Keywords
Drug abuse; Drug dependence; Drug control policy; Addiction
Introduction
The language of the science of drug addiction is situated in a context of a terminological quagmire. The quest to understand the excessive voluntary consumption of xenobiotic substances has required the assistance of several disciplines of science, such as pharmacology, psychology, sociology, neurology, etc. The contributions of each of these disciplines have been indispensable for gathering and understanding the empirical data driving the science. As such, there has been an effort within these scientific disciplines to organize the lexicon of basic principles or processes common to all scientific endeavors. For over 65 years, there has been a crusade to adopt a common meta-language or symbolic system that could be used universally to discuss, describe, or analyze meaningful data relevant to the human condition. The investigation into drug abuse is a science where entropy reigns supreme. The question, then, must be asked, “Can we have a science of addiction without some universal truths or one common agreed-upon set of terms that we use to communicate between and within disciplines?
In the second session of the Expert Committee on Habit-Forming Drugs of the World Health Organization (WHO) of the United Nations [1,2], the Committee voted on removing the terms “addictive forming” and “habit forming” from all texts related to the WHO. At the time, the committee approved the term “addictive producing” as more appropriate. The committee defined “drug addiction” as:
a state of periodic or chronic intoxication, detrimental to the individual and to society, produced by the repeated consumption of a drug (natural or synthetic). Its characteristics include:
1. An overpowering desire or need (compulsion) to continue taking the drug and to obtain it by any means;
2. A tendency to increase the dose;
3. A psychic (psychological) and sometimes a physical dependence on the effects of the drug.
Accordingly, the Committee renamed itself the “WHO Expert Committee on Addiction-Producing Drugs”. At the time, some of the most prominent and leading medical professionals appointed to the committee were of the opinion that the “functional structure of an addiction-producing drug” was that particular arrangement of atoms within the molecule which is responsible for the addictive properties of the drug. The Committee admitted in the report that the present state of their knowledge could not identify what part of the drug’s structure was responsible for the addictive properties, but there were prototypic structures such as morphine, pethidine, methadone, and cocaine, to name a few. The focus here was turned on the molecule itself – something about the arrangements of atoms in a given molecule gave the compound an addictive property – “it was owned by the molecule".
In the turmoil of the 1960s the Committee further revised their name to the “WHO Expert Committee on Dependence-Producing Drugs”. At its 13th meeting in 1964 [3] it was voted to abandon the terms, “drug addiction” and “habituation” in favor of “drug dependence” and the Committee once again renamed itself the “WHO Expert Committee on Drug Dependence”. In an attempt to form a consensus on the general terminology regarding drug abuse, the 16th meeting of the group [4] defined “dependence” as:
A state, psychic and sometimes also physical, resulting from the interaction between a living organism and a drug, characterized by behavioral and other responses that always include a compulsion to take the drug on a continuous or periodic basis in order to experience its psychic effects, and sometimes to avoid the discomfort of its absence. Tolerance may or may not be present. A person may be dependent on more than one drug.
By its 20th meeting [5], the international drug supply, distribution, and abuse scenes world-wide had changed dramatically, and the focus of intervention started to be directed on aspects of the individual abuser, the environment, social setting, as well as the pharmacology of the drug substance. The Committee reaffirmed the definition of dependence and redirected its main concern to identifying ways of reducing or eliminating the actual or potential harm to health and social functioning resulting in the repeated use of psychoactive drugs. At the 28th meeting, the Committee also noted that:
1. Dependence on psychoactive drugs may also arise where use is not for subjective pleasure or to relieve distress;
2. The distinction between physical and psychic dependence was difficult in the clinical setting. And,
3. This view was no longer consistent with the scientific literature supporting the notion that all drugs effects on the individual are potentially understandable in biological terms (i.e., there was no use for the term “psychic”) [6].
Based on the evolution of understanding the scientific underpinnings of drug dependence the 28th meeting of the Committee also redefined the term “dependence” to be:
A cluster of physiological, behavioral and cognitive phenomena of variable intensity in which the use of a psychoactive drug (or drugs) takes on high priority. The necessary descriptive characteristics are preoccupation with a desire to obtain and take the drug and persistent drug-seeking behavior. Determinants and the problematic consequences of drug dependence may be biological, psychological, or social and usually interact.
Because of the recognized importance of the term physical dependence in pharmacology and its potential to be confused with the term “drug dependence” the Committee adopted the term “withdrawal syndrome” described in terms of its relevant consequences as follows:
After the repeated administration of certain dependence-producing drugs, e.g. opioids, barbiturates and alcohol, abstinence can increase the intensity of drug-seeking behavior because of the need to avoid or relieve withdrawal discomfort and/or produce physiological changes of sufficient severity to require medical treatment.
A dependence-producing drug is one that has the capacity (property) to produce dependency as defined, above. The Expert Committee [7] concluded that:
1. The specific characteristics of dependence will vary dependent on the type of drug involved ;
2. The state of dependence is not necessarily harmful in itself, however
3. It may lead to consumption (self-administration) of the drug at dosage levels that produce deleterious physical or behavioral changes constituting public health and social problems.
The Expert Committee met again in 2003 and simply defined “dependence” as
“A state in which the individual has a need for repeated doses of the drug to feel good or to avoid feeling bad”,and concluded that it is clear that acceptable medical use of the drug, whether or not it results in drug dependence, is not drug abuse. The Committee suggested that drug dependence may be reported as an adverse drug reaction, but not as drug abuse, and further concluded that it is useful to stress that dependence liability alone is not sufficient reason for proposing the international control of a psychoactive drug [8].
At this 28th meeting the Expert Committee on Drug Dependence mandated the scientific examination of drug dependence and the harmful effects drugs as a part of its general definition of “health” under the organizing principles and Constitution of the U.N. Therefore, it was the mandate of the U.N. to its member states to engage in active research on drug dependence that is the guiding doctrine or driving force for the U.S. FDA and the National Institute on Drug Abuse (NIDA) to continue to identify the first principles of drug abuse as they apply to all new molecular entities (NMEs). As a member state of the U.N., the U.S. must play a health advisory role in mitigating the abuse of new drugs. The preemptive control by the governing body is based on the information in the extant literature from other known exemplars of the pharmacopiae that have taxed the worldwide health care systems as a result of treatment costs induced by abuse (overdose) and dependence (drug recidivism).
The demonstration that a NME has the potential to induce physical dependence is neither a necessary nor sufficient condition to initiate schedule control actions as part of the NDA process. The observations of physical and behavioral changes in animals following acute high dose administrations or following the chronic dose administrations in 2-week, 3, 6, or 9 month toxicity studies during the preclinical Investigational New Drug phase of development (IND) provides valuable information to drug control regulators and also have practical importance for labelling and “black box” warnings that have to be addressed in the NDA. Additionally, under current national and international drug control policies, the full characterization of a NMEs propensity or potential to be used outside the scope of normal medical practice still requires assessment of physical dependence.
The potential of a NME to induce physical dependence can be determined by “direct addiction”, substitution, or suppression of symptoms with similar methodologies in both humans and animals [9-12]. The term “direct addiction” is used to describe an experimental methodology of dosing and observations designed to assess dependence potential, and is consistent with the “zeitgeist” and terminology used at the time by the WHO Expert Committees (described above) to refer to the procedural development and validation of the models that were being reported (i.e., 1965 to 1970) [13-15]. At that time, the term “addiction” was not burdened by the excess baggage it has today. We refer to it now, only for historical accuracy. The hallmark of dependence is the expression of the “withdrawal syndrome”. In “dependence liability” studies the test article is typically administered repeatedly over 14 to 30 days. Physical dependence can then be demonstrated by abrupt cessation of drug administration or by administration of a selective antagonist for the appropriate receptor type (e.g., flumazenil for dependence of the benzodiazepine-type, or naloxone for dependence of the opiate-type).
A conference held in Uppsala Sweden in 1996 on the topic of the withdrawal syndrome from chronic exposure to serotoninselective- reuptake-inhibitors (SSRI’s) advocated the use of the term “discontinuation syndrome” [16]. Seven years later, at the 33rd meeting of the Expert Committee on Drug Dependence, the panel acknowledged that in order to avoid confusion over terminology that can affect proper reporting, interpretation and communication of adverse drug reactions related to dependence, an increasing number of researchers had begun using a different term - “discontinuation syndrome” - instead of “withdrawal syndrome”. They also noted that there is no internationally accepted definition of “addiction” and it was not possible to be certain in what way addiction differs from dependence.
This brief history of these events is intended to highlight the proverbial “Gordian knot” that pervades abuse liability research, literature, and associated conferences. The lexicon is always changing, and at times, has been comically referred to as “psychobabel” [17,18]. Figure 1 contains a series of graphs displaying the changes in yearly use of “key words” submitted by authors of journal manuscripts listed in the National Library of Medicine of the National Institutes of Health (PubMed) from 1950 through 2014.
It seems clear from Figure 1 that there is no end of the use of any one term by authors submitting “key words”, regardless of the regulatory influence of the WHO, NIDA, FDA, Drug Enforcement Administrations or scientific organizations targeting addiction and therapy. The efforts to turn the tide, for or against, any one term or phrase in our lexicon describing processes of drug abuse and addiction over the last 65 years seems to have failed.
The actual contributory or functional role that dependence-status and related physiological withdrawal symptoms play in the actual abuse repertoire of those legitimate patients taking medications as prescribed by their physicians remains unanswered. Even more tenuous is defining the relative importance of dependence in the motivation or drive to initiate, maintain, or reinstate drug taking scenarios in the cyclic pattern of continued drug abuse, even in the presence of significant deleterious physiological, psychological, economical, and social status effects on the abuser over decades of abuse. Moreover, even the language used to refer to these phenomena is not fully developed. The international community of scientists has made repeated attempts to establish the metalanguage we should use to conduct our work. For example, chemists have a distinct set of terms or lexicon (isomers, affinity, dimers, and such), as do engineers theirs (enthalpy, entropy, adiabatic process, etc.). Although countless hours, much debate, and a wealth of monetary resources have gone into modifying how we discuss our science, it seems that there is no consistency with regard to the use of such jargon, making it difficult to put forth a cogent argument regarding the status of these phenomena and their role in drug abuse behaviors. This we feel is an unfortunate state of affairs, one which would benefit from a stability and consistency with regard to the use and definition of terms.
The following example helps to clarify the role of these issues in everyday, clinical interactions with patients. In the early 1960s a “normal” prescribed dose of diazepam started at a 2 mg tablet, administered by mouth once, twice or three times a day [19]. That early maximum of 6 mg/day dose pales in comparison to reports in 2015 of “fully functioning” patients being legally prescribed doses of greater than 100 mg/day [20]. As reported by Hollister et al. [21], a patient who had been treated with 30 to 45 mg/day of diazepam for 20 months, which was abruptly discontinued, showed a clear-cut withdrawal reaction [22]. Precipitous weight loss and orthostatic tachycardia accompanied the typical dysphoria of withdrawal, which occurred between the fifth and ninth days after discontinuation of the drug [23]. In other cases, the withdrawal reaction under these circumstances has been markedly protracted, though mild. An even more extreme example of a protracted withdrawal reaction followed withdrawal of phenobarbital after 30 years of chronic use. Almost 7 months of treatment were required to stabilize the patient [24]. Clearly, compliant patients taking diazepam under the care of a physician may be taking doses that exceed any of the initial expectations of drug control regulators that approved the drug for use back in the early 1960s, doses that pose a significant risk for drug withdrawal upon abrupt cessation of drug-taking or removal of drug supply [25].
Four decades have passed since Dr. W Martin [26] questioned the motivational role that “negative feeling states” associated with drug intake or dependence may play in actual human drug use patterns. In 1984, Martin highlighted the importance of understanding that “dependencies” are needs [27]. Accordingly, a general definition of need is a life requirement for an environmental circumstance that is conducive to survival or well-being. A more specific definition refers to the mechanisms whereby congenial and hostile environments are recognized. With that in mind, Martin raises the question as to what degree does the intensity of an alcohol-induced hangover reduce the likelihood of future drinking in college? To what degree does the history of multiple episodes of opiate withdrawal, alcohol withdrawal, or the number of methamphetamine-associated “crashes” really motivate drug abusers from initiating another self-administered dose? Does acute dysphoria or even seizure-induction by drugs really control or inhibit drug intake by human consumers? McClane & Martin [26,28] had previously demonstrated cases of opiate abusers voluntarily taking doses of Demerol® (meperidine) and Darvon® (propoxyphene) that induced convulsions. If “convulsions” do not deter drug use, what will?
A better example may be the more recent incidences of the dysphoria, delusions, seizures, hallucinations, and deaths associated with the voluntary consumption of “bath salts” containing synthetic phenylethylamines (cathinones; e.g. 3,4-Methylenedioxypyrovalerone). These illicit chemicals are typically labeled “not for human consumption” and sometimes marketed as “plant food”, “jewelry cleaner”, or “phone screen cleaner”. The continued use of these chemicals despite such dramatically aversive consequences, highlight the minimal value drug abusers have for their own state of “wellbeing” or “homeostasis” [29]. Additionally, the lack of knowledge regarding the role of motivational or need states in initiating or facilitating drug intake is exemplified by the behavior of ketamine users. It is a wonder to question what motivational drive state or psychological value or need is fulfilled by ketamine abusers taking IV doses of the drug to the point of falling into the “K-hole” – complete disengagement from the environment, using doses exceeding the functional anesthetic dose and that generally minimizes memory processes of the event [30-32].
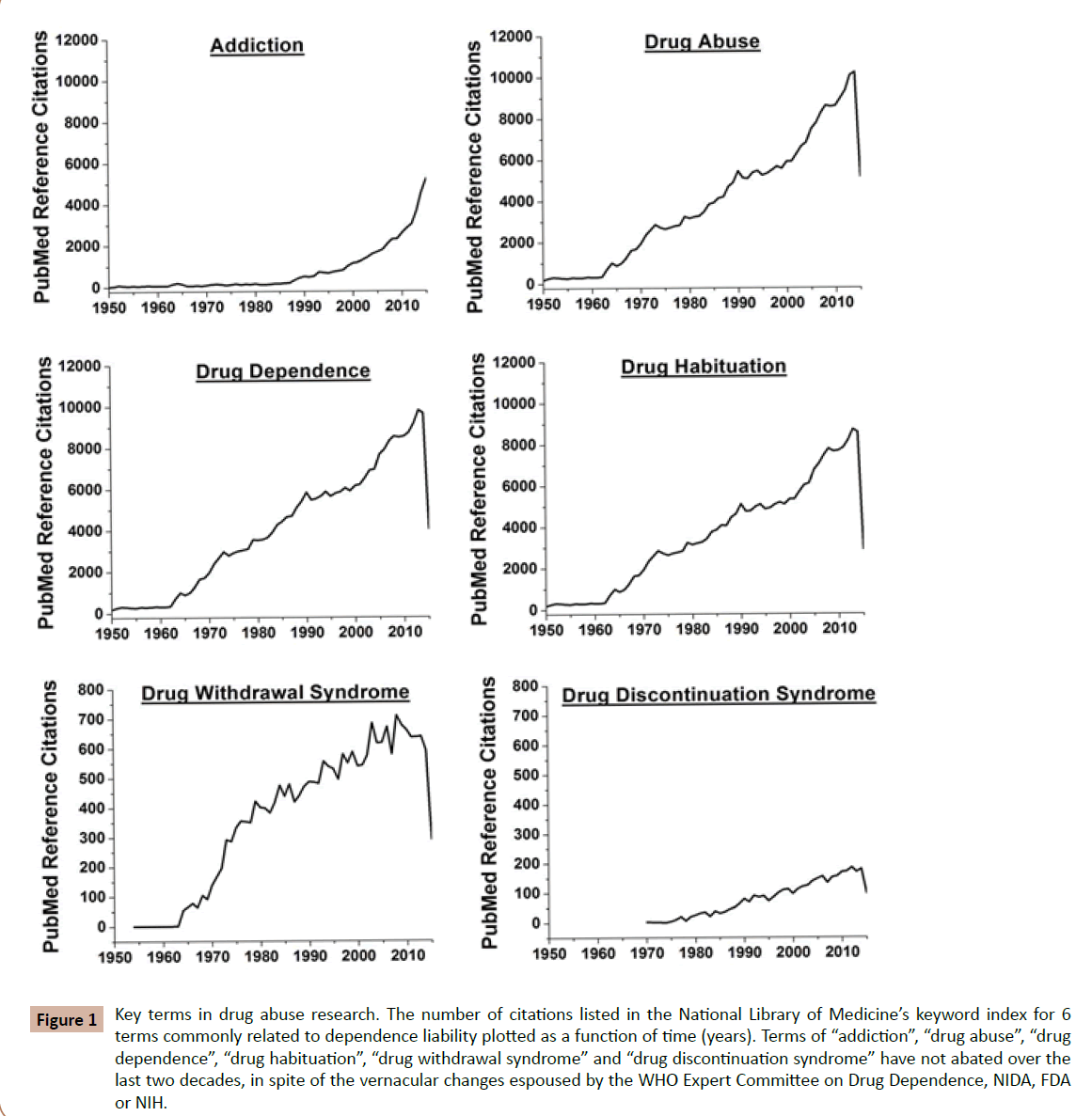
Figure 1: Key terms in drug abuse research. The number of citations listed in the National Library of Medicines keyword index for 6 terms commonly related to dependence liability plotted as a function of time (years). Terms of addiction drug abuse drug dependence drug habituationdrug withdrawal syndrome and drug discontinuation syndrome have not abated over the last two decades, in spite of the vernacular changes espoused by the WHO Expert Committee on Drug Dependence, NIDA, FDA or NIH.
Addiction as a “Disease”
Many times the choice of terms used in an article is based on a subjective feeling, such as a sense of stigmatization implied by the terms. Many attempts of the international community of scientists of the WHO have admonished the use of the ambiguous term addiction in the 1960 to 1970s. Dr. Jerome Jaffe in 1985 [33] wrote,
The term addiction, like the term abuse, has been used in so many ways that it can no longer be employed without further qualification or elaboration. However, since it is not likely that the term will be dropped from the language, it is appropriate to make an effort to delimit its meaning.”
Thirty years later, the NIDA currently accepts and defines addiction as a chronic, relapsing brain disease that is characterized by compulsive drug seeking and use, despite the harmful consequences [34]. It is considered a brain disease because drugs change the brain—they change its structure and how it works. These brain changes can be long-lasting, and can lead to the harmful behaviors seen in people who abuse drugs. The lead health agency on drug abuse in the United States even now considers addiction as a developmental disease [34]. While addiction is not considered a specific diagnosis in the fifth edition of The Diagnostic and Statistical Manual of Mental Disorders (DSM-5)—a diagnostic manual used by clinicians that contains descriptions and symptoms of all mental disorders classified by the American Psychiatric Association (APA), addiction, as used by the NIDA may be regarded as equivalent to a “severe substance use disorder” as defined by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [35].
The first link that resulted from a recent inquiry into a term search for disease on the National Institutes of Health website – the leading U.S. government health agency and the largest biomedical research agency in the world, is a 2004 paper titled, ‘What is disease?’ by Dr. Jackie Leach Scully, now at the Policy Ethics and Life Sciences (PEALS) in the UK. In the article Dr. Scully highlights that although it may not be able to articulate what constitutes a disease per se, most individuals believe they would be able to identify one when presented with given examples. Medical anthropologists and sociologists have shown that personal identification of illness varies with social strata (class), gender, ethnic group, and with history [36]. In 1994, the WHO changed its’ classification of osteoporosis from being an unavoidable part of normal aging to a pathological disease state [37]. The motivating factor for key health care institutions changing addiction [34] and osteoporosis [37] to “disease status” may be its financial drive to have treatment reimbursed by health services providers. The adoption of the disease model of addiction, and in particular classifying the process as a developmental disease, has effects that have both moral and economic consequences. If I have a genetic predisposition with a family history positive background, and reside in a lower income federally-funded housing project where drug sales and use is prevalent, am I already ill? If I have a diagnosis of development disease of addiction and I am asymptomatic, I may not be sick, but an insurance carrier and my employer may consider me to be. If I have the developmental disease of nicotine dependence am I a liability to my employer or do I have to pay for higher health insurance coverage? As Dr. Leach-Scully points out, how do we distinguish properly between real diseases, and human behaviors or characteristics that we just happen to find disturbing? As the pharmaceutical business shows, new clinical diagnoses are often welcomed primarily as opportunities for market growth [38]. With the advancement of PET, MRI, and SPECT imaging are we creating a new disease to fit our new ability to diagnose them [39]. What are the legal, moral, and financial implications if I have the developmental disease of addiction that has its origin from the legally prescribed opiates from my physician? If the proverbial waters are not murky enough, according to NIDA
Thus, it is possible to be dependent on morphine, without being addicted to morphine. (Although, if one is addicted, they are most likely dependent as well.) This is especially true for people being treated chronically with morphine, for example, pain associated with terminal cancer. They may be dependent - if the drug is stopped, they suffer a withdrawal syndrome. But, they are not compulsive users of the morphine, and they are not addicted. Finally, people treated with morphine in the hospital for pain control after surgery are unlikely to become addicted; although they may feel some of the euphoria, the analgesic and sedating effects predominate. There is no compulsive use and the prescribed use is short-lived
In contrast, the statutory or legal definition of addict set forth under the United States Code, Title 21, Chapter 13, [40] means any individual who habitually uses any narcotic drug so as to endanger the public morals, health, safety, or welfare, or who is so far addicted to the use of narcotic drugs as to have lost the power of self-control with reference to his addiction.
Grabbing another “paradox” by the horns, “what differentiates drug abuse, drug use, and drug misuse”? When the chronic pain patient who is in possession of an empty prescription for prn oxycodone ingests a pharmacologically similar opiate product (hydrocodone) that was prescribed for a family member without the knowledge of their physician, is this compulsive use? Drug misuse? Or drug abuse? When does the chronic pain patient move from drug dependency to the developmental disease state of addiction?
This inquiry should not be mistaken to be a general advocacy for a revival of the gospel according to Thomas Szasz [41], but after 65 years of trying to develop a common lexicon, leading scientists, journal editors, and government agencies still remain “on first base”. If we do not have a clear consensus on the subject matter of our science, or an unambiguous set of terms we use to discuss it, we limit ourselves to the way of the alchemists of days long gone. The question now posed to the community of scientists committed to learn, to wonder, even to speculate on the basic principles of human behavior related to repetitive drug consumption is, “How much more time do we need?”
Acknowledgement
All contributors assisted in literature review, consolidation and preparation of the manuscript. Development of all data discussed in this manuscript was funded by MPI Research.
Highlights
1. We review the history of attempts to define and promote a basic language or lexicon to be used to study drug abuse.
2. Regardless of the regulatory or statutory organization that has initiated attempts to organize the lexicon, there has been no clear pattern of change across 65 years of the scientific landscape of drug abuse literature.
3. We conclude that, like the tower of Babel, we may be impeding progress of our science without a common language.
References
- W.H.O. (1949) Expert Committee on Habit-forming Drugs. Report of the First Session. Geneva, World Health Organization, USA.
- W.H.O. (1950) Expert Committee on Drugs Liable to Produce Addiction. Report of the Second Session, World Health Organization, Technical Report Series, No. 21, USA.
- W.H.O. (1964) Expert Committee on Addiction Producing Drugs. Thirteenth Report. World Health Organization, Technical Report Series, No. 273, USA.
- W.H.O. (1969)WHO Expert Committee on Drug Dependence. Sixteenth Report. World Health Organization, Technical Report Series, No. 407, USA.
- W.H.O. (1974) Expert Committee on Drug Dependence, Twentieth Report. World Health Organization, Technical Report Series, No. 551, USA.
- W.H.O. (1993) Expert Committee on Drug Dependence, Twenty-eighth Report. World Health Organization, Technical Report Series, No. 836, USA.
- W.H.O. (2000) Guidelines for the WHO review of dependence-producing psychoactive substances for international control, USA.
- W.H.O. (2003) Expert Committee on Drug Dependence, Thirty-third Report. World Health Organization, Technical Report Series, No. 915, USA.
- Epstein DH, Preston KL, Jasinski DR (2006) Abuse liability, behavioral pharmacology, and physical-dependence potential of opioids in humans and laboratory animals: Lessons from tramadol. Biological Psychology 73: 90-99.
- Howes JF (1981) A simple, reliable method for predicting the physical dependence liability of narcotic analgesics in the rat. Pharmacology Biochemistry and Behavior 14: 689-692.
- Jasinski DR (1977) Assessment of the abuse potentiality of morphine-like drugs (methods used in man). In: Martin WR Drug Addiction I: Morphine, sedative/hypnotic and alcohol dependence. Berlin: Springer-Verlag, Germany.
- Martin WR, Jasinski DR (1977) Assessment of the abuse potential of narcotic analgesics in animals. In: Born G, Eichler O, Farah A, Herken H, Welch A Handbook of Experimental Pharmacology. Berlin: Springer-Verlag, Germany.
- Jasinski DR, Martin WR (1967) Assessment of the dependence-producing properties of dihydrocodeinone and codoxime. Clinical & Pharmacological Therapeutics 8: 266-270.
- Martin WR, Jasinski DR (1969) Physiological parameters of morphine dependence in man–tolerance, early abstinence, protracted abstinence. Journal of Psychiatric Research 7: 9-17.
- Jasinski DR, Martin WR, Hoeldtke R (1971) Studies of the dependence-producing properties of GPA-1657, profadol, and propiram in man. Clinical &Pharmacologica Therapeutics, 12, 613-649.
- Schatzberg, Haddad, Kaplan, Lejoyeux, Rosenbaum (1997) Possible biological mechanisms of the serotonin reuptake inhibitor discontinuation syndrome. Discontinuation Consensus Panel. J Clin Psychiatry 7: 23-27.
- Burton RF, Hinton JW (2010) Up the Tower of Psychobabel: does lexical anarchy impede research into “psychological stress”. Medical Hypotheses 74: 644-648.
- Gutman S, Meyer D (2003) Lexicon for laboratories–scaling the Tower of Babel. Archives of Pathology and Laboratory Medicine127: 625-626.
- Renaud M, Beauchemin B, Lalonde C, Poirier H, Berthiaume S (1980) Practice settings and prescribing profiles: The simulation of tension headaches to general practitioners working in different practice settings in Montreal area. American Journal of Public Health 70: 1068-1073.
- Liebrenz M, Gehring MT, Buadze A,Caflisch C (2015) High-dose benzodiazepine dependence: a qualitative study of patients’ perception on cessation and withdrawal. British Medical Journal–Psychiatry, 15, Epub ahead of print.
- Hollister LE, Motzenbecker FP, Degan RO (1961) Withdrawal reactions from chlordiazepoxide (“Librium”). Psychopharmacologia 20: 63-68.
- Marks J (1978) The Benzodiazepines: Use, Misuse, Abuse. Lancaster, England: MTP Press, Ltd.
- Pevnick JS, Jasinski DR, Haertzen CA (1978) Abrupt withdrawal from therapeutically administered diazepam. Archives of General Psychiatry 35: 995-998.
- Epstein RS (1980) Withdrawal symptoms from chronic use of low-dose barbiturates. American Journal of Psychiatry 137: 107-108.
- American Psychiatric Association (1990) Benzodiazepine dependence, toxicity, and abuse. A task force report of the American Psychiatric Association, Washington DC, USA.
- Martin WR (1977) Predicting abuse liability of depressant drugs. In: T Thompson, T Unna, KR (Eds) Predicting dependence liability of stimulant and depressant drugs. MD: University Park Press, Baltimore.
- Martin WR (1984) Phenomenology and Theoretical Basis of Tolerance and Dependence. In: Sharp, C.W. (Ed.), Mechanisms of Tolerance and Dependence. NIDA Research Monograph 54, NIDA: Rockville.
- McClane TK, Martin WR (1976) Subjective and physiologic effects of morphine, pentobarbital, and meprobamate. Clinical Pharmacology and Therapeutics 20: 192-198.
- National Institute on Drug Abuse (2015a) DrugFacts: Synthetic Cathinones (“Bath Salts”), United States.
- Curran HV, Monaghan L (2001) In and out of the K-hole: a comparison of the acute and residual effects of ketamine in frequent and infrequent ketamine users. Addiction 96: 749-760.
- Meutzelfeldt L, Kamboj SK, Rees H, Taylor J, Morgan CJ, et al. (2008) Journey through the K-hole: phenomeonological aspects of ketamine use. Drug and Alcohol Dependence 95: 219-229.
- Stirling J, McCoy L (2010) Quantifying the psychological effects of ketamine: from euphoria to the K-Hole. Substance Use and Misuse 45: 2428-2443.
- National Institute on Drug Abuse (2015b) The Neurobiology of Drug Addiction: 10: Addiction vs. dependence, United States.
- Jaffe JH (1985) Drug addiction and drug abuse. In: Goodman Gilman A, Goodman LS, Rall TW, Murad F (Edr) Goodman and Gilman’s The Pharmacological Basis of Therapeutics. NY: Macmillan Publishing Co, USA.
- DSM-5 (2013) Diagnostic and Statistical Manual of Mental Disorders. American Psychiatric Association, USA.
- Leach SJ (2004) What is a disease? Disease, Disability and their definitions. European Molecular Biology Organization (EMBO) Reports 5: 650-653.
- W.H.O. (1994) Assessment of fracture risk and its application to screening for postmenaopausal osteoporosis. WHO Technical Report Series 843, WHO Geneva.
- Moynihan R, Heath I, Henry D (2002) Selling sickness: the pharmaceutical industry and disease mongering. British Medical Journal 324:886-891.
- Smith R (2002) In search of ‘non-disease’. British Medical Journal 324:883-885.
- USC: United States Code, Title 21, Food and Drugs, Chapter 13–Drug Abuse Prevention and Control Act, also known as Uniform Controlled Substances Act, (CSA) 1973.
- Szasz T (1974) The myth of mental illness: Foundations of a theory of personal conduct. NY: Harper, USA.

