Billy M Tsima1,2*, Deogratias O Mbuka1,2, Maxwell Mungisi2 and Eva Lephirimile2
1Department of Family Medicine, University of Botswana School of Medicine, Gaborone, Botswana
2Letsholathebe II Memorial Hospital, Disaneng Ward, Maun, Botswana
*Corresponding Author:
Billy M Tsima
Department of Family Medicine
University of Botswana School of Medicine
Private Bag 0022, Gaborone, Botswana
Tel: +(267)3555564
Fax: +2673956591
E-mail: billy.tsima@mopipi.ub.bw
Received Date: April 20, 2017; Accepted Date: April 28, 2017; Published Date: May 10, 2017
Citation: Tsima BM, Mbuka DO, Mungisi M, et al. Use of Abbreviations and Acronyms among Healthcare Workers in a Resource Limited Setting. J Healthc Commun. 2017, 2:3. doi: 10.4172/2472-1654.100063
Keywords
Abbreviations; Acronyms; Healthcare; Botswana; Resource limited setting
Introduction
Abbreviations and acronyms (A&A) are commonly used in both general and clinical settings to simplify and facilitate communication. Additionally, abbreviations and acronyms are used as means of saving time, space and effort. Consequently, the communication of information in medical records is done through documentation that includes different A&A. The origin of the use of abbreviations can be traced back to Medieval Latin manuscripts when limitation in writing space necessitated shortening of sentences [1]. As Latin culture influenced medical terminology, the habit of using abbreviations became entrenched in medical culture [1]. Conversely the widespread use of acronyms became prominent in the 20th century when such acronyms as LASER (Light Amplifications by Stimulated Emission of Radiation) and SONAR (Sound Navigation And Ranging) became popular [2].
Although it has become common practice to use abbreviations and acronyms in medical records, their overuse has been highlighted as a concern for patient safety. Certain abbreviations have been noted to cause an increase in misinterpretations and consequently medication errors [3]. The Institute for Safe Medication Practices estimates that over 7,000 deaths per year may be attributed to medication error, with abbreviations contributing significantly to the high number [2,4]. Although abbreviations and acronyms exist to facilitate communication, ironically, lapses in communication often occur due to their use. Evidently, communication failures are the leading causes of inadvertent patient harm [5]. A recent audit in a paediatric unit in the United Kingdom revealed that as few as 56% paediatric doctors and 31% ancillary staff in the same unit consistently identified abbreviations used in their hand-over notes [6]. Another study suggested that there was a degree of misunderstanding between ophthalmologists and general practitioners regarding some of the acronyms used in their letters and discharge summaries [7]. An Australian study showed a high prevalence of error-prone abbreviations used in prescribing practices across a multiple-hospital network in that country [8].
Some abbreviations are ambiguous and thereby result in loss of clarity or precision of the message intended by the author. This has been demonstrated in a chart review survey in Oman that showed a significant use of ambiguous abbreviations in routine medical care [9]. The ambiguity of acronyms has been reported outside clinical practice. Cheng reported a high degree of ambiguity with a record of 16 separate acronyms for cardiology clinical trials using the same acronym [10]. Medical ethicists have raised concerns regarding the use of acronyms to describe clinical trials arguing that particularly positive sounding acronyms (e.g. HOPE, CURE etc.) may lead to research subjects overestimating the potential benefit of a research study and underestimating its potential harm [11].
Recent evaluation of nursing documentation in Nigeria indicated that most nurses disagreed or were undecided with the use of abbreviations and symbols in patients’ records [12]. A review of maternal mortality cases in Botswana for the year 2010 showed that in 30% of the recorded cases, there was evidence of poor communication between doctors and nurses [13]. However, the contribution of the misunderstanding or misinterpretation of A&A to the poor communication or patient outcomes as a result was not specified in that record review. The prevalence of abbreviation usage and the extent to which abbreviation use contributes to poor communication in district hospitals in resource limited settings remain unknown thus underscoring the need to bridge the knowledge gap.
District hospitals operate with a heterogeneous community of healthcare workers making up the multidisciplinary team in charge of patient care. These different medical cadres are expected to share important information centred on patient care. The information is captured within patients’ records and is used to communicate matters of patient care among the members of the multidisciplinary team. The use of A&A in this setting assumes that all have common understanding regarding the A&A authored by any member of the multidisciplinary team involved in the care of patients. However, the level of understanding of the meaning of abbreviations by healthcare workers in district hospitals in resource limited settings is rarely reported in the literature. We therefore aimed to assess the frequency, nature and healthcare workers’ understanding of the meaning of the abbreviations and acronyms used in medical records at a district hospital in a resource limited setting.
Methods
This was a cross-sectional study using inpatient medical charts. The charts of recently discharged patients were assessed for abbreviations and acronyms used during the period of admission. All abbreviations were transcribed into a data collection form. The data collected included the abbreviations used, their frequency of use and the context in which the abbreviation was used. Letsholathebe II Memorial Hospital (LIIMH) is a 300-bed district hospital with over 280 healthcare workers involved in clinical care. The data were collected from all units with inpatient service.
A research assistant prospectively collected the data on a two-day interval schedule for one month. A list of all abbreviations used during the data collection period was compiled. A list of the different abbreviations and acronyms was prepared and presented in the form of an anonymously completed, self-administered questionnaire to consenting, randomly selected healthcare workers at LIIMH. The questionnaire assessed each participant’s understanding of the meaning of the abbreviations listed as well as soliciting alternative interpretation of the listed abbreviations in the questionnaire. Participants were asked to leave a blank response and were discouraged to guess the meaning of abbreviations that they were not sure of. Completed questionnaires were marked against a compiled list of meaning of the abbreviations. The abbreviations were checked against the online version of the Merrian-Webster medical dictionary (https://www.merrian-webster.com) where applicable. We considered understanding as knowledge or realization of the meaning of the abbreviation presented. For instance, the abbreviation BD which is Latin in origin (bis die) was considered to be correctly understood if the participant recorded any of the following explanations; “bis die”, “twice a day”, “two times a day”, “twice daily” or “two times daily”. We also collected data on participants’ age, gender, professional designation, duration of posting and ward of duty.
Ethics
The study received ethical approval from the University of Botswana’s Ethics Review Board, the Botswana Ministry of Health’s Research Unit and from the Ethics Review Committee at LIIMH.
Statistics
Data were analysed descriptively as frequencies, means (or medians) and percentages. Data is herein described as number of subjects (percentages) for categorical variables and mean (plus Standard Deviation) for continuous variables. Where continuous variables do not follow a normal distribution, testing using the Shapiro-Wilks test for skewness was done; the median (interquartile range) is reported. Chi-square test (Fisher’s exact test) is reported for differences in distribution of the population with n categories. The Kruskal-Wallis test was used for hypothesis testing of non-parametric data when comparing more than two groups.
Results
A total of 57 inpatient charts were included in the study during the one month period. The total count of abbreviations, acronyms and symbols was 1693. This represented 86 different abbreviations, acronyms and symbols. Seventy-four healthcare workers at the LIIMH participated in the study by completing the questionnaires. Most of these were female (61%) and were from the nursing cadre (60%). The median (IQR) age of the participants was 32.5 (29,43) years. The distribution of the participants’ characteristics is presented in Table 1.
| Characteristic |
| Cadre |
n (%) |
| Doctors |
18 (24) |
| Nurses |
44 (60) |
| Allied healthcare workers |
12 (16) |
| Male gender; n (%) |
29 (39) |
| Duration at current posting; |
n (%) |
| Less than one month |
8 (11) |
| Less than one year |
15 (20) |
| Less than two years |
6 (8) |
| More than two years |
36 (49) |
| Not documented |
9 (12) |
| Age in years; Median (IQR) |
32.5 (29,43) |
Table 1: Distribution of study participants’ characteristics.
Over half (52.7%) of all the abbreviations came from doctors’ notes while nurses’ notes contributed over a third (34.6%) of abbreviations. Admission notes, laboratory forms, temperature charts and X-ray forms all contributed to less than one percent of all abbreviations used. The discharge notes, dietitians’ notes and drug sheets contributed 2.3%, 1% and 7.6% respectively. The source of abbreviations is listed in Table 2.
| Context |
N (%) |
| Admission form |
1 (0.1) |
| Consent form |
21 (1.2) |
| Dietitians notes |
17 (1) |
| Discharge summary |
39 (2.3) |
| Doctors notes |
892 (52.7) |
| Drug sheet |
128 (7.6) |
| Laboratory form |
2 (0.1) |
| Nurses notes |
586 (34.6) |
| Temperature chart |
5 (0.3) |
| X-ray form |
2 (0.1) |
| Total |
1,693(100) |
Table 2: Source of abbreviations.
The total score of correctly identified abbreviations was significantly different among the three cadres of healthcare workers (P=0.001) as shown in Figure 1. Allied healthcare workers exhibited the least score compared to the other groups while nurses had the highest score. However, when the analysis was restricted to doctors and nurses, the two groups had comparable scores (75% versus 76% respectively; p=0.6). Overall, the healthcare workers correctly identified 73% of the abbreviations presented to them. In fifty of the collated abbreviations (58.1%), participants suggested alternative meaning of the abbreviation.
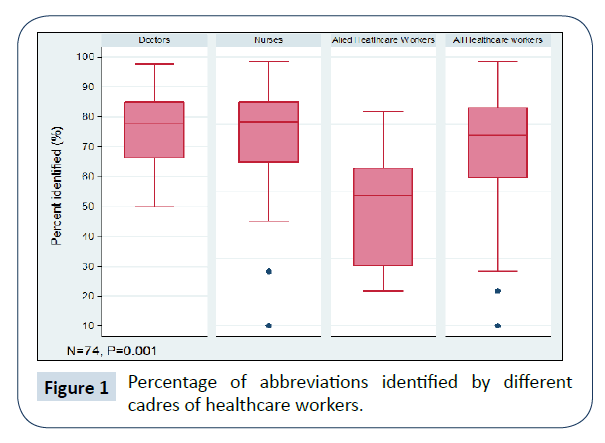
Figure 1: Percentage of abbreviations identified by different cadres of healthcare workers.
Discussion
Our findings indicate a high frequency of abbreviations usage in medical records at a district hospital in a resource limited setting, with 86 different abbreviations revealed in our study. Furthermore, our study showed that healthcare workers could only identify 73% of the abbreviations used in their settings. These results are similar to findings by Sheppard et al. in the United Kingdom which showed that healthcare workers involved in patient care in their paediatric unit recognized up to 63% of abbreviations [6]. In West Africa, a prospective study carried out in Ghana, Sierra Leone and Nigeria documented sixty-five unconventional abbreviations used by clinicians on radiological request forms. This was noted to be of clinical importance and raised concerns that such practice may result in incomplete or inappropriate investigations being carried out [9]. The wrong investigation is likely to have negative cost implication as there may be need to subsequently perform another investigation if the initial one does not yield relevant information. Furthermore, where such investigations involve radiation, the patient will be exposed to extra radiation as the need to rectify an inappropriately performed investigation arise. Inappropriate and incomplete investigations may be prevented or reduced by use of conventional abbreviations for which common understanding between clinicians exist. Although we did not stratify the abbreviations seen in our study into conventional and unconventional ones, the 73% performance level of healthcare workers in identifying the abbreviations may be in keeping with the fact that many unconventional abbreviations were used. Thus, the use of unconventional abbreviations may have contributed to failure of some participants to identify abbreviations in the questionnaire.
A high proportion (58.1%) of the abbreviations had alternative meaning reported by the participants. Our finding is comparable to findings by Kim et al. whose study recorded a 54.3% proportion of ambiguous abbreviations in clinical notes [14]. The ambiguity arising from multiple interpretations of abbreviations is potentially detrimental to patient care [15]. Several approaches to disambiguation of abbreviations and acronyms in clinical notes have been proposed in the biomedical literature. One approach is the use of electronic medical records guided by natural language processing computer applications [16]. The proximity of the abbreviation with its expanded form such as “ABBREVIATION (Expanded form)” is used to resolve the ambiguity [17]. Although this has good performance with biomedical text, it has poor performance when used with clinical notes [17]. To be effective, clinical natural language processing requires a comprehensive lexical database containing all clinical abbreviations and their possible senses. However, the compilation of such a database has eluded researchers due to the highly dynamic nature of abbreviation generation. Additionally, clinicians often create their own abbreviations that vary by context [18]. Moreover, the use of electronic medical records is often not feasible in resource limited settings. Although less than ideal, the implementation of a “Do Not Use” list of abbreviations is a possible solution to curb inappropriate use of abbreviations in clinical notes. Such a list could be informed by results of regular audits of medical charts ensuring that ambiguous abbreviations are excluded from the published list of standard abbreviations.
Doctors contributed the highest proportion (24%) as authors of abbreviations when compared with other healthcare workers. This is comparable to results from a study examining physician-entered inpatient admission notes at a New York hospital which revealed that abbreviations represented up to 17.1% of total words used in the notes [19]. There is very little qualitative data from the literature exploring the popularity of abbreviation use among doctors and therefore the reasons for this remain unknown. It is possible that doctors’ affinity for abbreviations stems from the need for speed in writing notes during limited time at patient encounters. Furthermore, doctors’ handwriting is notoriously illegible and therefore abbreviations may be preferred by those concerned about the legibility of their handwriting as abbreviations offer better readability as they are conventionally written in capital letters.
The nursing cadre outperformed the other cadres of healthcare workers in identifying the abbreviations presented in the questionnaire. It appears that even though nurses did not contribute the highest proportion of abbreviations, they performed better at correctly identifying the abbreviations than the other groups. We hypothesize that the reason for this is the fact that nurses regularly consult doctors’ notes and those of other members of the multidisciplinary team to get orders for patient care. Therefore, nurses become more familiar with the different abbreviations authored by different healthcare workers than do the other healthcare workers. Additionally, compared to the other healthcare workers in our setting, the nursing cadre is less heterogeneous in terms of training and practice background with an estimated 84% of nurses being from Botswana in contrast to only 21% of doctors in the country [20].
Our study is not without limitations. The study was conducted at a single district hospital and therefore limiting the generalization of our findings to other district hospitals. However, district hospitals in Botswana are generally comparable and healthcare workers often rotate among these. With only 57 files assessed, it is likely that our study missed other abbreviations used at LIIMH thus raising concerns regarding the completeness of the list. However, a review of the list showed no new abbreviations following the assessment of the first 20 files. Additionally, our sample had fewer allied healthcare workers than doctors and nurses thus limiting robust subgroup analyses. Furthermore, the cross-sectional design of our study precludes making inferences about causality. Future studies should include other district hospitals and expand the sample size.
Conclusions
There is evidence that abbreviations are frequently used in medical notes at a district hospital in a resource limited setting. A similar assessment likely exists in district hospitals in comparable settings. There is need to standardize abbreviations and acronyms used in clinical care to minimize the potential danger of compromised patient safety.
Acknowledgements
We are grateful to all the healthcare workers at Letsholathebe II Memorial hospital who participated in this study as well as Veronica O. Makopo for assisting with data collection.
References
- Bloom D (2000) Acronyms, abbreviations and initialisms. Br J Urol 86: 1-6.
- Kuhn IF (2007) Abbreviations and acronyms in healthcare: when shorter isn’t sweeter. Ped Nurs 33: 392-398.
- Koczmara C, Jelincic V, Dueck C (2005) Dangerous abbreviations: “U” can make a difference! CACCN 16: 11-15.
- https://www.ismp.org/pressroom/PR20051108.pdf.
- Leonard M, Graham S, Bonacum D (2004) The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care 13: i85-i90.
- Sheppard JE, Weidner LC, Zakai S, Fountain-Polley S, Williams J (2008) Ambiguous abbreviations: an audit of abbreviations in paediatric note keeping. Arch Dis Child 93: 204-206.
- Akunjee M, Ali N, Ahfat F (2007) The use of abbreviations in ophthalmologic correspondence with general practitioners. Qual Prim Care 15: 145-150.
- Doodley MJ, Wiseman M, Gu G (2012) Prevalence of error-prone abbreviations used in medication prescribing for hospitalised patients: multi-hospital evaluation. Inter Med J 42: e19-e22.
- Jumah KB, Gordon-Harris, Agahowa (1995) Common faults in filling of radiological request forms. East Afr Med J 72: 744-745.
- Cheng T (1999) Acronyms in clinical trials in cardiology-1998. Am Heart J 137: 726-765.
- Isles AF, Pearn JH (2014) Acronyms confuse everyone: combating the use of acronyms to describe paediatric research studies. J Paediatr Child Health 50: 756-758.
- Ofi B, Sowunmi O (2012) Nursing documentation: experience of the use of the nursing process model in selected hospitals in Ibadan, Oyo State, Nigeria. Int J Nurs Pract 18: 354-362.
- Ray S, Madzimbamuto FD, Ramogola-Masire D, Philips R, Mogobe KD, et al. (2013) Review of causes of maternal deaths in Botswana in 2010. S Afr Med J 103: 537-542.
- Kim Y, Hurdle JF, Meystre SM (2010) Acronyms and abbreviations ambiguity in clinical notes. AMIA Annu Symp Proc.
- Walsh KE, Gurwitz JH (2008) Medical abbreviations: writing little and communicating less. Arch Dis Child 93: 816-817.
- Pakhomov S, Pedersen T, Chute CG (2005) Abbreviation and acronym disambiguation in clinical discourse. AMIA Annu Symp Proc 2005: 589-593.
- Moon S, Pakhomov S, Melton GB (2012) Automated disambiguation of acronyms and abbreviations in clinical texts: window and training size considerations. AMIA Annu Symp Proc 2012: 1310-1319.
- Wu Y, Denny JC, Rosenbloom ST, Miller RA, Giuse DA, et al. (2011) A comparative study of current clinical natural language processing systems on handling abbreviations in discharge summaries. AMIA Annu Symp Proc 2011: 1541-1549.
- Xu H, Stetson PD, Friedman C (2007) A study of abbreviations in clinical notes. AMIA Annu Symp Proc pp: 821–825.
- Nkomazana O, Peersman W, Willcox M, Mash R, Phaladze N (2014) Human resources for health in Botswana: The results of in-country database and reports analysis. Afr J Prm Health Care Fam Med 6: E1-E8.

