Keywords
Virtual clinical education; Virtual reality; E-simulation; Web-based Simulation; Virtual clinical simulation
Introduction
Clinical experience is the very foundation of health care practice disciplines. This includes nursing, especially. Many factors have caused nursing academics to search for alternative pedagogies to supplement the traditional live or hands-on clinical practice experience. There are several reasons for these efforts. These include the shortage of nursing faculty, competitive clinical sites, high student-to-nurse faculty ratio, patient safety concerns of faculty, and student apprehension [1,2].
As of result of such barriers, the pedagogies of standardized patients and clinical simulation scenarios have evolved as valuable tools. They prove valuable for their ability to enhance both theoretical and clinical nursing education. Nevertheless, both teaching strategies have proven to be resource intensive in the use of nursing staff, manikins, and other tools to increase the fidelity of such teaching scenarios. In today’s evolving and the highly technical world, distance education has proven effective and has been accepted as an educational method. Despite distance education being highly acceptable in the nursing academic community, distance education is limited in its presentation in didactic content and lacks the capability to provide skills-based clinical education. Virtual clinical simulation is described as “a recreation of realistic environments in a context where learners view authentically repeated clinical settings in 3D (such as a ward environment) via the internet” [3]. However, the concept of virtual clinical education has yet to be explored in depth despite its increasing use. This article will attempt to describe this up and coming phenomenon of interest.
Meleis [4] explains the importance of concept exploration. It is a strategy used to develop a concept that has become newly identified and before it becomes an accepted constituent of the nursing lexicon. Interestingly, “a concept may have been accepted in the daily experience of nurses [as have virtual clinical education], yet because it is embedded in the nursing experiences, its existence and properties are normalized, thereby limiting the concept’s growth and meanings”. The purpose of this discussion is to prevent the dwarfing of the concept and meaning of virtual clinical education.
Method
The purpose of this essay is to explore the term ‘Virtual Clinical Simulation’ (VCS) which is also referred to as ‘e-simulation’ and ‘virtual clinical education’. VCS an emerging technology that has been utilized to broaden teaching strategies being used in health science and nursing instruction.
This phenomenon will be analyzed utilizing the Wilsonian method of concept analysis. According to Wilson [5] concept analysis has 11 imperative steps. The first two steps include identifying and isolating questions of the concept. Thirdly, exemplars are identified and described to “reflect the different critical and essential characteristics of the concept” [4] by the identification of contrary cases that exclude the essential characteristic of the concept. The fifth step involves identification, description, and use of related cases in which the concept may be similar in one way or as the concept occurs in similar texts. Next, borderline cases are to be included which have some aspects of the concept but in which abstruseness exists about whether the case belongs to the concepts or not or that are difficult to classify because they help further develop the concept. From here invented cases are developed and presented. Finally, the identification of social concepts should then occur, followed by sentiments and underlying anxiety related to or generated by the concept [4].
Identification and isolation of questions of VCS’s
Wilson [5] described the first step of concept analysis to include the identification and isolation of questions of the concept. Three separate categories of questions are to be included. The first group should be questions related to facts or that are answered by the current knowledge of the concept. The second group of questions should relate to values of the concept, referring to the moral principles of the concept-perhaps explaining when the phenomenon ‘should’ and ‘should not’ be used. The third group of questions are to include inquiries about meanings which do not explain facts or values. These questions’ focus is asked in terms of concepts.
In utilizing the Wilsonian method of concept analysis, the following questions are posed
Facts: What is a virtual clinical simulation within the discipline of nursing mean? What are the key features of a virtual clinical simulation? What events triggered the creation of virtual clinical simulations? What happened before the invention of virtual clinical simulation to inspire its creation? What has occurred as a result of virtual clinical simulations?
Values: What is the value of virtual clinical simulations to the profession of nursing education? When do such professionals consider such a method of simulation ‘should’ be used or ‘should not’ be used? Are there certain circumstances under which virtual clinical simulations should and should not be included as a learning activity?
What are the operational definitions of the key features of virtual clinical simulations? When should the term virtual reality clinical simulation is utilized in nursing and other disciplines? How will one know when to identify a phenomenon as a virtual reality (Figure 1) clinical simulation?
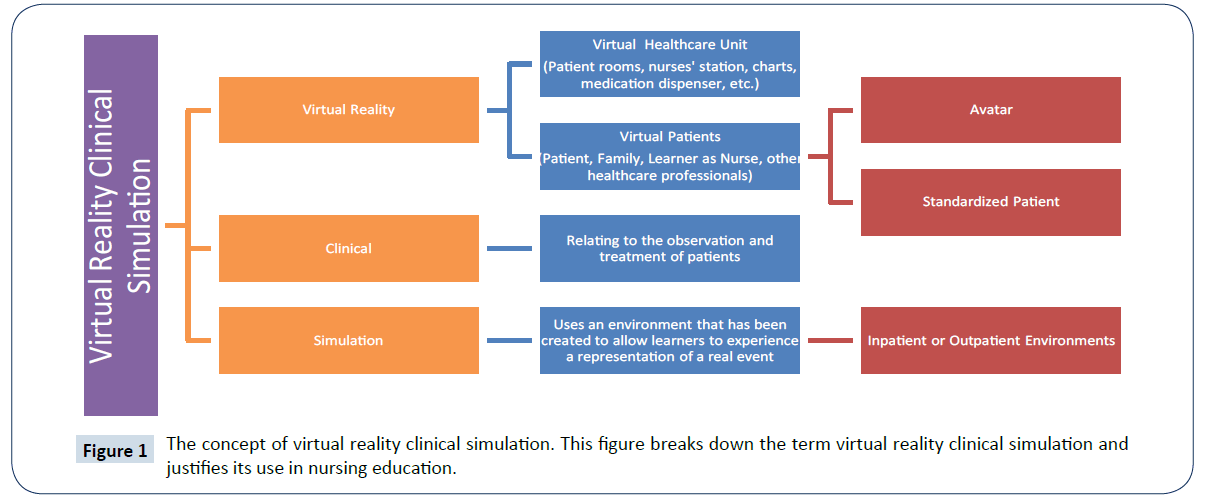
Figure 1: The concept of virtual reality clinical simulation. This figure breaks down the term virtual reality clinical simulation and justifies its use in nursing education.
The answers to these questions will be examined throughout the remainder of the text. In the examination of these questions 21 articles were identified from the literature that proved relevant to the concept of interest. These were collected from the following databases: EBSCO, Ovid, and CINAHL. The keywords utilized in the search of the literature included: virtual reality, clinical, simulation, e-simulation, and gaming. The articles identified consisted of qualitative and quantitative research studies, a meta-analysis, and expert opinions.
Findings
Exemplar and contrary cases: The third step in the Wilsonian concept analysis is to identify and describe exemplars of the critical features of the concept. Therefore, two exemplars of virtual clinical simulations are explained below. To follow these descriptions will include the typical characteristics of a virtual clinical simulation. Therefore, the following are model real-life cases [4].
Exemplar 1: An exemplar of virtual clinical simulation is the use of Second Life to create a virtual midwifery unit. Second Life is a social networking website that allows users to create virtual characters and avatars to explore a virtual 3-dimensional world. On this unit, pre-made characters are designed to represent women in labour and midwives. The midwife avatars represent the diversity of midwives in gender and race- one being white, black, Asian, and the other male. The midwife teacher then uses the pregnant avatar Gaia for the purpose of role play. The midwife teacher can direct the scenario of a woman’s labour virtually. As results, students are given the opportunity to practice several communication and theoretical management of care skills [6].
The scenario begins with the midwife avatar choosing rather a pool or bed setting can be changed according to a birth plan. Then the student is provided with a birth plan that is read on the computer, after which the student must select the appropriate birth environment and begins virtual care of Gaia. In all three stages, communication can be practiced via text chats or voice controls to represent speech; these can be printed off after completion of the scenario for discussion. Objects in the maternity unit virtual environment can be clicked on with the mouse so that information on such objects appears and can be stored away in inventory for the student [6].
The midwife teacher has the ability via a control panel to provide further information to the student about Gaia’s condition as her labour progresses. Information is provided on “various antenatal, intranasal and postnatal observations, such as blood pressure, contractions, degree of moulding, cervical dilatation, descent of the fetus, tone of the fundus, perineal trauma, Apgar score, and weight and feeding of the baby” [6].
Exemplar 2: Another example can be found in a narrative-based virtual patient simulation that is constructed based on a narrative clinical case scenario. These scenarios play before the learner via a computer screen, and there is a branching case structure that allows for various alternative pathways through a particular case. The central focus in the development of such scenarios are that an authentic clinical case scenario is authored and centered around a narrative that is realistic and large enough, with limited numbers of possible decision pathways through the case. Therefore, this type of virtual clinical simulation includes both an ideal pathway that contains the imperative stages of a case including alternative routes through the scenario [7].
Narrative feedback offered at each step of the pathways allows for each care decision to be linked to another. Therefore, those playing the scenario each base their next care decision on the feedback that was received at each step. When an adverse choice is made, the scenario will either end of allow the learner to make a reconsidered alternative grounded in the feedback received [7].
Typical and atypical features: Three main concepts are characteristic of virtual clinical simulations in both exemplars. The first is the learner interfacing the simulation via a computer. Both simulations were constructed to make them seem realistic to the user. The initial exemplar is accessed not only through a computer but also through an internet connection or network. The second feature is that a clinical scenario was provided for both exemplars for students to navigate through independently in a virtual clinical environment. The third common attribute is that the patients were portrayed as virtual patients or avatars.
The atypical features are the way in which they were controlled. The first exemplar is controlled solely by the teacher whereas the second exemplar has a predetermined path and feedback provided to the learner.
Contrary cases: The fourth step in the Wilsonian concept analysis is to find then contrary cases or examples that do not include any of the aforementioned typical properties of the concept exemplars for virtual clinical simulation. Meleis [4] compares contrary cases with exemplar cases stating, “Contrary cases may be extreme opposites of the exemplars, in that the concept is not readily visible or apparent”. Therefore, the contrary cases presented will be absent of the properties above of virtual clinical simulation.
A case totally contrary to virtual clinical simulation would be the use of simulation with the patient in the form of a low-high fidelity mannequin. Another clinical scenario that would be contrary to the ‘virtual aspect’ of VRCS is a standardized patient playing the role of the patient. Both of these modes of simulation are played out in the ‘real’ world whereas VRCS occurs in a totally created world which can be modified down to the very detail, unlike live simulation scenarios. There is a much greater level of control in the virtual environment. Such control is maintained in how the patient appears whether it is their race or bodily abnormalities, although they may not look as real as they appear on a standardized patient with moulage.
Borderline and related cases: Wilson confirms the sixth step of concept analysis to be the examination of borderline cases which “may have some features or attributes of the concepts and in which ambiguity exists about whether the case belongs to the concept or not” [4]. These borderline cases particularly are included because they help to develop further the concept of virtual clinical simulation.
Borderline and related cases: Cant and Cooper [1] completed an integrative review of web-based simulation in nursing education. Eighteen studies included 18 studies of web-based simulation programs: three of which were non-randomized case-control studies, six being quasi-experimental cross-sectional studies; three were qualitative program evaluations and three observational reports. In this literature review, there was obvious confusion as to the terminology referring to the modes of delivery of computer-based simulation. There was disunity about the nomenclature. Computer-based simulation was referred to in several ways including virtual patient simulation [7], virtual simulation [8], computerized virtual patients [9], virtual clinical simulation [10], cybergogy [10], e-simulation [11,12], and web-based simulation [13].
The terms ‘e-simulation’ and ‘virtual clinical education’ have similar meanings. According to the Australia Learning and Teaching Council, e-simulation involves ‘goal-based digital simulations that take place via a computer screen’ [1]. According to the Society for Simulation in Healthcare [14], ‘virtual reality simulations’ are "simulations that use a variety of enhanced technology to enhance reality in order to replicate real-life situations and/or healthcare procedures”. These definitions infer that such a simulation mode of education takes place via some technology such as a computer. They also point out that there is a goal related to such simulation. Whereas, e-simulation occurs only via a computer screen, virtual reality simulation includes various forms of enhanced technology such as video, the internet, and perhaps 3-dimensional glasses. The term ‘virtual clinical simulation’ is more specific in nature in its confinement to clinical healthcare situations, procedures, or skills.
This is similar to the term ‘computer-based simulation’ that are simulation activities that are performed in the mode of technology; in this case, it being a computer. Although they are similar to ‘virtual clinical simulations’, they do not include additional interfaces between the student and the computer. For example, they are restricted to the mouse as an interface [1].
There are various modes reported that which a ‘computer-based simulation’ can be delivered. Of Cant and Cooper’s [1] review, there was a lack of consensus concerning this nomenclature as well. Some studies explained ‘virtual’ simulation as involving only animated human characters whereas others displayed patients as standardized patients or human actors. Conversely, ‘virtual reality simulations’ are described as “incorporating physical or other interfaces (such as surgical instrumentation) that readily replicate the actions required in a given situation or setting”. Other studies referred to ‘virtual’ simulation as a mode of presentation on a computer screen alone.
‘Web-Based Simulation’ occurs on a computer but also takes place online. It is defined by Cant and Cooper [1] as “combining electronic multimedia options with a central video or virtual world to produce interactive learning mediated by the learner”. From the term, web-based learning seems to have developed ‘simulation-based e-learning’ or ‘e-simulation’ which combines the pedagogies of face-to-face simulation with electronic multimedia to create activities that are interactive and learner-mediated. Such programs are hosted on the Internet website and are accessed via the World Wide Web using the navigable software. However, Cant and Cooper [1] clarify that the term ‘web-based simulation’ could occur with the utilizations of a local electronic source such as a DVD or CD-ROM.
The invented case: In addition to exemplars, contrary, related, and borderline cases the concept analysis must create an invented case that exemplified those typical features and properties of a concept. This allows for the major features of the concept to be highlighted and perhaps enhanced. Meleis [4] describes the invented case as possibly having a different context, being ‘totally out of the ordinary and that it should be completed in an innovative way. The following is the author’s attempt to describe an invented case of a virtual clinical simulation.
The learner logs into a secure website with a username and password. After logging in, they are presented with several sets of clinical scenario titles based on the textbook reading that was assigned this week by their clinical professor. This week the student learned about diabetes and, therefore, opens a two-part diabetes clinical scenario. Once this scenario is opened, the students are asked to log in with their name, the shift they are working in the scenario, how many patients they are to be assigned, and what type of unit they are working on. This way the website can remember the student’s name when speaking to the learner and letting the student know what is going on in the scenario. It also will allow the theoretical and clinical professors to track the progress of each learner in clinical scenarios that have been assigned. The learner will take on the role of the nurse. Once logged in with all the specifics of the assigned information, the student will be instructed to don virtual glasses that will provide a 4-dimensional environment that will simulate a live 360 degree medical-surgical clinical unit.
The student begins the scenario by being given a report by a standardized nurse or human actor acting as a nurse. Both the audio and written report are provided before the student decides to enter the hospital unit from the nursing desk. At the nursing desk also exists a computer which when clicked has a simulated electronic health record system that includes all documentation in the chart and more. The electronic record would include but not be limited to: history and physical, previous shift nurse assessments and the ability of the learner to chart a shift assessment, the medication administration record, laboratory and radiology reports, previous consultants transcribed reports, an interdisciplinary care plan, and much more. If the learner decides not to access the computer, they can click on several links which will take them to either: their assigned patient rooms, the medication room, the clean and soiled utility, the break room, and the supply room.
Once entering the patient room a simulated patient will be available who the learner can type in text or use a microphone to communicate with whom will then respond to such communication according to the signs and symptoms the patient in the scenario would have. There would be a voice activated digital link, once the student enters the room, to enable the learner to document any detailed part of a head-to-toe assessment, or implement an intervention. If an intervention requires medications or supplies, the links to the several locations would be available as well as to contact a physician, nurse manager, supervisor, or unlicensed assistive personnel. The patient will be a simulated standardized patient with all the abilities of a real patient including ambulation with the learner outside the patient room and to be sent off the unit to diagnostic tests and surgery if needed. After completion of any intervention, the student would be able to document the procedure in the electronic health record via a simulated computer that will be available in the patient room.
Simulated friends, families, and visitors will be able to enter the unit as well as other nurses, physicians, case managers, social workers, and other interdisciplinary staff. These other health care professionals and avatars may interact with the learner if they have a concern about the student’s assigned patient. Again, the student may respond by either utilizing the keyboard to type a response or a microphone to speak a response to the avatar approaching them.
Alerts will become available when new laboratory values, radiologic reports, or any other important documentation appears in the electronic record. There also will be a phone available for the avatar to have to experience the everyday communication that may occur with other healthcare professionals, the patient, and family members.
The Social Context and History of Virtual Reality Simulation
Wilson [5] explains that that one must identify and define the social contexts of the concept during a concept analysis. The concept must be analyzed from the eye of the individual who may use the phenomenon, why it is used, and how it is used. Concepts that occur within a social context encompass both the past and future. Time and context are what create meanings for a concept. Meleis [4] explains that such meanings are derived from “a social context, and interpretations differ across disciplines, time spans, regions, and cultures”. Therefore, the following will explain the concept of virtual clinical education in the social content and historically, from its start.
Virtual reality simulation has been used for over four decades. In the late 1950’s, Douglass Engelhart took on a different view of the hulking computers that existed then, which many considered only as ‘glorified adding machines.' Engelhart began to envision them as a tool for which digital displays could be shown. As an expert in radar and digital technology, he reasoned that a computer connected to a screen could be used to solve problems. By the following decade, many other scientists began to think the same way. Therefore, his vision came to life as computing and graphic technology collided to make the first computers based on transistors. The synergy of these two fields was the start of user-friendly computers, personal computers, computer graphics, and eventually the commencement of virtual reality simulation [15].
One of the greatest antecedents of virtual reality simulation was the invention of the flight simulator. After World War II, the government funded the military and industrial complexes with millions of dollars to simulate the flying of airplanes, driving of combat tanks, and even steering ships. This allowed pilots to be trained on the ground safely before putting them at risk if the dangers of true flight. The earliest simulators had mock cockpits that were built on motion platforms that were able to pitch and roll. The downside of this technology was the lack of visual feedback. Nevertheless, soon video displays were combined with such mock cockpits. By the 1970’s, primitive computer generated graphics was replaced with videos and models allowing flight simulation to operate in real time. By 1979, military technologists had begun to use head-mounted displays. However, by the 1980’s, as a consequence of improved software, hardware, and motion control simulators, pilots were then enabled to travel through virtual worlds that were highly detailed. Nevertheless, other industries soon became interested in computer graphics [15].
The entertainment industry became a natural consumer of computer graphics. American film utilized computer-generated special effects such as the battle scenes in the famous science fiction movie Star Wars, which was first released in 1976. Soon after such movies as Terminator and Jurassic Park also were hits and known for their dazzling use of special effects. By the 1980’s, the video game business began to prosper [15].
As the world of gaming boomed, the field of scientific visualization evolved from bar charts and line drawings to lively images. Whereas they had previously used columns and numbers to attempt to understand DNA sequences, molecular modules, brain maps, and cosmic explosions. The goal of such scientific visualization “to capture the dynamic qualities of systems or processes in its images”. Such animation was so influential that an animation of smog descending upon Los Angeles, in 1990, won a national award for influencing the legislation of air pollution in the state. This animation acted as a compelling testament to the worth of such type of imagery. Despite the value of such imagery, scientists, the military, businesses, and entertainment wanted more. They demanded interactivity and visualization environments with which they received after high-performance computers were developed in the mid-1980. Today enhanced high-performance computers allow for computation and virtual reality and no longer act as number crunchers and document creators but have become ‘exciting vehicles for exploration and discovery’ [15].
Reeves and Reeves [16] explain how e-learning or computerbased learning grew exponentially as education courses began to be offered online. This enabled students to learn at their personal pace. E-learning developed in nursing originally when a need developed to disseminate information widely and to incorporate discussion groups in a textual format [17]. As a result, traditionally, e-learning was limited to the asynchronous discussion but it lacked the authenticity of experiential learning. However as aforementioned, “mixed media dimensions of the classroom were transferable to e-learning, including text graphics, sound, vision, color, animation, and video.” These approaches allowed a unique educational experience to learners with a significant amount of beneficial resources compared to other teaching methods. Computer-mediated modes of communication within the e-learning model include self-directed learning modules, podcasts, and video-enhanced programs. Virtual clinical education is a more technologically sophisticated interactive simulation-based, web-based learning mode which is now available [1].
The last decade saw an explosion of possibilities of virtual environments with the development of immersive and engaging virtual environments in engaging higher education learning experiences. In 2004, Linden Lab released Second Life, which has now become one of the world’s most populated and explored virtual environment for a plethora of educational purposes. Currently, there are 20 million virtual residents with over 70,000 people accessing the site daily. Of these, there are over 700 educational institutions who have a presence on Second Life. Within nursing schools, Second Life has been used for simulation in online theoretical and clinical experiences [1].
Today’s nursing students are more ‘tech savvy’ than ever before. They have high expectations of animations, interactions, and visual activities. They are computer literate and use an overabundance of multimedia technologies. The growing trend in electronic communications for both teaching and learning has led to students’ strong acceptance of online learning. Many millennial play virtual games at home which simulate many types of activities that range from fighting to racing. Deakin University [18] reports that simulation-based e-learning allows it learners to be immersed in computer-based simulation which immerses the student in “realistic context relying upon programs that are accessed directly from the Internet, downloaded as an application, or viewed on a DVD”.
The Morality of Virtual Clinical Simulation
The Wilsonian method requires that a concept’s unresolved issues be discussed. There are several barriers encountered by virtual clinical simulations currently. The boundaries of virtual reality simulation in nursing are the expense incurred. They are time-consuming to build, implement, and maintain. As a result, the wider use of the application has been prohibited [19,20].
They often are context and discipline specific. They also often require extensive technical skills. Therefore, students who prefer traditional teaching methods may be uncomfortable with the active learning principles that underpin simulation [21,22]. There is also the potential in speed through network traffic. The vulnerability of security issues must also be addressed. These are circumstances when not accounted for the technology of virtual clinical education should not be used [1].
Waldner and Olson [23] argue that virtual simulation clinical education lacks a comprehensive theoretical framework to support and guide its use. There also has been the critique that there is limited conclusive empirical evidence of its impact on learner outcomes. Further, there is the argument that there exists a poor understanding of the purposes and directions of simulation and that it lacks expressions of expected goals and outcomes of its utilization [24].
On the other hand, there are benefits under which this form of simulation should be included as a learning activity. First, it is interactive, stimulating, and enjoyable for learners. It may be accessed for single-user or group interaction. It provides realistic and real-world scenarios while reducing the face-to-face time and teaching resources. This form of simulation enables control and predictable outcomes while also promoting trial and error learning since it provides a risk-free environment. Lastly, it is widely available, yet access can be controlled via password protection [25].
The virtues of VRCS’s include their timeliness, relevance, measurability, and ‘delightfulness’ according to Koerner. It can be accessed anywhere at any time. The new learning platform architecture allows for modification of information to occur at the moment a research finding is broadcast to the nursing field rather than 5 to 7 years lag of time. Also with high-risk-low-volume events, nursing students may go online and utilize the learning activity for initial and refreshing of such skills to ensure competency in performance.
The virtual assessment also allows for true objectivity that was never possible before. Likewise, the sophisticated logic and tracking of work enables the learner to see the consequence of every action they take. Dashboards and instructors can provide students with a map of their individual reasoning so that verification of competence can occur. Also, it allows for the amplification of mental models that are incorrect for a given clinical situation. The “free-play” environment allows the learner to practice new and forgotten skills without putting patient safety at risk. This way the material the learner needs to know is targeted, and learners can bypass what competency they already possess. By honouring current knowledge and skills, it maintains the interest of the learner and their attention throughout the process of learning.
The National Council State Boards of Nursing points out that innovative strategies such as virtual clinical simulation should only be conducted in a manner that protects the public and in a way that conforms to the quality outcome standards and core education criteria established by the Board of Nursing. They explain the key point in implementing such innovative strategies is that it “will not compromise the quality of education or safe practice of students” (https://ncsbn.org/NSNA_09_Innovations.pdf). In recognition of these risks of implementation of highly innovative teaching strategies, Jenson and Forsyth explain that increased patient acuity, high student-to-faculty ratios, and student anxiety already are putting the population at risk for harm.
Due to increased patient acuity, students may not have sufficient time to participate in clinical experiences in their practicum. Nevertheless, higher acuity virtual patient scenarios provide the opportunity to be faced with those situations and assessed for competency. Based on such an assessment, the student and faculty will be able to identify and work on individual weaknesses in clinical practice before entering the profession.
Due to high student-to-faculty ratio, currently nursing clinical faculty cannot fully evaluate each student as closely as they wish to. However, virtual clinical simulation “allows faculty to review student progress from a computer at any time, which will alleviate faculty workload and foster patient safety”.
Lastly, student anxiety also plays a threat to the public during their live clinical practicum. “Virtual reality can assist in decreasing student anxiety and enhancing student confidence by allowing unlimited practice of clinical scenarios in a risk-free environment while also providing feedback via the computer during and after the scenario”. Therefore, students will be ensured that they utilize proper and consistent techniques [26].
Conclusion
Labelling the concept
The final step of the Wilsonian approach to concept analysis is to “carefully choose the language to describe the results and label the concept” [4]. It is recommended that a decision be made on the best words to use which correctly reflect the concept and its meaning. Meleis [4] explains that due to words having multiple meaning and perhaps ambiguous interpretations, it is imperative to determine a single meaning and label it accordingly.
Virtual reality clinical education (VRCS) is the term that has been chosen to label the ideal virtual clinical simulation. It includes the words ‘virtual reality’ which means a “computer-generated simulation of a three-dimensional image or environment that can be interacted with in a seemingly real or physical way by a person using special electronic equipment, such as a helmet with a screen inside or gloves fitted with sensors” (https://www.oxforddictionaries.com/us/definition/american_english/virtualreality?q=virtual+reality). This was chosen instead of virtual clinical education because the term ‘virtual’ is more general in nature whereas the term ‘virtual reality’ is more specific.
The word virtual means, ‘carried out, accessed, or stored using a computer, especially over a network’ (https://www.oxforddictionaries.com/us/definition/american_english/clinical). Realism refers to “the ability to impart the suspension of disbelief to the learner by creating an environment that mimics that of the learner’s work environment. Realism includes the environment, simulated patient, and activities of the educators, assessors, and facilitators” [14]. By combining the words ‘virtual’ and ‘reality’ it more aptly describes what occurs in virtual simulation and the situated cognition that can take place.
In such virtual scenarios, patients are observed and taken care of virtually based on theoretical knowledge. Therefore, it is appropriate that the word ‘clinical’ is utilized to describe this form of virtual reality simulation. Therefore, it cannot be confused with the term ‘virtual reality simulation’ that often is related to recreational gaming rather than a learning activity. The adjective clinical appropriately refers to, ‘of or relating to the observation and treatment of actual patients rather than theoretical or laboratory studies’ (https://www.oxforddictionaries.com/us/definition/american_english/clinical).
Simulation is the appropriate noun due to it's being a technique that uses an environment that has been created to allow learners to experience a representation of a real event for various purposes. The purpose of a simulation can be for practice, learning, evaluation, testing, or to understand the systems or human actions, in this case, the actions of a nurse. Often, simulation is used in the context of assessment or training [14].
References
- Cant RP, Cooper SJ (2014) Simulation in the internet age: The place of web-based simulation in nursing education. An integrative approach. Nurse Educ Today 34: 1435-1442.
- Jensen CE, Forsyth DM (2012) Virtual reality simulation: Using three-dimensional technology to teach nursing students. Comput Inform Nurs 30: 312-318.
- Warburton S (2009) Second Life in higher education: Assessing the potential for and the barriers to deploying virtual worlds in learning and teaching. Br J Educ Technol 40: 414-426.
- Meleis AI (2012) Theoretical nursing: development and progress. Philadelphia: Wolters Kluwer & Lippincott Williams and Wilkins.
- Wilson J (1969) Thinking with concepts. New York: Press Syndicate of the University of Cambridge.
- Bailey J (2012) The age of virtual learning. Midwives p: 1.
- Guise V, Chambers M, Valimaki M (2011) What can virtual patient simulation offer mental health nursing education? J Psychiatric Ment Health Nurs 19: 410-418.
- Sweigart L, Burden M, Hodson Carlton K, Filwalk J (2014) Virtual simulations across curriculum prepare nursing students for patient interviews. Clin Simulat Nurs 10: 139-145.
- Cook DA, Erwin PJ, Trioola MM (2010) Computerized virtual patients in health professions education: A systematic review and meta-analysis. Acad Med 85: 1589-1602.
- Foronda C, Godsall L, Trybulski J (2013) Virtual clinical simulation: The state of the science. Clin Simulat Nurs 9: 279-286.
- Lamont S, Brunero S (2013) eSimuation part 1: Development of an interactive multimedia mental health education program for generalist nurses. Collegian 20: 239-247.
- Lamont S, Brunero S (2013) eSimuation part 2: Evaluation of an interactive multimedia mental health education program for generalists nurses. Collegian.
- Cooper S, Beauchamp A, Bogossian F, Bucknall T, Cant R, et al. (2012) Managing patient deterioration: A protocol for enhancing student nurses’ competence through web-based simulation and feedback techniques. BMC Nurs p: 11.
- https://www.ssih.org/Portals/48/Certification/CHSE_Docs/CHSE%20Handbook.pdf
- https://archive.ncsa.illinois.edu/Cyberia/VETopLevels/VR.History.html
- Reeves PM, Reeves TC (2008) Design considerations for online learning in health and social work education. Learning Health Social Care 7: 46-58.
- Moule P, Wilford A, Sales R, Lockyer L (2008) Student experiences and mentor views of the use of simulation for learning. Nurse Educ Today 34: 790-797.
- www.deakin.edu.au/itl/assets/resources/e-simmoduleplan-v2ss002.pdf
- Conradi E, Poulton T, Round J (2007) Teaching decision-making skills through virtual scenarios. 10th IASTED International Conference on Computers and Advanced Technology in Education, Calgary: ACTA Press, Beijing, China.
- Nehring WM, Lashley FR (2009) Nursing simulation: A review of the past 40 years. Simul Gaming 40: 528-552.
- Royse MA, Newton SE (2007) How gaming is used as an innovative strategy for nursing education. Nurs Educ Perspect 28: 263-267.
- Peddle M (2011) Simulation gaming in nurse education: entertaining or learning? Nurs Educ Today 31: 647-649.
- Waldner MH, Olson JK (2007) Taking the patient to the classroom: Applying theoretical frameworks to simulation in nursing education. Int J Nurs Educ Scholar 4: 1-14.
- Schiavenato M (2009) Re-evaluating simulation in nursing education: Beyond the human patient simulator. J Nurs Educ 48: 388-394.
- Byrne J, Heveya C, Byrne P (2010) A review of web-based simulation and supporting tools. Simulation Models of Practical Theory 18: 253-278.
- Cook LJ (2006) Inviting teaching behaviors of clinical faculty and nursing students’ anxiety. J Nurs Educ 44: 156-161.

