Keywords
Ischemic heart failure; NYHA IV; Sacubitril/valsartan; Acute coronary syndrome
Abbreviations
ACE: Angiotensin Converting Enzyme; DES: Drug Eluting Stent; HFrEF: Heart Failure with Reduced Ejection Fraction; ICD: Implantable Cardioverter Defibrillator; LAD: Left Anterior Descending; LCx: Left Circumflex; LVEF: Left Ventricular Ejection Fraction; NSVT: Non-Sustained Ventricular tachycardia; NYHA: New York Heart Association functional classification; PCI: Percutaneous Coronary Intervention; RCA: Right Coronary Artery; STEMI: ST-segment Elevation Myocardial Infarction
Introduction
The combination of sacubitril/valsartan has proven superior to enalapril administration in patients with chronic heart failure with reduced ejection fraction (HFrEF), in terms of mortality rates and heart failure hospitalizations in the PARADIGM-HF randomized trial [1]. Data from this randomized trial led to the replacement of angiotensin converting enzyme (ACE) inhibitors with the combination of sacubitril/valsartan in HFrEF patients who are already on ACE inhibitors and remain symptomatic, according to the 2016 HFrEF ESC and 2017 ACC/AHA guidelines [2,3]. In this case report, we describe our own experience on the remarkable clinical recovery of a patient with known ischemic HFrEF and a recent acute coronary syndrome, right after the replacement of the ACE inhibitor with the sacubitril/valsartan combination.
Case Report
A 55-year old male with a past medical history of known ischemic heart failure, ejection fraction of 30-35% and poor adherence to his medical treatment, was transported from a secondary provincial hospital to our emergency department suffering from an acute inferior ST-segment elevation myocardial infarction (STEMI). The patient entered the catheterization laboratory about 7½ hours after the onset of pain and 4 hours after failed fibrinolysis with reteplase.
Upon his initial presentation, the patient was in Killip class II, with basal pulmonary crackles and moderate distention of his jugular veins, respiratory rate of 20 breaths/min, heart rate of 95/ min, blood pressure 100/65 mmHg and 96% oxygen saturation on ambient air. Cardiac auscultation revealed an audible S3 sound and a moderate systolic murmur, indicative of mitral regurgitation.
His initial ECG, 3 hours after the onset of pain, revealed sinus rhythm, along with ST-segment elevation in the inferior leads (II, III, aVF) and reciprocal ST-segment depression in leads aVL, aVR, V1 and V2 (Figure 1), indicating an acute inferior myocardial infarction. The patient was subjected to thrombolysis with reteplase, right after the per OS administration of acetylsalicylic acid (325 mg), clopidogrel (300 mg), intravenous (iv) administration of 5.000 IU of heparin and 20 mg omeprazole. 90 minutes after the thrombolysis with reteplase, he reported a reduction in the intensity of his pain, but his ECG exhibited partial restoration (<50%) of the ST-segment elevation in the inferior wall leads, a sign of unsuccessful reperfusion (Figure 2). A decision was made to transport the patient immediately to our centre, in order to perform a rescue percutaneous coronary intervention (PCI). The patient developed several episodes of non-sustained monomorphic ventricular tachycardia (NSVT) and 3 episodes of sustained monomorphic ventricular tachycardia.
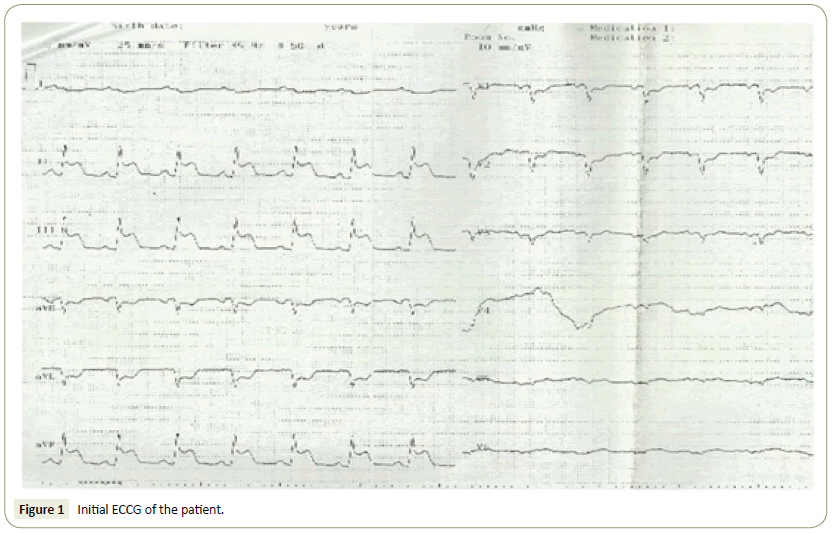
Figure 1: Initial ECCG of the patient.
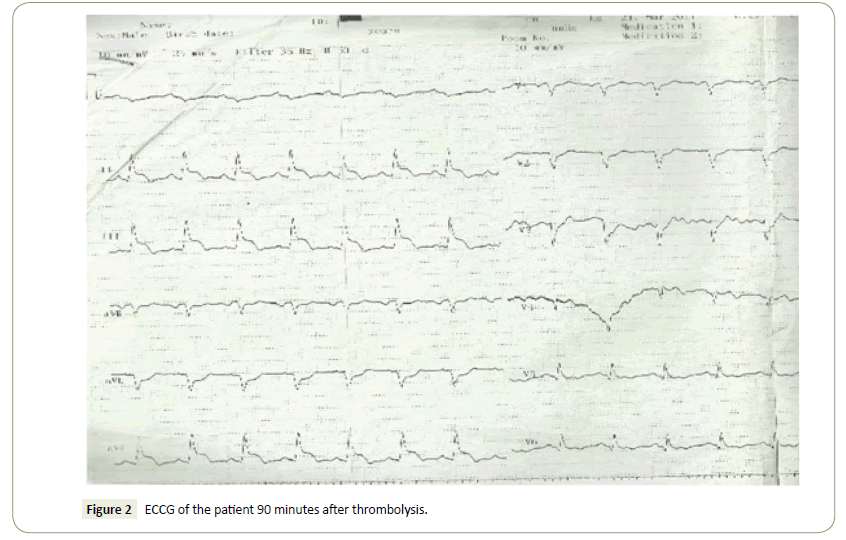
Figure 2: ECCG of the patient 90 minutes after thrombolysis.
Upon his arrival to our centre, 7½ hours after symptom onset, the patient was oriented and reported mild dyspnea. Coronary angiography through the radial artery revealed 90% in stentrestenosis in the proximal left anterior descending artery (LAD), moderate stenosis of 50-60% in the middle segment of the left circumflex (LCX) and total occlusion (100%) in the middle segment of the right coronary artery (RCA). After successful passage of the guidewire in the RCA, balloon dilatation was performed (Spinter© 2.0 × 10 mm) and a drug-eluting stent (DES) was placed (Promus Element Plus© 3.5 × 28 mm), with 0% remaining stenosis in the RCA (Figure 3). By the end of the procedure, the patient developed pulmonary edema and we were forced to terminate any other intervention. He was transported to the coronary care unit and treated with nasal oxygen, IV diuretics and IIb/IIIa antagonist (tirofiban) with complete restoration of his dyspnea. His heart failure treatment was re-initiated on the next day (Ramipril 5 mg 1 × 1, carvedilol 6.25 mg 1 × 2, eplerenone 50 mg 1 × 1). Figures 4 and 5 represent the patient’s ECGs on the day 1 and day 30 after PCI, respectively.
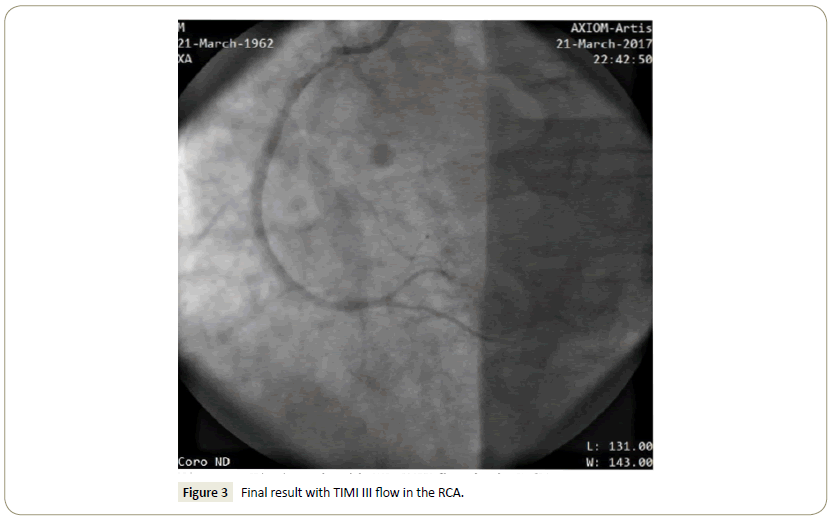
Figure 3: Final result with TIMI III flow in the RCA.
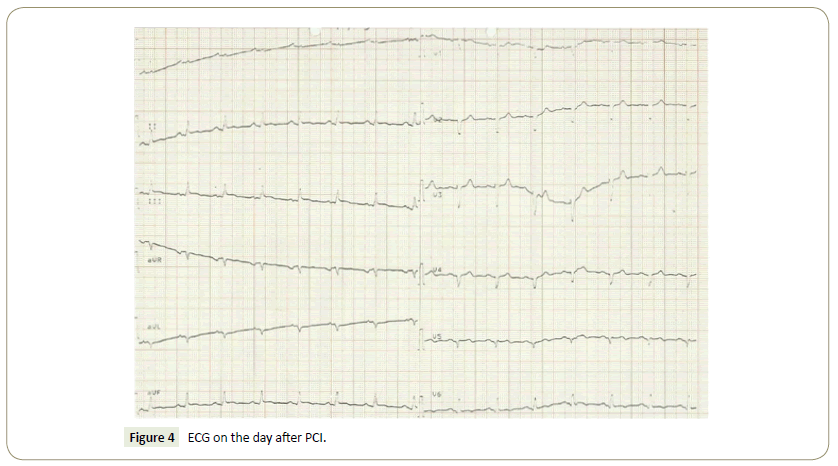
Figure 4: ECG on the day after PCI.
Figure 5: ECG on the day after PCI.
48 hours after his admission, our patient developed epigastric discomfort, nausea and elevated values of serum and urine amylase. A computed tomography of the abdomen and surgeons’ evaluation confirmed the diagnosis of ileus due to acute pancreatitis. A conservative approach was recommended and a Levin tube placed. The cardiac ultrasound revealed a left ventricular ejection fraction (LVEF) of 20%, with akinetic and thinned anterior wall, moderately to severely hypokinetic inferior wall, moderate functional mitral regurgitation, an E/A ratio of >>2 and E deceleration time <100 msec. His clinical course further deteriorated during the following days, with episodes of blood loss from the rectum, due to rectum fissures and subsequent fever development 1 week after the PCI with blood cultures positive for Staphylococcus haemolyticus. An IV antibiotic regimen was initiated, and the patient remained closely monitored in the coronary care unit.
The patient’s clinical stabilization was accomplished about 3 weeks after his hospital admission, with apyrexia and negative blood cultures, normalization of inflammation serum markers, gradual reduction in the IV doses of diuretics and inotropes, termination (days 20-22) of dopamine administration and one blood unit transfusion. It must be noted that his systolic blood pressure remained between 90-100 mmHg during the entire course of his hospitalization, with the patient clinically categorized as NYHA class IV and completely dependent on nasal oxygen up to that point. The BNP value was consistently >300-400 pgr/ml. After the patient was weaned off the inotropes, a decision was made to administer levosimendan on day 24 (both loading and 24-hour maintenance infusion of 0.1 μgr/Kgr/min), without any signs of clinical improvement in the following days.
Due to the patient’s continuous nasal oxygen dependence, his persisting NYHA class IV clinical condition even after the administration of levosimendan, along with the unsatisfying clinical response to the standard heart failure medication, we decided to suspend Ramipril administration on day 36. 36 hours later, on day 38, we initiated the low dose of the sacubitril/ valsartan combination (24/26 mg), 1 × 2 per day. On day 42, 4 days later, the patient was completely weaned from the nasal oxygen and clinically categorized as NYHA III. On day 44, a 2nd cardiac ultrasound was performed and revealed an EF 20%, E/A =2.4 and moderate mitral regurgitation (Figures 6 and 7) PISA with Effective regurgitant orifice area-EROA 18 mm2 and regurgitant volume of 20 ml). The patient was dismissed from the hospital two weeks later and underwent myocardial perfusion scintigraphy and a stress-echo, both of which demonstrated the complete absence of viable myocardium in the anterior wall (scar tissue) and no signs of reversible ischemia in the remaining walls of the left ventricle. Right heart catheterization was also performed (Figure 8) and the patient was then referred for further evaluation to a cardiac transplantation centre-heart failure clinic.
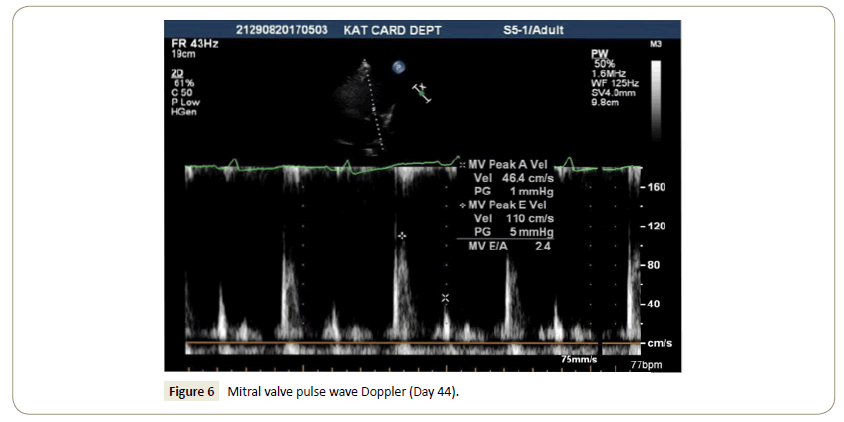
Figure 6: Mitral valve pulse wave Doppler (Day 44).
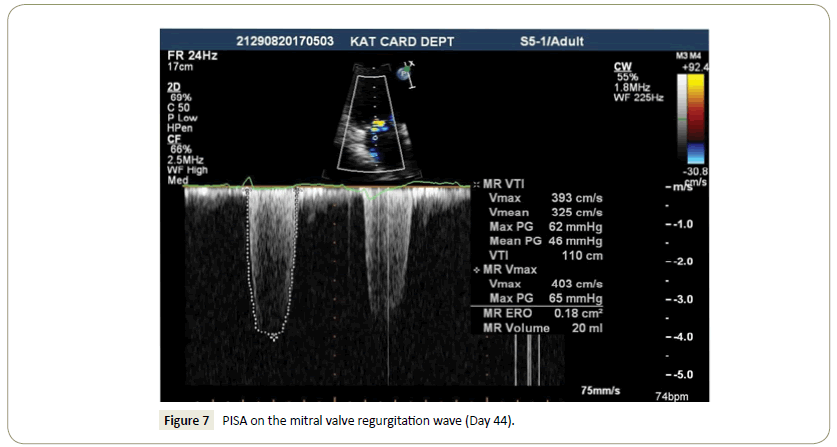
Figure 7: PISA on the mitral valve regurgitation wave (Day 44).
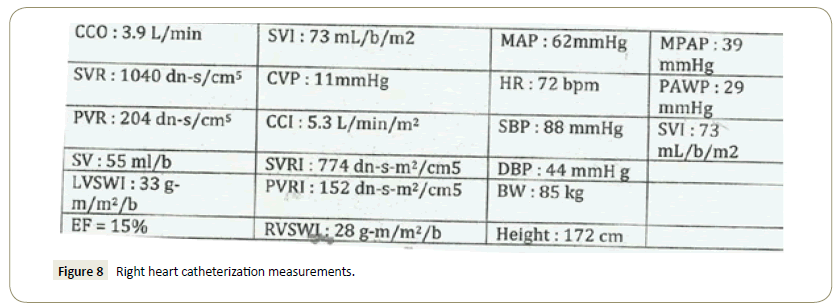
Figure 8: Right heart catheterization measurements.
Two months later, the patient underwent an implantable cardioverter-defibrillator (ICD) implantation, in accordance with ESC Guidelines on Acute and Chronic Heart Failure [2]. Today, approximately one year after his hospitalization, the patient is alive and well. His clinical condition has improved even further to NYHA class II, under the maximum dose of sacubitril valsartan (97/103 mg) 1 × 2 per OS/day.
Discussion
The presence of heart failure after an acute coronary syndrome has been identified as an independent factor of adverse prognosis, since the late 1960s [4]. Furthermore, data from the GRACE registry also confirm that patients suffering an acute coronary syndrome and present with Killip class II or III (the same class in which our patient was initially categorized), exhibit significantly higher mortality rates and reduced in-hospital and 6-month survival rates [5]. The in-hospital mortality rates in this particular registry ranged from 9.9% for patients presenting in Killip class II and 20.4% for patients presenting in Killip class III. Importantly, patients under 55 years old exhibited the highest relative increase in mortality rate related to heart failure, a finding which was consistent among all ACS patients [5]. Furthermore, ACS patients with an admission diagnosis of heart failure were more likely to be re- hospitalized than those with uncomplicated ACS, while post discharge mortality rates were similar between those who presented with heart failure and those who developed heart failure during the index hospitalization. The overall mortality rates remained lower for the heart failure patients who had undergone revascularization, when compared with those who did not [5].
Data from a more recent, single-center study which involved 1111 patients with STEMI, also suggest that the Killip classification in these patients is strongly associated with in-hospital prognosis [6]. According to these data, mortality increased with higher Killip class in patients with STEMI (1.5%, 3.7%, 16.7% and 36.7% in-hospital mortality for Killip classes I, II, III and IV, accordingly). Based on the aforementioned data, our patient was categorized in the group with the worst prognosis (55 years old, 16.7% to 20.4% in-hospital mortality), especially if he had not undergone a revascularization procedure (cumulative 6-month mortality of 23.7%).
Due to the fact that our patient exhibited an incredible recovery without any other alteration in his medical treatment, it is safe to assume that the most likely cause of his recovery was the ACEi replacement with sacubitril/valsartan. It must also be acknowledged that the administration of the sacubitril/valsartan combination to our patient remains an off-label use, since patients with SBP<100 mmHg were excluded from the PARADIGM-HF trial [1] and also NYHA IV patients were significantly underrepresented in the same trial (0.8% of the patient sample on sacubitril/valsartan, 0.6% on enalapril). As a result, there is no official indication to support the use of the sacubitril/valsartan combination in this patient category, mostly due to severe lack of evidence. However, there are some recent case reports on the ‘’off-label’’ use of sacubitril/valsartan for the successful weaning of inotropes in HIV cardiomyopathy and acute decompensated heart failure [7] and on the resolution of Cheyne-Stokes respiration in HF [8]. An animal model also suggested that the combination of sacubitril/valsartan in mice might be useful in improving the survival after acute myocardial infarction [9].
Conclusion
To our knowledge, this is the first case report on the successful, off-label use of the sacubitril/valsartan combination to a patient with acute heart failure after an acute coronary syndrome, during his initial hospitalization. In our opinion, the gradual increase of the dose to 97/103 mg 1 × 2 OS, during the next few months (Autumn) was decisive for the patient’s further clinical improvement to NYHA class II. More clinical trial data are urgently needed for this patient population, to obtain safer conclusions.
Acknowledgement
All the authors of this article have no conflicts of interest and did not receive any type of funding for this work.
References
- McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, et al. (2014) Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 371: 993-1004.
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, et al. (2016) 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 18: 891-975.
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, et al. (2017) ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines and the Heart Failure Society of America. Circulation 136: e137-161.
- Killip T, Kimball JT (1967) Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol 20: 457-464.
- Steg PG, Dabbous OH, Feldman LJ, Cohen-Solal A, Aumont MC, et al. (2004) Determinants and prognostic impact of heart failure complicating acute coronary syndromes: Observations from the Global Registry of Acute Coronary Events (GRACE). Circulation 109: 494-499.
- Vicent L, Velásquez-RodrÃÂÂÂguez J, Valero-Masa MJ, DÃÂÂÂez-Delhoyo F, González-SaldÃÂÂÂvar H, et al. (2017) Predictors of high Killip class after ST segment elevation myocardial infarction in the era of primary reperfusion. Int J Cardiol 248: 46-50.
- Bell TD, Mazer AJ, Miller PE, Strich JR, Sachdev V, et al. (2018) Use of sacubitril/valsartan in acute decompensated heart failure: a case report. ESC Heart Fail 5: 184-188.
- Fox H, Bitter T, Horstkotte D, Oldenburg O (2017) Resolution of Cheyne-stokes respiration after treatment of heart failure with Sacubitril/Valsartan: A first case report. Cardiology 137: 96-99.
- Ishii M, Kaikita K, Sato K, Sueta D, Fujisue K, et al. (2017) Cardioprotective effects of LCZ696 (Sacubitril/Valsartan) after experimental acute myocardial infarction. JACC Basic Transl Sci 2: 655-668.

