a technique at a single institution. J Am CollSurg 2010; 211:503-509. [PMID: 20868976]
- Borja-Cacho D, Al-Refaie WB, Vickers SM, Tuttle TM, Jensen EH. Laparoscopic distal pancreatectomy. J Am CollSurg 2009; 209:758-765. [PMID: 19959046]
- Kooby DA, Gillespie T, Bentrem D, Nakeeb A, Schmidt MC, Merchant NB, Parikh AA, et al. Left-sided pancreatectomy: a multicenter comparison of laparoscopic and open approaches. Ann Surg 2008; 248:438-446. [PMID: 18791364]
- Weber SM, Cho CS, Merchant N, Pinchot S, Rettammel R, Nakeeb A, et al. Laparoscopic left pancreatectomy: complication risk score correlates with morbidity and risk for pancreatic fistula. Ann SurgOncol 2009; 16:2825-2833. [PMID: 19609621]
- Hashimoto Y, Traverso LW. Pancreatic anastomotic failure rate after pancreaticoduodenectomy decreases with microsurgery. J Am CollSurg 2010; 211:510–521. [PMID: 20801693]
- Boggi U, Amorese G, Vistoli F, Caniglia F, De Lio N, Perrone V, Barbarello L, et al. Laparoscopic pancreaticoduodenectomy: a systematic literature review. Surg Endosc 2015; 29:9-23. [PMID: 25125092]
- Eguchi H, Nagano H, Tanemura M, Takeda Y, Marubashi S, Kobayashi S, Wada H, et al. A thick pancreas is a risk factor for pancreatic fistula after a distal pancreatectomy: selection of the closure technique according to the thickness. Dig Surg 2011; 28:50-6. [PMID: 21293132]
- Evans JD, Wilson PD, Carver C, Bramhall SR, Buckels JAC, Mayer AD, et al. Outcome of surgery for chronic pancreatitis. Br J Surg 1997; 84: 624-629. [PMID: 9171747]
- Andersson B, PendseML, Andersson R. Pancreatic function, quality of life and costs at long-term follow-up after acute pancreatitis. World J Gastroenterol 2010; 16: 4944–4951. [PMIC: 2957603]
- Park JW, Jang JY, Kim EJ, Kang MJ, Kwon W, Chang YR, Han IW, Kim SW. Effects of pancreatectomy on nutritional state, pancreatic function and quality of life. Br J Surg 2013; 100:1064-1070. [PMID: 23616030]
- Tang CW, Feng WM, Bao Y, Fei MY, Tao YL. Spleen-preserving distal pancreatectomy or distal pancreatectomy with splenectomy?: Perioperative and patient-reported outcome analysis. J ClinGastroenterol 2014; 48:62-66. [PMID: 24231937]
- Kristinsson S, Gridley G, Hoover RN, Check D, Landgren O. Long-term risks after splenectomy among 8,149 cancer-free American veterans: a cohort study with up to 27 years follow-up. Haematologica 2014; 99:392-398. [PMID: 24056815]
- Schwarz R, Hinz A. Reference data for the quality of life questionnaire EORTC QLQ-C30 in the general German population. Eur J Cancer 2001; 37: 1345–1351. [PMID: 11435063]
- Geraerts I, Van Poppel H, Devoogdt N, Van Cleynenbreugel B, Joniau S, Van Kampen M. Prospective evaluation of urinary incontinence, voiding symptoms and quality of life after open and robot-assisted radical prostatectomy. BJU Int 2013; 112:936-943. [PMID: 23937206]

