Veena A Patil and Jignesh R Patel*
Department of Periodontics, HKE Society’s SN Institute of Dental Sciences and Research, Karnataka, India
*Corresponding Author:
Jignesh R Patel
Department of Periodontics, HKE Society’s SN Institute of Dental Sciences and Research, Kalaburagi, Karnataka, India
Tel: +919480285089
E-mail: veenaashokpatil@yahoo.com
Received Date: February 28, 2017; Accepted Date: March 09, 2017; Published Date: March 14, 2017
Citation: Patil VA, Patel JR. Treatment of AlteredPassive Eruption Related Gummy Smile. Periodon Prosthodon 2017, 3:1.doi: 10.21767/2471-3082.100027
Copyright: ©2017 Patil VA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: This report describes the management of a case with gummy smile by esthetic crown lengthening, along with gingival depigmentation using 980 nm diode laser.
Methods: A 23 year old male patient reported with the demand for cosmetic correction of “gummy smile”. Various causes for excessive gingival display were ruled out and diagnosed to be altered passive eruption. Following Phase-I therapy, 980 nm diode laser was used to achieve the desired results.
Results: The 1 to 6 months follow up showed excellent color and contour of gingiva. Healing was uneventful on evaluation.
Conclusion: Correcting gummy smile with esthetic mucoginigval procedure, along with depigmentation gives esthetic as well as cosmetic benefits. Diode laser was used as it is known to be an excellent tool as compared with other conventional surgical procedures in terms of patient and operator comfort.
Keywords
Gummy smile; Mucoginigval surgery; Laser; Gingival depigmentation
Background
A pleasant smile is considered a symbol of beauty and desired by every individual in the modern society. Major Factors influencing the smile are: the teeth, the gingiva and the lip. All the components in an esthetic harmony create a pleasant smile [1,2]. The excessive gingival display during smiling is a frequent condition impairing smile esthetics. Excessive gingival tissue, frequently called Gummy Smile, can be associated to vertical maxillary growth, dentoalveolar extrusion, short upper lip, upper lip hyperactivity, Altered Passive Eruption (APE) or a combination of these factors [3]. APE of teeth mostly due to developmental or genetic factors that may lead to the persistence of excessive soft tissue amount over the enamel surface because the epithelial junction do not shifts apically to the cementoenamel junction (CEJ) level physiologically. The prevalence of APE is reported to be approximately 12% considering more than 1,000 adult patients with mean age of 24 years [4]. This case report demonstrate management of APE by gingivectomy method combined with gingival depigmentation procedure using commonly available diode laser and followed up for short term period.
Methodology
A 23-year old male patient was referred to the department of Periodontics, HKES’s S.N. Institute of Dental Sciences and Research with the chief complaint of excessive gingival display since 3 years. On examination, teeth 13-23 [FDI notation] demonstrated excessive gingival display which he was finding unaesthetic when he smiled naturally (Figure 1).
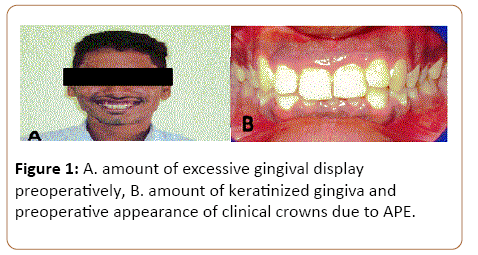
Figure 1: A. amount of excessive gingival display preoperatively, B. amount of keratinized gingiva and preoperative appearance of clinical crowns due to APE.
The gingival tissue was firm on palpation and wide band of keratinized gingiva was present. Radiograph was also advised to see the relation between CEJ and alveolar bone crest (ABC). It was found that distance between the CEJ and ABC was more than 1.5 mm. Based on the clinical findings and after ruling out other causes of gummy smile, the case was diagnosed as excessive gingival display due to type-1 altered passive eruption. Altered passive eruption is the condition in which the gingival unit fails to migrate physiologically apical to CEJ. To correct excessive gingival display esthetic crown lengthening procedure by gingivectomy was planned along with gingival depigmentation. Treatment plan was elaborated to the patient, and a written informed consent was acquired. The surgical procedure is as follows: local infiltration of local anesthesia was administered; depth of the sulcus was marked with pocket marker. An incision was given with direct contact using 980 nm diode laser with pulse mode and 2 W power setting. Excessive amount of excised gingiva was removed using surgical curettes and the area was thoroughly irrigated with normal saline. The amount of residual keratinized gingiva and display of gingiva was evaluated intraoperatively. After successful removal of excessive gingiva frenum attachment was located at papillary level and patient was also complaining of dark brown pigmentation of gums, therefore laser frenectomy was done at the same power setting and gingival depigmentation procedure was done in non-contact, 1 W pulse mode power setting to enhance the overall esthetic outcome (Figure 2).
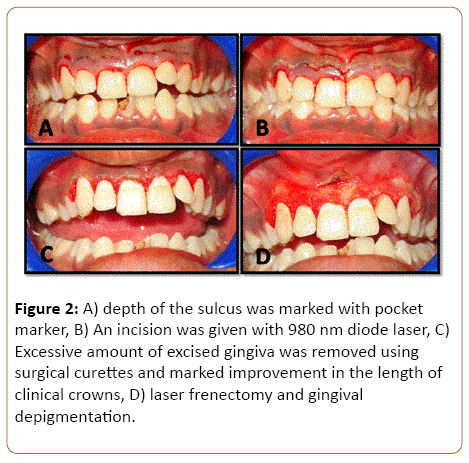
Figure 2: A) depth of the sulcus was marked with pocket marker, B) An incision was given with 980 nm diode laser, C) Excessive amount of excised gingiva was removed using surgical curettes and marked improvement in the length of clinical crowns, D) laser frenectomy and gingival depigmentation.
The area of treatment was covered with periodontal pack (Coe-pak) to reduce the discomfort of the patient while having food and beverages. Patient was prescribed 400 mg ibuprofen twice daily for 10 days as an analgesic. Patient was evaluated after 1 month and 3 months postoperatively.
Results
The healing of the treated area was uneventful after 1 month and there was a significant improvement in the amount of gingival display when it was compared with the postoperative one. Patient was happy with the outcome of the therapy and overall esthetic of the patient improved satisfactorily. Patient was re-evaluated again after 6 months and esthetic results were maintained (Figure 3).

Figure 3: A) follow up after 1 month, B) results are maintained even after 6 months, C) preoperative unaesthetic gummy smile, D) postoperative esthetic improvement
Discussion
An increasing stringent demand for improvement of esthetics is part of the current periodontal practice. Esthetic treatment of a smile line is often a multifaceted scenario where teeth, periodontal tissues, and lip position interact [5]. The average smile exhibits approximately the full length of the maxillary anterior teeth, with an incisal curve of the teeth parallel to the inner curvature of the lower lip [6]. The treatment of APE may represent a challenge for clinician; In this report a well-defined surgical procedure to correct gummy smile was demonstrated with application of laser. In order to plan correctly the position of incision with laser, a preliminary study on radiograph was performed calculating the real clinical crown dimension. Care was taken not to endanger the bone or periosteum because of laser by adequately marking sulcus depth with pocket marker. In this report care was taken to preserve the natural scalloping architecture of the gingiva and relocation of frenum attachment was also taken into consideration by frenectomy procedure. A study on crown lengthening procedure showed that at least 3 mm of coronal regrowth of gingival margin 6 months after surgery is expected when the flap is sutured at the bone crest [7]. Final outcomes of this report showed that the used procedure was effective with no residual gingival recession or regrowth, stable improvement of crown length compared to the baseline and high patient satisfaction. Laser is an advanced tool which has benefit of precise cutting with pain less and blood less surgical area which enhances the patient comfort. Laser depigmentation is also a predictable treatment modality, results of which are comparable to gold standard surgical scrapping done by scalpel [8]. Literature concerning treatment of gummy smile is generally anecdotal and sparse with no data supported by statistical analysis but based on routine clinical and radiographic examinations etiology of the gummy smile can be established and accordingly treatment plan is prepared. This report describes correction of type-1 APE using gingivectomy procedure due to sufficient amount of keratinized gingiva but in type-2 cases or when osseous contouring is required, flap technique can be chosen to correct the relation between bone and gingival margin.
Conclusion
This case report showed that simple esthetic crown lengthening by gingivectomy procedure with gingival depigmentation leads to predictable outcomes in the treatment of altered passive eruption/gummy smile. A careful preoperative planning avoids complications and enhances postsurgical stability of the gingival margin. Laser is a valuable tool in terms of increasing patient and operator comfort and also provides similar results that can be achieved with conventional surgical instruments and techniques.
References
- Miller PD, Allen EP (1996) The development of periodontal plastic surgery. Periodontology 11: 7-17.
- Garber DA, Salama MA (1996) The aesthetic smile: diagnosis and treatment. Periodontology 11: 18-28.
- Levine RA, McGuire M (1997) The diagnosis and treatment of the gummy smile. CompendContinEduc Dent 18: 757-764.
- Volchansky A,Cleaton-Jones PE (1974) Delayed passive eruption. A predisposing factor to Vincent’s infection? Journal of Dental Association of South Africa 29: 291-294.
- Cairo F, Graziani F, Franchi L, Defraia E, Paolo G, et al. (2012) Periodontal Plastic Surgery to Improve Aesthetics in Patients with Altered Passive Eruption/Gummy Smile: A Case Series Study. International Journal of Dentistry1:1-6.
- Tjan AHL, Miller GD (1984) Some esthetic factors in a smile. The Journal of Prosthetic Dentistry 51:24-28.
- Pontoriero R, Carnevale G(2001)Surgical crown lengthening: a 12-month Clinical Wound Healing Study. Journal of Periodontology 72:841-848.
- Hegde R, PadhyeA, Sumanth S, Jain S, Thukral N(2013) Comparison of Surgical Stripping; Erbium-Doped:Yttrium, Aluminum, and Garnet Laser; and Carbon Dioxide Laser Techniques for Gingival Depigmentation: A Clinical and Histologic Study. J Periodontol84:738-748.

