Paul Magill1, Paul French Ridgway1, Kevin Christopher Conlon2, Paul Neary1
1Department of General and Vascular Surgery; 2Professorial Surgery Unit, Department of Surgery, Trinity College Dublin. Adelaide Meath and National Childrens Hospital. Tallaght, Ireland
- *Corresponding Author:
- Paul Magill
54 Ashgrove road
Newry
Co. Down, BT34 1QN
Northern Ireland
Phone +353-87.779.1719
Fax +353-1.414.2212
E-mail paulmagill8@hotmail.com
Received: 18 February 2006 Accepted: 03 August 2006
Keywords
Hyperamylasemia /chemically induced; Ibuprofen; Pancreatitis, Acute Necrotizing
INTRODUCTION
Certain agents such as azathioprine and aminosalicylates have well documented associations with acute pancreatitis [1, 2]. It is imperative to identify specific drugs as possible causative aetiologies early in the clinical course in order to prevent any ongoing pancreatic injury. Non steroidal antiinflammatory drugs (NSAIDs) have rarely been identified as a definitive cause for acute pancreatitis. We present the most probable case to date of ibuprofen-induced pancreatitis.
CASE REPORT
An eighteen-year-old man with no previous medical or surgical history presented to our Emergency Department with a six-hour history of severe epigastric pain. He reported that five hours prior to the onset of symptoms, he had ingested seven tablets of ibuprofen 400 mg (equivalent to a 51.4 mg/kg bolus) in an attempt at deliberate self harm. He had been taking ibuprofen as prescribed for low back pain for one week prior to this event. He denied ingestion of other drugs or alcohol in the preceding days. This was confirmed by collateral history. The diagnosis of acute pancreatitis was made as per the UK Working Party on Acute Pancreatitis update criteria [3]. Serum amylase was 493 IU/L (reference range: 0-90 IU/L) and urinary amylase was 4,786 IU/L (reference range: 0-460 IU/L). His lactate dehydrogenase was 370 IU/L (reference range: 100-350 IU/L) and he had a leucocytosis of 11.6 x109/L (reference range: 4.0-11.0 x109/L). Liver function tests, calcium level and lipid profile were all normal. The Imrie (Glasgow) score predicted a mild course (score 0) of pancreatitis. The standard acute predicted mild pancreatitis treatment was commenced. Standard toxicology screen at twenty-four hours was negative for alcohol, salicylates and paracetamol. The screening imaging demonstrated no sonographic evidence of cholelithiasis. Although not standard practice, given the unusual clinical presentation we performed computerized tomography at 48 hours which was graded as Balthazar A, consistent with mild pancreatitis [4] with otherwise normal anatomy and notably no double duct sign [5]. We did not feel that any further invasive investigation regarding pancreas ductal anatomy was warranted. Given the large dose NSAID ingestion, to rule out a gastric cause of epigastric pain a gastroscopy was performed, which was normal. The patient made an uneventful recovery. The serum amylase normalised by day three using conservative management, without a need for antibiotics. He commenced oral diet on day three and on day five he was discharged home. He was seen for out-patient follow-up at the 6-week point with no subsequent adverse consequences. We advised our patient to avoid using ibuprofen and hence there has been no re-exposure to date.
DISCUSSION
This case characterises an association between acute pancreatitis and ibuprofen ingestion. This relationship has only been suggested in two previous publications. The first report [6] was in a patient with systemic lupus erythematosus who displayed a hyperamylasaemia along with parotiditis in what was termed a general hypersensitivity reaction to ibuprofen. There was no definite diagnosis here and lupus itself is considered a risk factor for the development of acute pancreatitis. The second was by Eland et al. [7]. This was a review of adverse drug reaction reports in the Netherlands over a twenty-one year period. The study investigated links between acute pancreatitis and a number of agents. They were able to clarify a definite diagnosis of acute pancreatitis in 34 out of 55 reported cases and they then labelled the association as definite if there was a positive re-challenge. In one case a 25-year-old female had an antecedent history of protracted use of ibuprofen. The diagnosis however was not clearly established and there was no positive re-challenge and so the case was defined as a probable association only.
The UK guidelines for diagnosis of acute pancreatitis [3] include a rise of amylase (or lipase where available) within 48 hours of characteristic abdominal pain. A greater than four-fold rise, as seen in our case, is desirable but not always required. We eliminated the most common aetiological factors in developing pancreatitis and are therefore left with either idiopathic or ibuprofen-induced pancreatitis. Given the temporal relationship between ingestion and onset and the general rarity of acute idiopathic pancreatitis in an 18- year-old, we believe it is reasonable to suggest a probable cause and effect relationship.
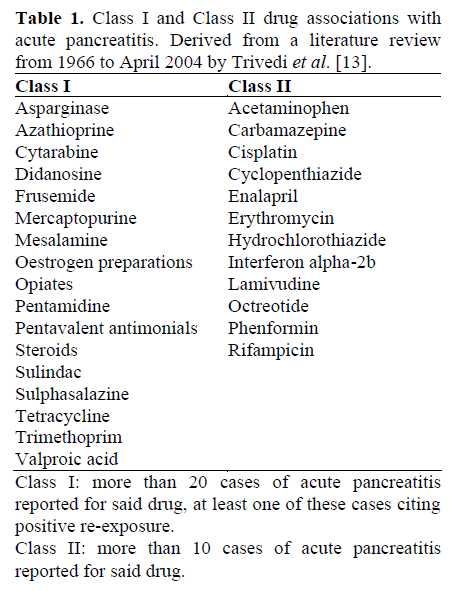
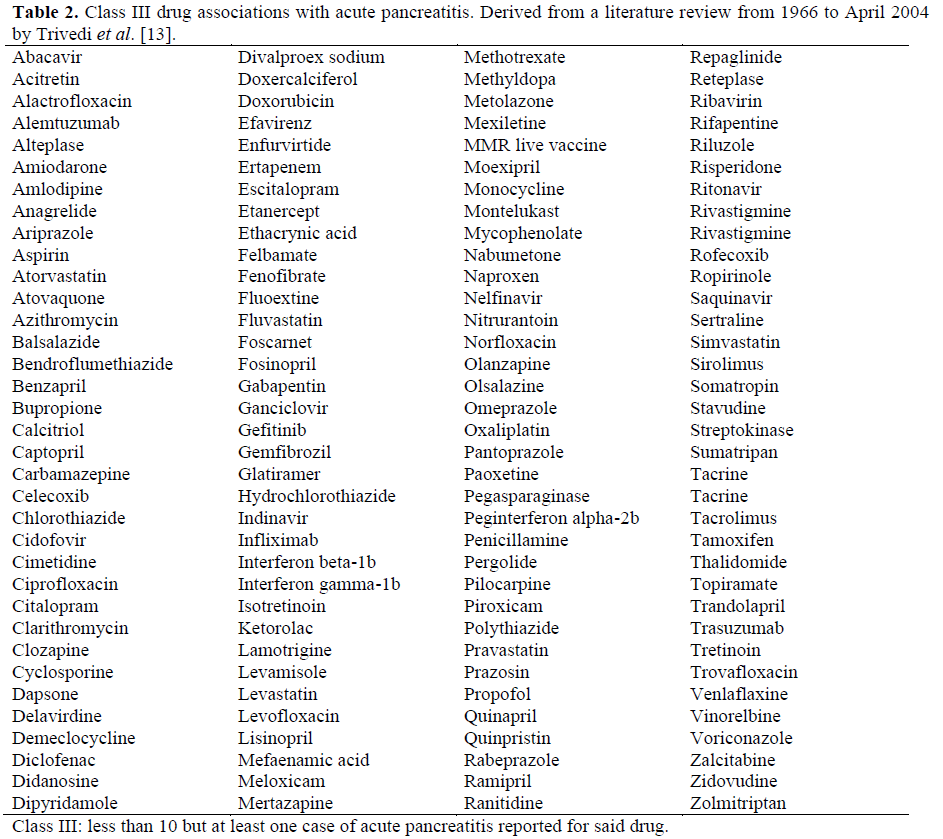
Eland et al. proposed the ibuprofen effect at a dose of 3,600 mg over a 10 day period (dose/kg unknown). Our patient ingested a bolus of 2,800 mg which correlates to 51.4 mg/kg. The use of activated charcoal is recommended if ingestion of more than 400 mg/kg in the preceding hour has occurred [8]. Our patient had been taking 1,600 mg daily for one week prior to this event. It is not clear whether the cumulative effect is important but with a plasma half-life of 1.9 to 2.2 hours [9], it would seem improbable unless a steady state had been maintained up to the overdose. There are a multitude of drugs which are also possible causes of acute pancreatitis (Tables 1 and 2) [1, 2, 7, 10, 11, 12, 13, 14, 15]. Other reports of NSAID-induced pancreatitis are few. Sulindac seems to be the most reported [14, 15] and the mechanism by which this occurs is unknown. One hypothesis however links the possibility of NSAIDS reducing the amount of systemic glutathione and hence inducing an oxidative stress reaction [16]. Indeed there is no data to predict the clinical course in these cases. Clinical scoring systems have not been validated in this population (owing to rarity) nor has it been determined whether they are likely to follow a more severe course. In our case we adopted standard pancreatitis protocols as per consensus guidelines [3]. We do not have data to recommend whether this index case should avoid therapeutic dose of NSAIDS in the future. However, it would seem appropriate to follow up the case at regular intervals for some time.
In summary, we document a clinical case of acute mild pancreatitis. The patient had no previous medical history and no risk factors for the development of acute pancreatitis. Immediately preceding the onset of the attack he took a 51 mg/kg dose of ibuprofen. He had other causes of acute pancreatitis excluded by clinical history, serum toxicology and abdominal imaging. In the absence of re- challenge we believe it is probable that ibuprofen has a causative link with acute pancreatitis.
References
- Banerjee AK, Patel KJ, Grainger SL. Druginduced acute pancreatitis. A critical review. Med Toxicol Adverse Drug Exp 1989; 4:186-98. [PMID 2664430]
- Wilmink T, Frick TW. Drug-induced pancreatitis. Drug Saf 1996; 14:406-23. [PMID 8828018]
- UK Working Party on Acute Pancreatitis. UK guidelines for the management of acute pancreatitis. Gut 2005; 54:iii1-9.
- Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH. Acute pancreatitis: value of CT in establishing prognosis. Radiology 1990; 174:331-6. [PMID 2296641]
- Delhay M, Matos C, Deviere J. Acute relapsing pancreatitis. Congenital variants: diagnosis, treatment, outcome. JOP. J Pancreas (Online) 2001; 2:373-81. [PMID 11880697]
- Ruppert GB, Barth WF. Ibuprofen hypersensitivity in systemic lupus erythematosus. South Med J 1981; 74:241-3. [PMID 7466447]
- Eland IA, van Puijenbroek EP, Sturkenboom MJ, Wilson JH, Stricker BH. Drug-associated acute pancreatitis: twenty-one years of spontaneous reporting in the Netherlands. Am J Gastroenterol 1999; 94:2417- 22. [PMID 10484002]
- Volans G, Monaghan J, Colbridge M. Ibuprofen overdose. Int J ClinPractSuppl 2003; 135:54-60. [PMID 12723749]
- Ibuprofen data sheets. November 2004. Available at https://www.medsafe.govt.nz/DatasheetPage.htm (search for ibuprofen). Accessed, 17th October 2005.
- Singh S, Nautiyal A, Dolan JG. Recurrent acute pancreatitis possibly induced by atorvastatin and rosuvastatin. Is statin induced pancreatitis a class effect? JOP. J Pancreas (Online) 2004; 5:502-4. [PMID 15536291]
- Antonopoulos S, Mikros S, Kokkoris S, Protopsaltis J, Filioti K, Karamanolis D, Giannoulis G. A case of acute pancreatitis possibly associated with combined salicylate and simvastatin treatment. JOP. J Pancreas (Online) 2005; 6:264-8. [PMID 15883478]
- Nigwekar SU, Casey KJ. Metronidazole-induced pancreatitis. A case report and review of literature. JOP. J Pancreas (Online) 2004; 5:516-9. [PMID 15536294]
- Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis: an update. J Clin Gastroenterol 2005; 39:709-16. [PMID 16082282]
- Goldstein J, Laskin DA, Ginsberg GH. Sulindac associated with pancreatitis. Ann Intern Med 1980; 93:151. [PMID 7396304]
- Lilly EL. Pancreatitis after administration of sulindac. JAMA 1981; 246:2680. [PMID 7310962]
- Memis D, Akalin E, Yucel T. Indomethacininduced pancreatitis: A case report. JOP. J Pancreas (Online) 2005; 6:344-7. [PMID 16006685]

