Keywords
Carcinoma; KRAS protein, human; Pancreas; SMARCB1 protein, human
INTRODUCTION
Undifferentiated/anaplastic carcinoma (UAC) of the pancreas is a rare neoplasm that accounts for 2-7% of pancreatic neoplasms [1]. The tumor histologically shows round giant cells, pleomorphic cells, spindle cells, or even rhabdoid cells [2] and commonly contains small foci of atypical glandular elements; this glandular component is identical to that of ductal adenocarcinoma (DAC), thus indicating pancreatic UAC to be a subtype of ordinary DAC of the pancreas. If pancreatic UAC lacks the associated DAC component, it may be indistinguishable from a sarcoma.
Sarcomas of the pancreas are extremely rare, accounting for less than 0.1% of all pancreatic malignancies [3]. The literature reveals occasional examples such as leiomyosarcoma, liposarcoma, primitive neuroectodermal tumor, desmoplastic small round cell tumor, sclerosing epithelioid fibrosarcoma, malignant fibrous histiocytoma/ undifferentiated pleomorphic sarcoma, fibrosarcoma, follicular dendritic cell sarcoma, and malignant peripheral nerve sheath tumor [4, 5]. In addition, some of these tumors may actually arise from adjacent tissues such as the retroperitoneum or the duodenal wall and secondarily involve the pancreas.
Classical epithelioid sarcoma (ES), first described by Franz Enzinger in 1970 [6], is an uncommon malignant neoplasm of soft tissue with an unknown lineage and typically presents as a subcutaneous or deep dermal mass in “distal” portions of the extremities of adolescents or young adults. The histological findings are characterized by nodules of spindle and epithelioid tumor cells circumscribing hyalinization or necrosis (granuloma-like pattern). Patients often develop multiple local recurrences, with subsequent metastases in approximately 30 to 50% of cases over a long duration of time (5 to 10 years) [7].
The “proximal-type” ES (PES) was first reported in 1997 by Guillou et al. [8] as a subtype of ES occurring as a deep-seated soft tissue mass at proximal body sites. The proximal extremities, limb girdles, chest wall, trunk, back, pelvis, genital tract, vulva and perineum have been reported as distinct locations for PES. PES is histologically characterized by a solid growth pattern of larger cells with prominent nucleoli or pleomorphic rhabdoid cells, in addition to the conventional histological appearance of classical “distal-type” ES (DES) described above. PES is more aggressive than DES, and approximately 65% of all cases develop local recurrence and 75% have metastases within a short duration of time (several months to years) [9].
Despite the differences in the clinical presentation and histological features, DES and PES share a similar immunophenotypic profile: a co-expression of epithelial markers, cytokeratin and epithelial membrane antigen (EMA), and a mesenchymal marker, vimentin, and a frequent expression of CD34, which provide a strong contribution for the diagnosis of DES or PES [10], accompanying the lack of significant expression of specific differentiation markers such as myogenic, angiogenic, or neurogenic markers(e.g., desmin, S100 protein). The loss of SMARCB1/INI1 protein expression, which is frequently and specifically associated with PES or DES as well as malignant rhabdoid tumors [11-13], may strongly assist the diagnosis.
The pancreas is an unusual site for PES. When encountered a tumor similar to PES it may be diagnosed as pancreatic UAC or pancreatic undifferentiated rhabdoid carcinoma [2, 14]. Therefore there have thus far been no reports of PES arising in or involving the pancreas. We here discussed the differential diagnosis of pancreatic UAC vs. PES through the present case showing specific histological and immunohistochemical characteristics of PES.
CASE REPORT
The patient was a 35-year-old female who complained of epigastralgia and back pain and presented with tarry stools and a weight loss of 4 kg per month. No jaundice was observed. A growing tumor measuring more than 6 cm in diameter was detected in the pancreatic head on several abdominal images, with invasion into the surrounding large blood vessels and metastases to the surrounding lymph nodes and the liver. Computed tomography showed that the tumor contained a massive hemorrhage, corresponding to a heterogeneous signal area by magnetic resonance imaging (Figure 1). On upper endoscopy, bleeding from the duodenal papilla of Vater was noticed. The main pancreatic duct (MPD) and the common bile duct (CBD) were pressed by the large tumor, however, the upstream dilatation was not prominent. Positron emission tomography showed significant tumorous signals only in the pancreas and the liver, not in other sites including the extremities. The serum neuron-specific enolase (NSE) level was mildly elevated (15.3 ng/ml), however, carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9) were within the normal limits. An exploratory laparotomy liver biopsy revealed malignant cells. Chemotherapy using TS-1 (80 mg per day by internal use) was performed, however, it was unsuccessful. A large amount of ascites merged by diffuse peritoneal dissemination and the patient died within seven monthsafter the onset of symptoms. An autopsy was subsequently performed.
Figure 1a, b. A computed tomography (CT) scan and magnetic
resonance imaging (MRI) of the abdomen. CT (a. plain; b. contrast)
shows hemorrhagic masses in the pancreas head and in the liver, (c.). corresponding to heterogeneous signal areas by MRI.
Pathological Findings
Microscopic Findings of the Liver Biopsy: A diffuse infiltration of epithelioid and spindle-shaped cells with abundant eosinophilic cytoplasm was seen in the liver biopsy (Figure 2). The nuclei were round to spindleshaped and showed moderate pleomorphism, and some of them were grooved. Mitotic figures were scattered at 5 per 10 high-power fields. Lymphocytic inflammatory cells infiltrated between the tumor cells. Ultrastructurally, the tumor cells exhibited aggregates of intermediate filaments, desmosome-like cell junctions, and small intercellular spaces surrounded by filopodia (Figure 3). No definite findings suggestive of specific differentiation were observed.
Figure 2. Histological findings of the liver biopsy.
Diffuse infiltration of spindle to epithelioid atypical cells is seen with
lymphocytic cells. They have abundant eosinophilic cytoplasm.
Figure 3. Electron microscopic findings of tumor cells from the liver
biopsy. Tumor cells exhibit aggregates of intermediate filaments (a, b), (a.). desmosome-like cell junctions, and (b.). small intercellular spaces
surrounded by filopodia.
Autopsy Findings
A large, whitish mass with severe hemorrhage and necrosis, mainly located in the head portion of the pancreas, involved the whole pancreas. The mass measured 18x13 cm in size. Microscopically, the tumor showed medullary growth with hemorrhage and edema and consisted of pleomorphic spindle to epithelioid cells, which were loosely cohesive and included rhabdoid morphology (Figures 4, 5), appearing to be more pleomorphic than those observed in the liver biopsy. They infiltrated diffusely or in lobules separated by fibrous septa. Approximately half of the cells were spindle while the other half was epithelioid cells and they merged imperceptibly. Mitotic figures were scattered at 5 per 10 high-power fields. The glandular component, suggestive of ductal adenocarcinoma, could not be detected by total sampling. The tumor cells invaded the second portion of the duodenum and the portal vein, metastasized to the peripancreatic and mesenteric lymph nodes, the liver, and the lumbar vertebrae, and disseminated widely to the peritoneum. In bone metastases, spindle-shaped cells arranged in a storiform or fascicular growth pattern were predominantly observed.
Figure 4. Histological findings of the pancreatic tumor (low power view). The
tumor shows medullary growth of pleomorphic spindle to epithelioid cells.
Figure 5. Histological findings of the pancreatic tumor (high power view).
Tumor cells consist of poorly cohesive, spindle (a.). and epithelioid or
rhabdoid, (b.). cells.
Immunohistochemical and Molecular Analyses
Immunohistochemical staining was performed using the antibodies listed in Table 1 and each antigen localization was detected using peroxidase labeled amino acid-polymer (Histofine Simple Stain MAX-PO (M), Nichirei, Tokyo, Japan). The tumor cells were diffusely positive for cytokeratin (AE1/AE3), cytokeratin 19, EMA, vimentin, CD34 (Figure 6), NSE, and β-catenin, and were negative for cytokeratin 7, cytokeratin 20, S100 protein, CD99 (MIC2), c-kit, desmin, α-smooth muscle actin (αSMA), myoglobin, CD31, factor-VIII, calretinin, mesothelial cell (HBME-1), chromogranin A, synaptophysin, CD56, CA125, leukocyte common antigen (LCA) and trypsin (Table 1). In addition, a loss of SMARCB1/INI1 protein expression (using BAF47, an antibody to the SMARCB1/INI-1 gene product (clone 25; BD Transduction Laboratories, San Diego, CA)) was found (Figure 7). On the other hand, no alterations (homozygous deletion and mutation) at the DNA level sufficient to suppress the expression of SMARCB1/INI1 gene products were recognized by real-time polymerase chain reaction and direct sequencing. The detailed methods of SMARCB1/INI1 detection are described elsewhere [12]. In addition, mutations in codons 12 and 13 of the KRAS gene were not seen by direct sequencingperformed by a clinical testing company (SRL, Tokyo, Japan). As for these immunohistochemical and molecular results, there were no differences between the liver biopsy specimen and autopsy specimen of the primary pancreatic mass.
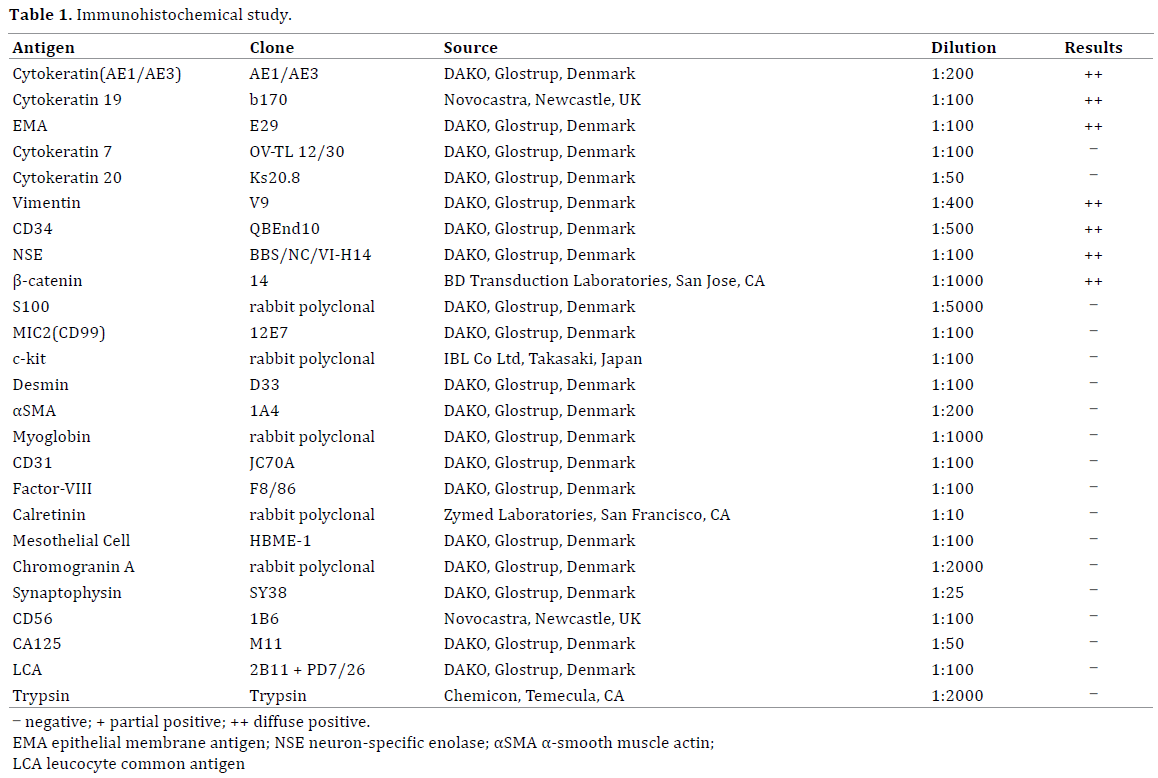
Figure 6. CD34 immunohistochemical staining of the pancreatic tumor.
Rhabdoid tumor cells show diffuse CD34 expression.
Figure 7. SMARCB1/INI1 immunohistochemical staining of the
pancreatic tumor. Expression of SMARCB1/INI1 protein is not seen in the
nuclei of rhabdoid tumor cells, while its expression is seen in the nuclei of
endothelial cells and lymphocytes (inner control).
DISCUSSION
Regarding the histologic type of the present tumor, PES was considered primarily from the sarcomatoid solid growth histology which consisted of epithelioid, spindle or rhabdoid cells and immunohistochemical positivity for cytokeratin, EMA, vimentin, and CD34, although its occurrence in the pancreas is exceedingly unusual. The immunoreactivity for NSE and β-catenin found in this tumor has been previously described in PES [9, 15]. The ultrastructural findings were also consistent with those of PES in previous reports [16]. In addition, immunohistochemical negativity of various specific differentiation markers including myogenic, angiogenic, neurogenic/neuroendocrine and mesothelial markers (e.g., desmin, s100 protein, CD31, calretinin), LCA, and CD99 (MIC2) excluded other epithelioid or rhabdoid neoplasms often confused with PES, such as synovial sarcoma, malignant mesothelioma, malignant melanoma, epithelioid angiosarcoma, epithelioid hemangioendothelioma, epithelioid malignant peripheral nerve sheath tumor, and extrarenal malignant rhabdoid tumor.
Indeed pancreatic UAC also commonly demonstrates co-expression of cytokeratin/EMA and vimentin and occasionally exhibits rhabdoid features, but there were several reasons suggestive of PES rather thanUAC as follows: i. the patient was young in her 30s. The mean age at diagnosis is 40 years for PES [8] vs. 63 years for UAC [17]; ii. the ductal adenocarcinoma (DAC) component, which is typically observed in pancreatic UAC, could not be detected in the pancreatic tumor even with extensive sampling, although the pre-existing DAC component may have been eradicated by the massive invasion of sarcomatoid cells transformed from DAC cells in the early stage or this tumor may have originated from epithelial precursors but occurred as a sarcomatoid tumor without an apparent DAC component from the beginning; iii. theimmunohistochemical expression of cytokeratin 7, a pancreatobiliary duct marker which is in patches but strongly immunostained in UAC, was not seen in the present tumor; iv. aKRAS mutation was not detected in this tumor, while most UACs harbor KRAS mutations, supporting the hypothesis that UACs arise from ductal adenocarcinoma [17]; v. the immunohistochemical expression of CD34 as well as the co-expression of cytokeratin/EMA and vimentin, which contributes strongly to the diagnosis of PES, was readily demonstrated. No reports have focused on the CD34 expression in pancreatic UACs. Moreover, none of 10 pancreatic UACs in our institutes showed CD34 expression (data not shown), however, further studies are needed to address the expression of this marker, because several reports of sarcomatoid carcinomas have demonstrated CD34 expression in other organs [18]; and vi. the loss of SMARCB1/INI1 protein expression, which has been reported to be a frequent, specific event in PES [11-13], was demonstrated in the present tumor, while none of the 5 pancreatic UACs in our institutes showed the loss of SMARCB1/INI1 protein expression (data not shown). Our molecular study showed no alterations (homozygous deletion and mutation) at the DNA level, however, this is not surprising because previous studies with SMARCB1/ INI1 negative tumors by immunohistochemistry showed that the percentage of cases with homozygous SMARCB1/ INI1 deletions ranged from 5–71% [12, 13, 19]. The evaluation of the SMARCB1/INI1 status using another method (e.g., Sanger sequencing of the coding region and multiplex ligation-dependent probe amplification, a rapid and sensitive method for detecting intragenic deletions and duplications) may solve the conflicting results [20].
Nevertheless, there are several reportssuggesting a difficulty in distinguishing PES from UAC, even if the loss of this protein or its gene alteration is confirmed. Cheng et al. showed the loss of SMARCB1/INI1 expression in renal medullary carcinoma with rhabdoid features [21]. Donner et al. reported the loss of SMARCB1/INI1 expression and its gene alteration in uterine carcinosarcomas with rhabdoid components (composite rhabdoid tumors) [22]. Moreover, Cho et al. reported a SMARCB1/INI1 missense mutation in mucinous carcinoma of the pancreas accompanying poorly differentiated carcinoma with rhabdoid features [23]. Thus, pancreatic UACs with rhabdoid features may also have abnormalities of SMARCB1/INI1, and this may indicate that the present tumor is a special type of UAC.
Recently Agaimy A et al. studied 14 cases of pancreatic undifferentiatd carcinomas with prominent rhabdoid cells and coexpression of cytokeratin and vimentin and proposed two subtypes characterized by KRAS alterations and SMARCB1/INI1 expression status: pleomorphic giant cell subtype with KRAS alterations and intact SMARCB1/ INI1 expression and monomorphic anaplastic subtypewith abscence of KRAS alterations and loss of SMARCB1/INI1 expression [2, 14]. Although their monomorphic anaplastic subtype as well as pleomorphic giant cell subtype did not express CD34, the present case appears to correspond to the monomorphic anaplastic subtype.
Nonetheless, its histological, immunohistological and molecular characters were completely identical to those of PES, thus the clinical treatment and care for PES as a sarcoma may be recommended rather than those for UAC as a subtype of ductal adenocarcnoma. Further accumulation of similar cases of pancreatic tumor will lead to the adequate diagnosis and may clarify the distinctions between a rhabdoid variant of pancreatic UAC and true pancreatic PES.
In conclusion, we herein described an autopsy case of a fatal metastasizing pancreatic sarcomatoid tumor, closely mimicking PES, characterized by epithelioid and rhabdoid histology, co-expression of cytokeratin/EMA and vimentin, CD34 positivity, no DAC component, CK7 negativity, lack of a KRAS mutation and the loss of SMARCB1/INI1 protein expression. The tumor may be classified as pancreatic UAC, but distinctive treatment strategies will be required.
Conflict of Interests
All the authors have no conflicts of interest or financial ties to disclose.
References
- Fukushima N, Hruban RH, Kato Y, Klimstra DS, Kloppel G, Shimizu M, et al. Ductal adenocarcinoma variants and mixed neoplasms of the pancreas. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, eds. World Health Organization Classification of Tumours of the Digestive System. Lyon: International Agency for Research on Cancer (IARC) Press 2010; 292-5.
- Agaimy A, Haller F, Frohnauer J, Schaefer IM, Ströbel P, Hartmann A, et al. Pancreatic undifferentiated rhabdoid carcinoma: KRAS alterations and SMARCB1 expression status define two subtypes.Mod Pathol 2015; 28:248-60. [PMID: 25103069]
- Baylor SM, Berg JW. Cross classification and survival characteristics of 5000 cases of cancer of the pancreas. J SurgOncol 1973; 5: 335–58. [PMID: 4355621]
- Hruban RH, Pitman MB, Klimstra DS. Nonepithelial and miscellaneous neoplasms. In: Hruban RH, Pitman MB, Klimstra DS. eds. AFIP Atlas of Tumor Pathology Fourth Series Fascicle 6: Tumors of the Pancreas. Washington, DC: American Registry of Pathology, 2007, 305-24.
- Lack EE. Primary tumors and tumefactive lesions along with tumors secondarily involving the pancreas. In: Lack EE, eds. Pathology of the Pancreas, Gallbladder, Extrahepatic Biliary Tract, and Ampullary Region. New York: Oxford University Press, 2003; 374-91.
- Enzinger FM. Epitheliod sarcoma: a sarcoma simulating a granuloma or carcinoma. Cancer.1970; 26:1029-41. [PMID: 5476785]
- Chase DR, Enzinger FM. Epithelioid sarcoma. Diagnosis, prognostic indicators, and treatment.Am J Surg Pathol 1985; 9: 241-63. [PMID: 4014539]
- Guillou L, Wadden C, Coindre JM, Krausz T, Fletcher CD. "Proximal-type" epithelioid sarcoma, a distinctive aggressive neoplasm showing rhabdoid features. Clinicopathologic, immunohistochemical, and ultrastructural study of a series.Am J Surg Pathol 1997; 21: 130-46. [PMID: 9042279]
- Hasegawa T, Matsuno Y, Shimoda T, Umeda T, Yokoyama R, Hirohashi S. Proximal-type epithelioid sarcoma: a clinicopathologic study of 20 cases. Mod Pathol 2001; 14: 655-63. [PMID: 11454997]
- Guillou L, Kaneko Y. Epithelioid sarcoma. In: Christopher DM, Fletcher K, Krishnan Unni, Fredrik Mertens, eds. World Health Organization Classification of Tumours; Pathology and Genetics, Tumours of Soft Tissue and Bone. Lyon: International Agency for Research on Cancer (IARC) Press, 2002; 205-7.
- Hornick JL, Dal Cin P, Fletcher CD. Loss of INI1 expression is characteristic of both conventional and proximal-type epithelioid sarcoma. Am J SurgPathol2009; 33: 542-50. [PMID: 19033866]
- Kohashi K, Izumi T, Oda Y, Yamamoto H, Tamiya S, Taguchi T, et al. Infrequent SMARCB1/INI1 gene alteration in epithelioid sarcoma: a useful tool in distinguishing epithelioid sarcoma from malignant rhabdoid tumor. Hum Pathol 2009; 40: 349-55. [PMID: 18973917]
- Modena P, Lualdi E, Facchinetti F, Galli L, Teixeira MR, Pilotti S, et al. SMARCB1/INI1 tumor suppressor gene is frequently inactivated in epithelioid sarcomas. Cancer Res 2005; 65: 4012-9. [PMID: 15899790]
- Agaimy A. The expanding family of SMARCB1(INI1)-deficient neoplasia: implications of phenotypic, biological, and molecular heterogeneity.Adv Anat Pathol 2014;21:394-410. [PMID: 25299309]
- Saito T, Oda Y, Itakura E, Shiratsuchi H, Kinoshita Y, Oshiro Y, et al. Expression of intercellular adhesion molecules in epithelioid sarcoma and malignant rhabdoid tumor. Pathol Int 2001; 51: 532-42. [PMID: 11472566]
- Weiss SW, Goldblum JR. Epithelioid sarcoma. In Enzinger and Weiss’s Soft Tissu Tumors. 5th ed. Mosby-Elsevier; Philadelphia, 2008, 1191-203.
- Hruban RH, Pitman MB, Klimstra DS. Adenocarcinoma variants. In: Hruban RH, Pitman MB, Klimstra DS. eds. AFIP Atlas of Tumor Pathology Fourth Series Fascicle 6: Tumors of the Pancreas. Washington, DC: American Registry of Pathology, 2007, 165-90.
- Costa MJ, Guinee D Jr. CD34 immunohistochemistry in female genital tract carcinosarcoma (malignant mixed müllerian tumors) supports a dominant role of the carcinomatous component. Appl Immunohistochem Mol Morphol 2000; 8: 293-9. [PMID: 11127921]
- Gasparini P, Facchinetti F, Boeri M, Lorenzetto E, Livio A, Gronchi A, et al. Prognostic determinants in epithelioid sarcoma. Eur J Cancer 2011; 47: 287–95. [PMID: 20932739]
- Sullivan LM, Folpe AL, Pawel BR, Judkins AR, Biegel JA. Epithelioid sarcoma is associated with a high percentage of SMARCB1 deletions. Mod Pathol. 2013; 26: 385–92. [PMID: 23060122]
- Cheng JX, Tretiakova M, Gong C, Mandal S, Krausz T, Taxy JB. Renal medullary carcinoma: rhabdoid features and the absence of INI1 expression as markers of aggressive behavior. Mod Pathol 2008; 21: 647-52. [PMID: 18327209]
- Donner LR, Wainwright LM, Zhang F, Biegel JA. Mutation of the INI1 gene in composite rhabdoid tumor of the endometrium.Hum Pathol 2007; 38: 935-9. [PMID: 17376508]
- Cho YM, Choi J, Lee OJ, Lee HI, Han DJ, Ro JY.SMARCB1/INI1 missense mutation in mucinous carcinoma with rhabdoid features. Pathol Int 2006; 56: 702-6. [PMID: 17040295]








