Keywords
Muscle tumors; Neoplasms; Clinical behavior; Gastrointestinal tract; Necrosis
Introduction
Uterine leiomyoma are the most common benign tumor diagnosed in women [1]. The majority of these leiomyomas are benign with malignancy accounting for only about 1% of all uterine smooth muscle tumors [2]. There is however another subtype of leiomyoma that is relatively uncommon. The World Health Organization (WHO) classifies this other subtype as a uterine smooth muscle tumor of uncertain malignant potential (STUMP) [1-4]. The term “STUMP” was first used in the literature in 1973, and continued understanding and comprehension of these entitles are necessary. Various manuscripts classify STUMP with leiomyoma variants as they share histologic criteria, however others strictly separate these groups due to the unknown malignant potential of STUMP tumors. STUMP tumors therefore create a dilemma from the standpoint of histologic diagnosis, classification, and appropriate treatment [5-10]. Research is ongoing with clinical management guidelines and post-operative surveillance remaining elusive.
Pathophysiology
Extensive work has been performed to characterize cellular mechanisms of myometrial tissue and neoplasmic growth leiomyoma. Normal myometrial tissue contains stem cells responsible for its own proliferation and self-renewal under regulated processes. Smooth muscle cells will undergo multiple cycles of growth and involution from physiologic ovarian hormone stimulation under estrogen and progesterone in the reproductive age female [8,10,11]. These cells also receive indirect paracrine signaling from stem cells to create a regulated physiologic process on the uterine myometrium. Repeated physiologic stimulation of hormonal and paracrine signals have the potential to create genetic mutations and chromosomal rearrangements in myometrial stem cells [8]. Mutations influencing regulated genetic processes then cause unregulated self-renewal and proliferation. Several observations support the notion that a single somatic mutation arises in a myometrial cell that then alters normal cellular mechanisms involving regulation, signaling, growth, and destruction [8,12,13]. There are a spectrum of outcomes to include benign leiomyoma vs leiomyosarcoma growth. Some of the mutations have been shown to involve the mediator complex subunit 12 (MED12), wingless-type MMTV integration (WNT) with the B-catenin pathway, T-cell transcription factor (TGF), transforming growth factor B3 (TGF-B3), fumarate hydratase among others [8,11,14,15].
Leiomyomas frequently harbor recurrent deletions affecting 7q22, 22q, and 1p suggesting that these regions contain tumor suppressor genes [15]. Several locations and regions have been identified that can lead to the development of leiomyomas. Deletions of 1p have specifically been associated with distinct histopathological features and possible malignant progression of leiomyomas. Mehine et al. and Hodge et al. confirmed a malignant behavior in myometrial cells containing the chromosome 1p deletion. Further identification and classification of chromosomal mutations and signaling pathways will aide in correct diagnosis and management [11,16,17].
Deletions and mutations in the 12q4 gene have been characterized and seen to have MED12 gene mutations. Schwetye et al. discovered that the presence of exon 2 MED12 mutations could help distinguish between which extra-uterine tumors that were hormonally responsive [17,18]. The group noticed that Mullerian-derived tissues (the pelvis and retroperitoneum) developed extra-uterine tumors in which 34% of patients (10/29) had the exon 2 MED12 mutation and thought to all be hormonally responsive, and the extra-uterine tumors that occurred in the gastrointestinal tract, dermis, urinary system, and vasculature, did were not seen to have the exon 2 MED12 mutation (0/29) and all thought to not be hormonally responsive [14,15,18].
Leiomyomas with high mobility group AT-hook 2 (HMGA2) mutations displayed an up-regulation of the proto-oncogene pleomorphic adenoma gene 1 (PLAG1), suggesting that HMGA2 can promote tumorigenesis through PLAG1 activation [17]. An accumulation of fumarate has been thought to lead to activation of the oncogenic transcription factor nuclear factor erythroid 2-related factor 2 (NRF2) which is another oncogenic protein. These new genetic mutations emphasize the need for further studies in molecular research [17].
Classification
No single morphologic feature clearly separates uterine smooth muscle tumors into benign or malignant histologic types. The classification of uterine smooth muscle tumors is based on the assessment of three histopathologic characteristics: Mitotic count activity or mitotic index (number of mitotic figures per 10 high power fields [hpf]), presence of coagulative tumor cell necrosis, and degree of cytological atypia [19-22]. Accurately diagnosing uterine smooth muscle neoplasms is clinically significant for correct patient management. The correct diagnosis of STUMP tumors however can be challenging as many histologic characteristics overlap with rare subtypes of leiomyoma variants [2,3,19,23].
Diagnosis of cellular atypia is more clearly defined in Kempson and Hendrickson by the use of a two tiered scheme to classify atypia into insignificant (absent to mild atypia) and significant (moderate to severe atypia) [19,24,25]. Degree of atypia is based on an assessment of nuclear pleomorphism, nuclear size, nuclear membrane irregularities, chromatin density, and the size and prominence of nucleoli. Tumors with absent atypia are comprised of smooth muscle cells with uniform nuclei that may be enlarged but have smooth nuclear contours and evenly distributed chromatin. Tumors with mild atypia show minimal variation in nuclear size and shape with small nucleoli. Tumors with moderate atypia have cells with nuclei that are large, plump, and irregular with coarse chromatin and the presence of at least two enlarged abnormal mitotic figures. Tumors with severe atypia have obvious nuclear pleomorphism and cells with enlarged bizarre nuclei with dense chromatin [19,21,26,27].
Mitotic index is based on the number of mitotic figures per 10 hpf. Using specific criteria is beneficial to aide in accurate diagnosis.
1) Hairy extensions of chromatin (condensed chromosomes) must be present, extending from a central clot-like dense mass of chromosomes. The clots may be single (metaphase) or separate (telophase). Hairy extensions from an empty center favor nonmitosis.
2) The nuclear membrane must be absent, but the cytoplasm is often discernible.
3) Differential diagnosis: Lymphocytes, mast cells, stripped nuclei, degenerated cells, precipitated hematoxylin [19,21,26,27].
Two types of necrosis are found in uterine smooth muscle tumors: Coagulative tumor cell necrosis and hyalinizing necrosis. Coagulative tumor cell necrosis features an abrupt transition between necrotic cells and preserved cells. Outlines of the nuclei from the necrotic cells can often be seen, and inflammatory cells are uncommon. This pattern of necrosis is common in clinically malignant smooth muscle tumors. In contrast, hyalinizing necrosis features a zone of hyalinized collagen interposed between the dead cells and the preserved cells, a pattern reminiscent of an infarcted region being organized by granulation tissue. Hyalinizing necrosis is common in leiomyomas, however is not helpful in predicting the malignant potential of a smooth muscle tumor [11,19,21,26,27].
The WHO classifies leiomyoma variants as benign and with low risk of recurrence:
1) Mitotically active leiomyoma: These tumors have the macroscopic and histological appearance of a leiomyoma with the exception of having >5 mitosis/10 hpf. No cytologic atypia or tumor cell necrosis should be found.
2) Mitotically active leiomyoma with limited experience: These tumors contain >15 mitosis/10 hpf. No cytologic atypia or tumor cell necrosis should be found.
3) Cellular leiomyoma: These tumors are defined as tissue with cellularity that is ‘significantly’ greater than that of the surrounding myometrium. These lack tumor cell necrosis, are without moderate or severe atypia, and with infrequent mitotic figures.
4) Atypical leiomyoma (pleomorphic, bizarre or symplastic leiomyoma): Enlarged hyperchromatic nuclei with prominent chromatin clumping. Large cytoplasmic pseudonuclear inclusions are present. The atypical cells may be distributed throughout the leiomyoma (diffuse) or they may be present focally (possibly multifolcally). No tumor cell necrosis or have ≤10 mitosis/10 hpf should be found in Figures 1A-1G [4,17,19,21,27].

Figure 1A: Leiomyomas are composed of uniform smooth muscle cells arranged in whorled anastomosing fascicles. Cytologically, smooth muscle cells are spindly, with indistinct cytoplasmic borders and a fibrillary eosinophilic cytoplasm. Nuclei are ovoid to elongate with blunt ends. The chromatin is open and occasionally an inconspicuous nucleolus is seen. Rare mitosis or none is characteristic of typical leiomyomas.
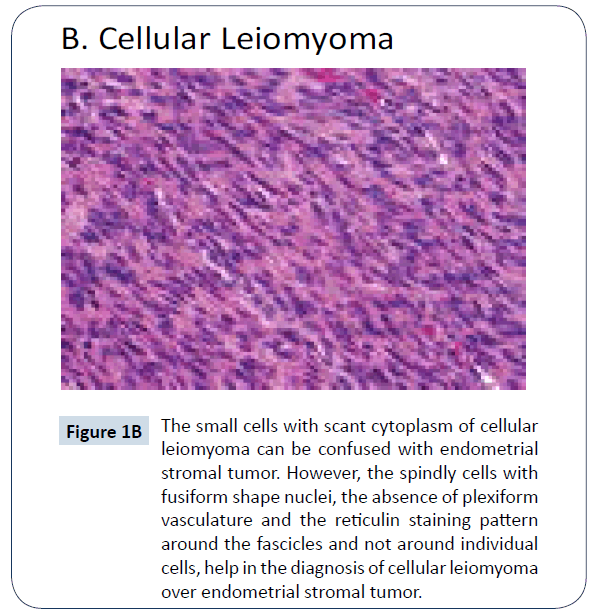
Figure 1B: The small cells with scant cytoplasm of cellular leiomyoma can be confused with endometrial stromal tumor. However, the spindly cells with fusiform shape nuclei, the absence of plexiform vasculature and the reticulin staining pattern around the fascicles and not around individual cells, help in the diagnosis of cellular leiomyoma over endometrial stromal tumor.
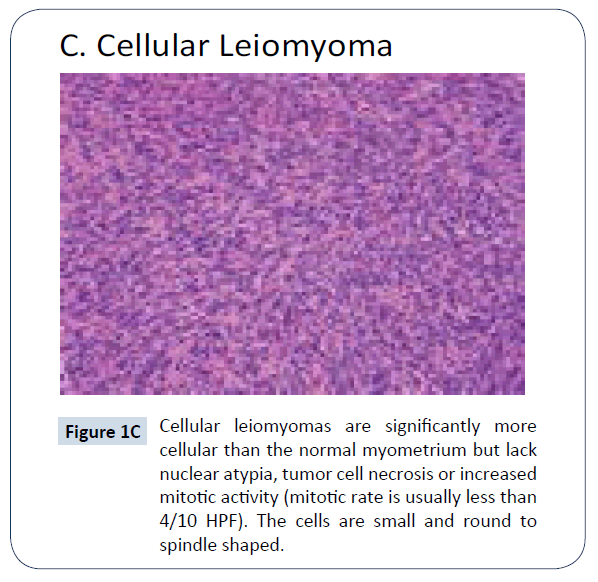
Figure 1C: Cellular leiomyomas are significantly mor e cellular than the normal myometrium but lack nuclear atypia, tumor cell necrosis or increased mitotic activity (mitotic rate is usually less than 4/10 HPF). The cells are small and round to spindle shaped.
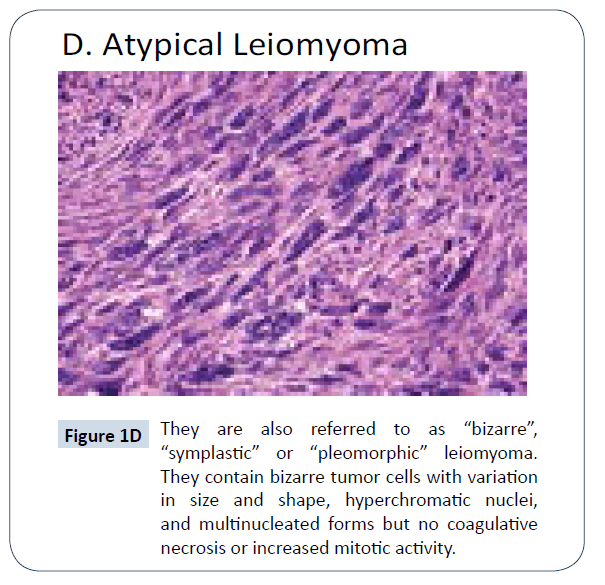
Figure 1D: They are also referred to as “bizarre” , “symplastic” or “pleomorphic” leiomyoma. They contain bizarre tumor cells with variation in size and shape, hyperchromatic nuclei, and multinucleated forms but no coagulative necrosis or increased mitotic activity.
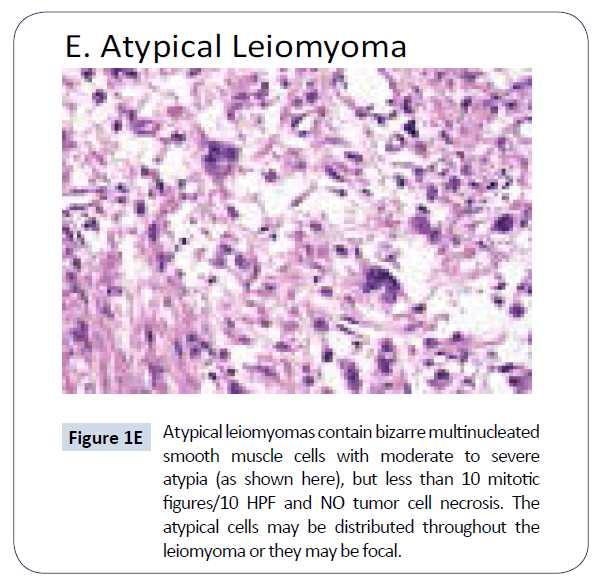
Figure 1E: Atypical leiomyomas contain bizarre multinucleated smooth muscle cells with moderate to severe atypia (as shown here), but less than 10 mitotic figures/10 HPF and NO tumor cell necrosis. The atypical cells may be distributed throughout the leiomyoma or they may be focal.
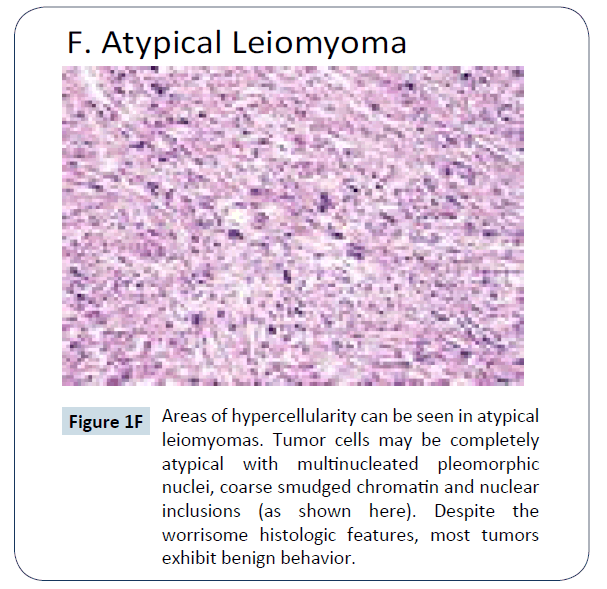
Figure 1F: Areas of hypercellularity can be seen in atypica l leiomyomas. Tumor cells may be completely atypical with multinucleated pleomorphic nuclei, coarse smudged chromatin and nuclear inclusions (as shown here). Despite the worrisome histologic features, most tumors exhibit benign behavior.
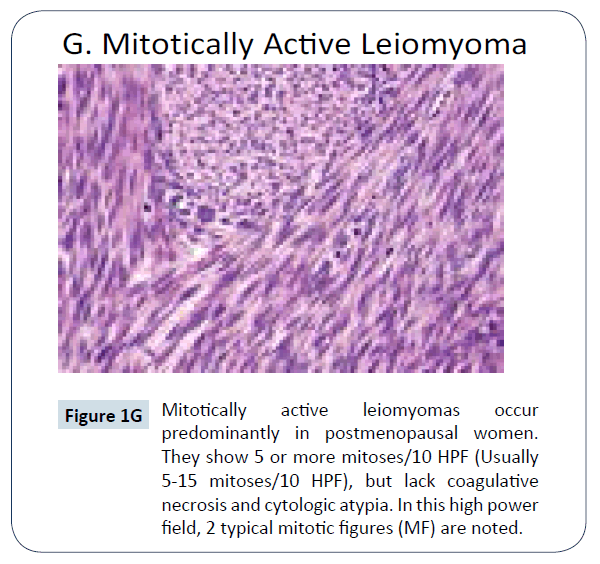
Figure 1G: Mitotically active leiomyomas oc cur predominantly in postmenopausal women. They show 5 or more mitoses/10 HPF (Usually 5-15 mitoses/10 HPF), but lack coagulative necrosis and cytologic atypia. In this high power field, 2 typical mitotic figures (MF) are noted.
Bell et al. proposed criteria to classify STUMP tumors divided into 4 categories based upon the degree of cellular atypia, presence of coagulative necrosis, and mitotic index [1-4,9].
1) Atypical leiomyoma: Diffuse moderate to severe cellular atypia without coagulative cell necrosis and a mitotic index <10 mitotic figures/10 hpf.
2) Atypical leiomyoma with limited recurrence: Focal or multifocal moderate to severe atypia without coagulative cell necrosis and a mitotic index <20 mitotic figures/10 hpf.
3) Leiomyomas with increased mitotic activity but limited recurrence: Without atypia or mild atypia without coagulative necrosis with mitotic index ≥ 20 mitotic figures/10 hpf
4) Smooth muscle tumors of low malignant potential: Without atypia or mild atypia with coagulative necrosis with mitotic index <10 mitotic figures/10 hpf (Figures 1A- 1G) [1-3,21,27].
Having a diagnostic strategy to evaluate smooth muscle tumors proves to be beneficial. This is adapted from Kempson and Hendrickson [19,28]:
1) First look at types of atypia along with presence of tumor cell necrosis:
• If atypia is absent or mild and tumor cell necrosis is absent, then the tumor is a leiomyoma.
• If there is moderate to severe atypia, without tumor cell necrosis, stratification is based on the mitotic index as follows: Less than 10 mf/10 hpf: The tumor is an atypical leiomyoma; and Greater than 10 mf/10 hpf: The tumor is a leiomyosarcoma.
2) If both moderate to severe atypia and tumor cell necrosis are present, the tumor is a leiomyosarcoma whatever the mitotic index.
Clinical Symptoms
Clinical presentation and symptoms of STUMP included pelvic mass, heavy uterine bleeding, bulk symptoms of fibroids, dysmenorrhea, infertility, pelvic pressure, abnormal vaginal discharge, intermenstrual bleeding among others. The risk factors and biological events that lead to STUMP remain poorly understood and thus subsequent clinical behavior difficult to predict. Median age at time of presentation is similar to leiomyoma [7,25,26].
Diagnostic Imaging
Imagining studies have been attempted to determine benign from malignant uterine smooth muscle tumors. However there is no reliable method to pre-operatively clarify benign from malignant tumors [29]. Ultrasound imaging has only limited information on uterine smooth muscle tumors. There are no specific ultrasound features described for STUMP tumors compared with fibroids, however more aggressive tumors such as sarcomas, may be unable to be distinguished with the appearance as an irregularly vascularize mass, with a regular or irregular outline, often with irregular anechoic areas due to necrosis. Data on prediction of uterine sarcoma diagnosed by sonogram is scarce and based mainly on small retrospective case series at the current time [30,31].
Although certain MRI features may indicate differences in tissue intensity, there are no definitive imaging findings that reliably determine ordinary leiomyomas from leiomyoma variants. The available evidence suggests that hypointense T1 signal, moderate T2 signal intensity, and high signal intensity on DWI are not typical findings of ordinary leiomyomas, and thus, if present, especially in combination, might raise the possibility of a leiomyoma variant or STUMP [32]. Sato et al. in a retrospective study investigated the application of MRI Diffusion Weighted Imaging (DWI) and Apparent Diffusion Coefficients (ADC) to differentiate benign leiomyomas from leiomyosarcoma. Results from DWI alone showed that low intensity lesions were all benign leiomyomas, however intermediate and high intensity lesions were considered indicative of leiomyosarcomas and thus the ADC value was measured. Leiomyoma ADC value was found to be ≥ 1.1 (× 10-3 mm2/s) and was low risk verses a diagnosis of leiomyosarcoma with a ADC value <1.1 (× 10-3 mm2/s) and determined to be high risk. Analyses comparing the low-risk group with that of the high risk with combined DWI and ADC values yielded the following: Sensitivity of 100%, Specificity of 94%, positive predictive value of 100% and accuracy of 94.6% [29].
The utility of Positron Emission Tomography/Computed Tomography (PET/CT) to differentiate ordinary leiomyomas, leiomyomas variants, and leiomyosarcomas remains limited because ordinary leiomyomas can take up Fluorodeoxyglucose (FDG) on PET (as a marker for cellular proliferation) [33]. It is still difficult to accurately determine uterine sarcoma from STUMP tumors or cellular leiomyoma [29-33].
Immunohistochemistry
Histologic distinction between malignant and benign smooth muscle tumors remains challenging. Numerous small series have investigated the use of immunohistochemical marker expression profiles to aid in the exact diagnosis of smooth muscle tumors. A significant difference in staining intensity can further delineate STUMP from benign and malignant counterparts [34,35].
Various cell cycle regulatory proteins and tissue expression may have the potential for diagnostic utility [36,37]. Ki-67 is a non-histone nuclear protein only expressed in G1-M phases of the cell cycle, used as a marker of cellular proliferation. p16 is a tumor suppressor protein that binds to cyclin dependent kinase 4 creating a p16–CDK4 complex that inhibits cellular growth [23]. Application of pHH3 has been proven as a novel proliferation marker expressed in the late G2 phase of mitosis. Bcl-2 is a protein that regulates and prevents abnormal apoptotic cell death. This regulatory protein also promotes cellular replication by reducing the requirement for growth factors [36,38-40].
Liang et al. compared expression of progesterone (PR), p16, p53 and pHH3 between benign, atypical, and malignant leiomyoma [40-42]. Use of a higher threshold value for p16 staining improves the significant increase in expression from benign to leiomyosarcoma with similar findings as seen in Atkins et al. and Gannon et al. PR expression was found to be in 82- 100% leiomyomas, 75-90% in leiomyoma variants, and <25% of leiomyosarcoma [39,40]. This delineates no difference in PR expression between leiomyomas and leiomyoma variants, but significant difference when comparing leiomyoma variants such as STUMP and leiomyosarcoma. In several studies, p53 had variable expression profiles when comparing leiomyosarcoma to leiomyoma variants. Zhang et al. examined PCR expression of p53 mutations and found 24% (9/38) cases of leiomyosarcoma and 12% (5/42) of atypical leiomyoma [42]. Liang et al. and Veras et al. showed that >5 pHH3 positive cells/10 HPF were found to be expressed in about 40% of leiomyosarcoma and <10% atypical leiomyoma [38,42,43]. Bcl-2 has been investigated previously and has been found to be expressed more frequently in leiomyomas as compared to STUMP or leiomyosarcoma. If Bcl- 2 is expressed in STUMP or malignant tumors, it is indicative of a good prognostic factor. After long term follow up from diagnosis, 2 STUMP tumors had known recurrence. These tumors were immunoreactive for the CKD2A inhibitor, p16 and p53 tumor suppressors supporting evidence that subtypes of tumors have a greater propensity to recur [39-43].
Evaluation of Caveolin-1 (Cav-1) and AT-rich interactive domain 1 alpha (ARID-1A) expression in uterine smooth muscle tissue was done by Ayaz et al. Cav-1 and ARID-1A are known as signal regulators and tumor suppressors and were used in the differential diagnosis of uterine Smooth Muscle Tumors (SMTs) [44]. The tissue concentration was evaluated between benign leiomyoma, STUMP, and leiomyosarcoma (where each tumor subgroup had 10 patients). Results of the study relieved that as the tumor becomes malignant, expression of perivascular Cav-1 increases significantly between groups. Nuclear staining for ARID- 1A in leiomyosarcomas was shown to be significantly higher than in STUMP benign leiomyoma, making it another potential marker of malignancy [44].
Treatment and Post-treatment Follow Up
There are no available guidelines regarding treatment and follow up for patients diagnosed with STUMP. STUMP is typically diagnosed after tissue sampling from hysteroscopy D&C or following myomectomy or hysterectomy specimen with a patient with suspected fibroids. For women who have been diagnosed with STUMP following myomectomy, a detailed discussion should be held with the patient to review the characteristics of the tumor and the patient’s plans for future pregnancy. Management options include hysterectomy if fertility is completed or myomectomy if fertility is still desired with then hysterectomy after child bearing. Annual surveillance with pelvic imaging has been suggested after hysterectomy [3,19,20].
Although STUMP is thought to a low malignant potential, recurrence of these tumors is a reality. Zhang et al. reviewed 127 patients representing leiomyoma on the pathologic spectrum from benign to malignant. It was determined that 3/31 (10%) atypical leiomyomas and 3/14 (21%) of STUMP with clinical follow up had in fact recurred [36]. Ly et al. had similar results in which they discovered 51 atypical leiomyoma of the uterus with 4/34 (12%) were found to have a recurrence [37]. Guntupalli et al. had identified 41 patients with STUMP in a retrospective review at their institution and found that at a mean follow up time of 45 months (1-171 months), 3 patients (7.3%) had a recurrence during the follow up interval. One of the three patients was diagnosed with leiomyosarcoma at time of recurrence, and all 3 patients diagnosed with a recurrence were healthy and disease free after a mean follow up time of 121 months [12]. Deohar et al. had looked at 21 patients diagnosed with STUMP, of these only 11 had adequate follow up, and one patient was noted to have metastatic liver disease 3 years after the primary surgery [38]. Vahedpoor et al. in a case report of STUMP looked at several tumors from one patient including one that was located on the ovary. They concluded after histologic diagnosis of all tumors that it is possible the number of mitosis is more effective in prediction of the tumor behavior and prognosis of patients [45].
Metasteses of STUMP are also a rare, however potential occurrence. Canciani et al. reported an isolated recurrence of a STUMP 24 years after hysterectomy with metastasis to the lungs [46]. In a retrospective review by Miller et al., 10 patients were identified as having benign metastasizing leiomyoma to the lungs. They also included a literature search that identified about 57 other cases of leiomyoma that had metastasized the lungs. The lung has been the most common extra-uterine site for leiomyoma metastasis and if pulmonary symptoms develop or there is an increasing growth interval, surgical intervention is required [46]. Shapiro et al. reported a case of STUMP tumor with metastasis to the humerus, concluding this group of tumors needs to be under close observation [24]. Kropp et al. also diagnosed a uterine STUMP tumor from a primary bone tumor [47,48].
Although there are no National Comprehensive Cancer Network Clinical Practice Guidelines established for patients with STUMP, recommendations can be based off of guidelines for leiomyosarcoma. New evidence of increased mitotic index and chromosome 1p deletions may lead treating physicians to a more aggressive and more intense follow up as these have been shown to have more malignant potential and likely increased recurrence rate [16,42]. Recommendations include the following: if a patient has been diagnosed with STUMP after tissue sample from biopsy or hysteroscopy, the surgeon should perform a hysterectomy on the patient (regardless of vaginal, abdominal, or laparoscopic). Patients with surgically removed STUMP lesions should get a baseline CT of the chest, abdomen, and pelvis is recommended and then routine physical examinations every 6 months for 5 years and then annually thereafter as recurrences often present as pelvic, abdominal or even as pulmonary metastases [44-47]. If the patient had a myomectomy for fertility purposes clinical evaluation with sonogram every 6 months after surgery with yearly MRI and chest x-ray was for the first 5 years is proposed [4,30,37,40]. Once the patient with myomectomy is finished with fertility, recommendation is to have a hysterectomy due to possibility of recurrence [49].
Surgical management of STUMP has been regarded as common, however treatment of STUMP tumors with adjuvant therapy is less clear and less studies have been performed. Some studies have given hormonal suppression in premenopausal patients to prevent disease progression if metastasis was found [46]. Due to the low recurrence rates, there generally is no role for adjuvant hormonal or chemotherapy therapy [1,9,12,23,49,50].
Conclusion
The diagnosis of STUMP carries with it an element of unknown prognosis. Increasing knowledge of molecular genetics with mutations in MED12, Cav-1, ARID-1a and HMGA2 and deletions seen in chromosome 1, immunohistochemistry with findings of PPH3 and hormonal positive extra-uterine tumors, and longer term follow up data will prove to aide in future management and surveillance guidelines. The focus of future research should be on finding biomarkers, histologic findings, or immune-histochemical markers that can guide which tumors will have malignant transformation [44,49,50].
References
- Kalogiannidis I, Stavrakis T, Dagklis T, Petousis S, Nikolaidou C, et al. (2016) A clinicopathological study of atypical leiomyomas: Benign variant leiomyoma or smooth muscle tumor of uncertain malignant potential. OncolLett 11:1425-1428.
- Ng JS, Han A, Chew SH, Low F (2010) A clinicopathologic study of uterine smooth muscle tumors of uncertain malignant potential (STUMP). Ann Acad Med Singapore 39: 625-628.
- Bell SW, Kempson RL, Hendrickson MR (1994) Problematic uterine smooth muscle neoplasms: aclinicopathologic study of 213 cases. Am J SurgPathol 18: 535.
- Hendrickson MR, Tavassoli FA, Kempson RL, McCluggage WG, Haller U, et al. (2003) Mesenchymal tumours and related lesions In: Worldhealth organization of tumours. Pathology and Genetics of Tumours of Breast and Female Gynetical Organs. Franc: IARC Press.
- Campbell JE, Knudtson JF, Valente PT, Robinson RD, Kost ER (2016) Successful pregnancy following myomectomy for uterine smooth muscle tumor of uncertain malignant potential: a case report and review of the literature. GynecOnc Report 15: 1-3.
- Tabrizi AD, Ghojazadeh M, Anvar HT, Vahedi A, Naji S, et al. (2015) Immunohistochemical prolife of uterine leiomyosarcoma with bizarre nuclei; comparison with conven3onal leiomyoma, smooth muscle tumors of uncertain malignant potental and leiomyosarcoma. Adv Pharm Bull 5: 683-687.
- Dall’Asta A, Gizzo S, Musaro A, Quaranta M, Noventa M, et al. (2014) Uterine smoother muscle tumors of uncertainmalignant poten3al (STUMP): pathology, follow-up and recurrence. Int J Clin Exp Pathol 7: 8136-8142.
- Bulun SE (2013) Uterinefibroids. N Engl J Med 369: 1344-1355.
- Peters WA, Howard DR, Andersen WA, Figge DC (1994) Uterine smooth muscle tumors of uncertain malignant potential. ObstetGynecol 83: 1015-1020.
- Zivanovic O, Jacks LM, Iasonos A, Leitao MM, Soslow RA, et al. (2012) A nomogram to predict postresection 5-year overall survival for patients with uterine leiomyosarcoma. Cancer 118: 660-669.
- Christacos NC, Quade BJ, Dal Cin P, Morton CC (2006) Uterineleiomyomata with deletions of Ip represent a distinct cytogenetic subgroup associated with unusual histologic features. Genes Chromosomes Cancer 45: 304.
- Guntupalli SR, Ramirez PT, Anderson ML, Milam MR, Bodurka DC,et al. (2009) Uterine smooth muscle tumor of uncertain malignant potential: a retrospective analysis. GynecolOncol 113: 324-326.
- Quade BJ, Robboy SJ (2009) Uterine smooth muscle tumors. In:Robboy SJ, Mutter GL, Prat J, et al. (2ndeds.)Robboy's Pathology of the Female Reproductive Tract. Churchill Livingstone Elsevier, Oxfordp: 474.
- Dhingra S, Rodriguez ME, Shen Q, Duan X, Stanton ML, et al. (2011) Constitutive activation with overexpression of the mTORC2 phospholipse D1 pathway in uterine leiomyosarcoma and STUMP: morphoproteomic analysis with therapeutic implications. Int J Clin Exp Pathol 4: 134-146.
- Mehine M, Kaasinen E, Heinonen HR, Makinen N, Kampjarvi K,et al. (2015) Characterization of uterine leiomyomas by whole-genome sequencing. PANS 113: 1315-1320.
- Hodge JC, Pearce KE, Clayton AC, Taran FA, Stewart EA (2014) Uterine cellular leiomyomata with chromosome 1p deletions represent a distinct entity. Am J ObstetGynecol210: 572
- Mehine M, Kaasinen E, Heinonen HR, Mäkinen N, Kämpjärvi K,et al. (2016) Integrated data analysis reveals uterine leiomyoma subtypes with distinct driver pathways and biomarkers. ProcNatlAcadSci U S A 113: 1315-1320.
- Schwetye KE, Pfeifer JD, Duncavage EJ (2014) MED12 exon 2 mutations in uterine and extrauterine smooth muscle tumors. Hum Pathol 45: 65-70.
- Kempson RL, Hendrickson MR (2000) Smooth muscle, endometrial stromal, and mixed mullerian tumors of the uterus. Mod Pathol 13: 328-342.
- Ip PP, Tse KY, Tam KF (2010) Uterine smooth muscle tumors other than the ordinary leiomyomas and leiomyosarcomas: a review of selected variants with emphasis on recent advances and unusual morphology that may cause concern for malignancy. Adv Anat Pathol 17: 91.
- Oliva E (2016) Practical issues in uterine pathology from banal to bewildering: the remarkable spectrum of smooth muscle neoplasia. Mod Pathol 29: 104-120.
- Manuja K, Kadam SR, Chandrasekhar HR (2011) Variants of leiomyoma: histomorphological study of tumors of myometrium. J South Asian Fed ObstetGynaecol 3: 89-92.
- Kerliu-Saliu I, Sahatciu-Meka V, Kerliu L, Shahini L (2016) Atypicaluterine leiomyoma: a case report and review of the literature. J Med Case Report 10: 22-26.
- Shapiro A, Ferencyzt A, Turcotte R, Bruchim I, Gotlieb WH (2004) Uterine smooth muscle tumor of uncertain malignant potential metastasizing to the humerus as a high grade leiomyosarcoma. GynecolOncol 94: 818-820.
- Taran FA, Weaver AL, Gostout BS, Stewart EA (2010) Understanding cellular leiomyomas: a case-control study. Am J ObstetGynecol 203: 109.
- Wen KC, Horng HC, Wang PH, Chen YJ, Ten MS, et al. (2016) Uterine sarcoma part I uterine leiomyosarcoma: The Topic Advisory Group systematic review. Taiwan K ObstsGynecol 55: 463-471.
- Toledo G,Oliva E (2008) Smooth muscle tumors of the uterus. Arch Pathol Lab Med 132: 594-605.
- Stănescu AD, Nistor E, Sajin M, Stepan AE (2014) Immunohistochemical analysis in the diagnosis of uterine myometrial smooth muscle tumors. Rom J MorpholEmbryol55: 1129-1136.
- Sato K, Yuasa N, Fujita M, Fukishima Y (2014) Clinical application of diffusion weighted imaging for preoperative differentiation between uterine leiomyoma and leiomyosarocoma. Am J ObstetGynecol 210: 368.
- Van den Bosch T, Dueholm M, Leone F, Valentin L, Rasmussen CK, et al. (2015) Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: a consensus opinion from the morphological uterus sonographic assessment (MUSA) group. Ultrasound ObstetGynecol 46: 284-298.
- Arleo EK, Schwartz PE, Hui P, McCarthy S (2015) Review of Leiomyoma Variants. Am J Radiol 205:912-923.
- Sahdev A,Sohaib SA, Jacobs I,Sheperd JH, Oram DH, et al. (2001) MR imaging of uterine sarcomas. AJR 1777: 1307-1311.
- Goto A, Takeuchi S, Sugimura K, Maruo T (2002) Usefulness of Gd-DTPA contrast-enhanced dynamic MRI and serum determination fo LDH and its isozymes in the differential diagnosis of leiomuosarcoma from degenerated leiomyoma of the uterus. Int J GynecolCnacer 12: 354-361.
- O'Connor DM, Norris HJ (1990) Mitotically active leiomyomas of the uterus. Hum Pathol 21: 223-227.
- Perrone T, Dehner LP (1988) Prognostically favorable "mitotically active" smooth-muscle tumors of the uterus. A clinicopathologic study of ten cases. Am J SurgPathol 12: 1-8.
- Zhang Q, Ubago J, Li L (2014) Molecular analyses of 6 different types of uterine smooth muscle tumors: emphasis in atypical leiomyoma. Cancer 120: 3165-3177.
- Ly A, Mills AM, McKenney JK (2013) Atypical leiomyomas of the uterus: a clinicopathologic study of 51 cases. Am J SurgPathol 37: 643-649.
- Deodhar KK, Goyal P, Rekhi B, Menon S, Maheshwari A, et al. (2011) Uterine smooth muscle tumors of uncertain malignant potential and atypical leiomyoma: A morphological study of these grey zones with clinical correlation. Indian J PatholMicrobiol 54: 706-711.
- Atkins KA, Arronte N, Darus CJ, Rice LW (2008) The Use of p16 in enhancing the histologic classification of uterine smooth muscle tumors. Am J SurgPathol 32: 98-102.
- Gannon BR, Manduch M, Childs TJ (2008) Differential Immunoreactivity of p16 in leiomyosarcomas and leiomyoma variants. Int J GynecolPathol 27: 68-73.
- Abdelkader A, Lam CA, Shahir KS, Christians K, Suster SM (2017) Retroperitoneal lymphangioleiomyoma with lymph node involvement: A pathologic-radiologic correlation of a rare form of myomelanocytic tumor. Ann DiagnPathol 27: 69-73
- Liang Y, Zhang X, Chen X, Lu W (2015) Diagnostic value of progesterone receptor, p16, p53, and pHH3 expression in uterine atypical leiomyoma. Int J Clin Exp Pathol 8: 7196-7202.
- Veras E, Malpica A, Deavers MT, Silva EG (2009) Mitosis-speci c marker phosphohistone H3 in the assessment of mitotic index in uterine smooth muscle tumors: a pilot study. Int J GynecolPathol 28: 316-321.
- Ayaz D, Diniz G, Kahraman DS, Sayhan S, Uncel M,et al. (2016) The evaluation of the caveolin-1 and AT-rich interactive domain 1 alpha expressions in uterine smooth muscle tumors. Indian J PatholMicrobiol 59: 301-304.
- Vahedpoor Z, Khamechian T, Zandi N (2017) Uterine smooth muscle tumors of uncertain malignant potential (STUMP) mistaken with ovarian tumor in a female with polio: a case report. J ObstetGynecol Cancer Res 2: e9425.
- Canciani GN, Burbos N, Duncan TJ, Lonsdale R, Nieto JJ (2012) Late presentation of metastatic smooth muscle neoplasm of the uterus with low malignant potential. J GynecolOncol 23: 69-71.
- Miller J, Shoni M, Siegert C (2016) Benign metastasizing leiomyomas to the lungs: an institutional case series and a review of the recent literature. Ann ThoracSurg 101: 253-258.
- Kropp L, Siegal GP, Framptom GM, Rodriguez MG, McKee S, et al. (2016) Primary intraosseous smooth muscle tumor of uncertain malignant potential: original report and molecular characterization. RareTumors 4: 2036-3613.
- Peeters N, Hulsbosch S, Ballaux F, Baekelandt J (2016) Uterine smooth muscle tumors of uncertain malignant potential: analysis of diagnoses and therapies illustrated by two case reports. Eur J GynaecolOncol 37: 367-373.
- Rommel B, Holzmann C, Bullerdiek J (2016) Malignant mesenchymal tumors of the uterus – time to advocate a genetic classification Expert Rev Anticancer Ther 111: 1155-1166.

