Keywords
End-of-life care; Futile care; Intensive care unit; Palliative care; Cancer patients; Anxiety and depression; Post-traumatic stress disorder; HADS; IES
Introduction
Almost one out of five Americans die in an intensive care unit (ICU) or shortly after an ICU stay [1]. Despite the growing Palliative Care movement, most admissions of terminal patients still occur in ICUs. The Study to Understand Prognosis and Preferences for Outcomes and Risks of Treatments (SUPPORT) [2] was one of the first studies to systematically investigate symptoms in seriously ill hospitalized patients. Patients at high risk of dying suffer more during ICU: they stay longer under mechanical ventilation, receive more opioids and sedatives, suffer with delirium, anxiety, they are confused, tired, with severe pain and other symptoms [3].
Many reports suggest that clinicians are often inadequately prepared to effectively “diagnose dying” or to discuss the likelihood of imminent death with patients and families [4]. Many guidelines recommend that planning on end of life (EOL) care begin early in the disease course, for patients with incurable cancer [5,6]. Therefore, patients with unlikely benefit whether admitted to the ICU because of high risk of death should be carefully treated in the ward.
Die at home may bring benefits for both patients and family members, regarding improvement of Quality of Life and diminishing the risks for development of post-traumatic stress disorder in relatives [7].
Family members of patients with high risk of death suffer with symptoms of anxiety, depression and post-traumatic stress [8-10]. In addition, the earlier integration of Palliative Care with standard cancer care may improve the survival and the quality of life (QOL), and lessen psychological conditions, ICU length of stay, duration of mechanical ventilation and the use of unbeneficial treatments [11-13]. In this study, our goals were to evaluate the impact of poor prognosis patients admitted to the ICU on their family members’ emotional disorders during ICU and at 3 months follow up.
Methods
This prospective study was conducted in a tertiary private hospital, in an adult medical-surgical 22-bed ICU, in Sao Paulo, Brazil. After 48 h of ICU stay, we approached their family members.
For each patient the following information was recorded: age, gender, marital status, level of education, cause of ICU admission, cancer, SAPS III, Glasgow, SOFA, ICU length of stay (LOS), need for mechanical ventilation, Renal Replacement therapy, delirium (positive CAM-ICU), do not resuscitation (DNR) orders, Palliative Care status and final outcome in the ICU.
The following information was collected about family members: gender, age, marital status, level of education, religion, relationship with the patient and previous ICU experience.
Family members were evaluated at three time points (ICU, and 30- and 90-days after ICU discharge). For the first interview, still in the ICU, family members complete the Hospital Anxiety and Depression Scale (HADS). After ICU discharge, family members were interviewed by phone at 30- and 90-days to complete both the HADS and Impact of Event Scale (IES) and we verify the status of patients’ survival. Both scales HADS and IES were previously validated in Brazil [14,15].
Family members were excluded if they had psychiatric problems or if they refuse to participate. At the moment of ICU admission, clinical condition and oncologic status were analyzed using their medical records. “Poor prognosis patients” were defined as those with incurable disease, Palliative Care status, with “Not Full Treatment”, with DNR orders, according to medical records. They were not necessarily under the care of the Palliative team.
This study was approved by the ethics committee (nº HSL 2010/44).
The Instruments
The HADS score for each subscale (anxiety and depression) ranges from 0-21 and a cut-off score of 10 was used to depict each condition [8]. Scores for the entire scale (emotional distress) range from 0-42, with higher scores indicating more distress. The IES is a tool to detect symptoms indicating a risk of Post-traumatic stress disorder (PTSD). In agreement with previous reports, we used a cut-off score of 30 to indicate a significant risk of PTSD [9,10]. The same person (RRLF), a psychologist with ICU interviews experience [8], conducted all interviews.
Statistical Analysis
Data are presented as the mean ± standard deviation (SD) or the median and the 25th and 75th percentiles (IQR) if distributions were normal or skewed, respectively. Continuous variables were compared using Mann-Whitney or unpaired t-tests, as appropriate. Fisher's exact test or Chi-squared tests were used for dichotomous variables. To evaluate the family HADS score overtime, we fit two-way repeated measures ANOVA, with Bonferroni correction for post-hoc analysis.
All statistical tests were performed using the commercial SPSS21.0 package for Windows (Armonk, NY: IBM Corp).
Results
From March 2011 to March 2013 a total of 576 ICU patients were analyzed. Of those, 95 were poor prognosis patients. They were admitted to the ICU due the postoperative status (27.4%), acute respiratory failure and/or pulmonary diseases (24.2%), shock (20.0%), neurologic diseases (14.7%), cardiovascular diseases (6.3%), acute renal failure (2.1%) and others (5.3%). Table 1 shows the variables according to poor prognosis status in the ICU.
Poor prognosis patients needed more mechanical ventilation, tracheotomy and vasopressors, had greater ICU LOS, higher SAPS 3 score and SOFA when compared with others (Table 1) and we observed that metastatic tumor disease was the most prevalent clinical conditions among poor prognostic patients (Table 2).
The characteristics of family members, anxiety, depression and PTSD symptoms were described in Table 3. Family members of poor prognosis patients presented higher HADS score than family members of patients on the group without poor prognosis (p<0.001, for all time points). Family members of both groups had their HADS score decreased overtime (p<0.001), although family members of poor prognosis patients had a delayed improvement (p=0.024).
We observed that poor prognosis patients had high mortality at ICU (32.6%), and at the follow-up: at 30-days mortality was of 60.0% and at 90-days it was of 73.5% (p<0.001, for all) (Figure 1).
Discussion
Our results suggest that patients with poor prognosis were more likely to receive aggressive treatments during ICU stay. Nowadays, for patients with incurable diseases, conversations about EOL care are strongly recommended as early as possible. When these conversations take place early, patients are less likely to receive aggressive care and have better quality of life before death [5,6].
According to the World Health Organization, Palliative care is an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and thorough assessment and treatment of pain and other problems, physical, psychosocial and spiritual [16].
| Variables |
Poor prognosis n=95 |
Non-Poor prognosis n=481 |
p-value |
| Age, years |
67.9 ± 16.2 |
64.4 ± 18.0 |
0.075 |
| SAPS 3 points |
68.56 ± 16.0 |
51.12 ± 17.5 |
<0.001 |
| SOFA points |
|
|
|
| Mean ± SD |
4.81 ± 3.2 |
2.81 ± 2.8 |
<0.001 |
| Median [IQR] |
4 [2-7] |
2 [0-4] |
| Medical admission reason |
69 (72.6) |
237 (49.3) |
<0.001 |
| ICU LOS (Days) |
|
|
|
| Mean ± SD |
14.2 ± 16.2 |
7.9 ± 9.8 |
<0.001 |
| Median [IQR] |
8 [5-18] |
4 [3-8] |
| Male Gender, n(%) |
46 (48.4) |
287 (59.6) |
0.043 |
| Mechanical Ventilation, n (%) |
47 (50) |
158 (32.9) |
0.002 |
| Mechanical Ventilation (Days) |
|
|
|
| Mean ± SD |
11.83 ± 15.0 |
5.85 ± 6.7 |
0.030 |
| Median [IQR] |
7 [3-15] |
3 [2-6] |
| Tracheotomy, n (%) |
11 (11.6) |
24 (5.0) |
0.014 |
| Vasopressors, n (%) |
52 (54.7) |
177 (36.8) |
0.001 |
| Renal replacement therapy, n(%) |
12 (12.6) |
52 (10.8) |
0.606 |
Table 1: Demographic data of patients according to poor prognosis status at ICU.
| Clinical Conditions referring to secondary diagnosis in poor prognosis patients (n=95) |
N(%) |
| Metastatic tumor |
58 (61.0) |
| Dementia |
13 (20.0) |
| Severe Chronic Kidney Disease |
11 (11.6) |
| Malignant Lymphoma or Leukemias |
7 (7.4) |
| Cerebrovascular Disease |
7 (7.4) |
| Chronic Lung Disease |
6 (6.3) |
| Heart Failure |
6 (6.3) |
| Chronic Liver Disease |
3 (3.1) |
| Hemiplegia |
3 (3.1) |
Table 2: Clinical conditions referring to secondary diagnosis in patients with poor prognosis.
At end-of-life, aggressive interventions may not only be futile but also inappropriate because may impair the QOL and increase the symptoms of anxiety, depression and PTSD for both patients and family members [7].
We observed that family members suffer more when compared to patients with curative disease. We understand that the suffering of family members of dying patients was not only due to death but additionally it could be due to the lack of comfort, to the poor discussions on EOL care and to the aggressive treatments of patients beyond benefiting, in view of their poor health status. The above issues on intervention must be discussed, since family members of those who did not benefit with mechanical ventilation are at increased risk of psychological symptoms [17].
This study showed the lower survival 30-days and 90-days post ICU discharge of poor prognosis patients and may represent a missed opportunity to improve EOL care. Furthermore, we showed that incurable patients had an increase ICU length of stay, needed more time under mechanical ventilation, and more need of vasoactive drugs. Previous data have pointed out to the importance to better select ICU admissions based on characteristics of disease, their prognosis and the benefits from intensive care support [18]. In the present study, we showed that advanced cancer is a common diagnosis among ICU patients.
Many studies have demonstrated the significant burdens of cancer care in terms of healthcare expenditures and resource use. Therefore, we need advanced directives that limited transfer to an ICU to diminish the patients and family members’ suffer and the costs of unbeneficial treatments. In Brazil, it is not widespread the culture of advanced directives and only recently a resolution of the Federal Council of Medicine was formal regulated and recognized (CFM Nº 1805/2006. DOU, November 28, 2006) as well as the revised 2010 Brazilian Code of Medical Ethics determine that EOL decisions for incompetent terminally ill patients should necessarily be discussed with surrogates, but family members are frequently still not involved in such decisions [19]. Additionally, education in medical and nursing schools from many countries (including Brazil) is focused mostly on curative care, and there is little training in palliative medicine [20].
The study of Forte et al. shows that education in End-of-Life care for physicians can modify EOL practice in the ICU. According to them, ICU physicians reading at least four articles per year on ethical aspects were more prone to involve family and nurses in the EOL process, as well not apply “full code”, had less aggressive attitude and more interest in discussing end-of-life care [21]. There are some limitations in our study. First, we used a questionnaire with no possibility of clarifying other questions. Furthermore, the IES and HADS are screening tools rather than diagnostic tools and provide information only about symptom levels. Another limitation is that we followed family members only three months after ICU and some studies have been demonstrated that family members have an increased risk of depressive and/or anxiety disorders as well as post-traumatic stress more than one year following a relative’s stay in ICU, principally when occur the patient’s death during ICU stay or with high risk of death [22,23].
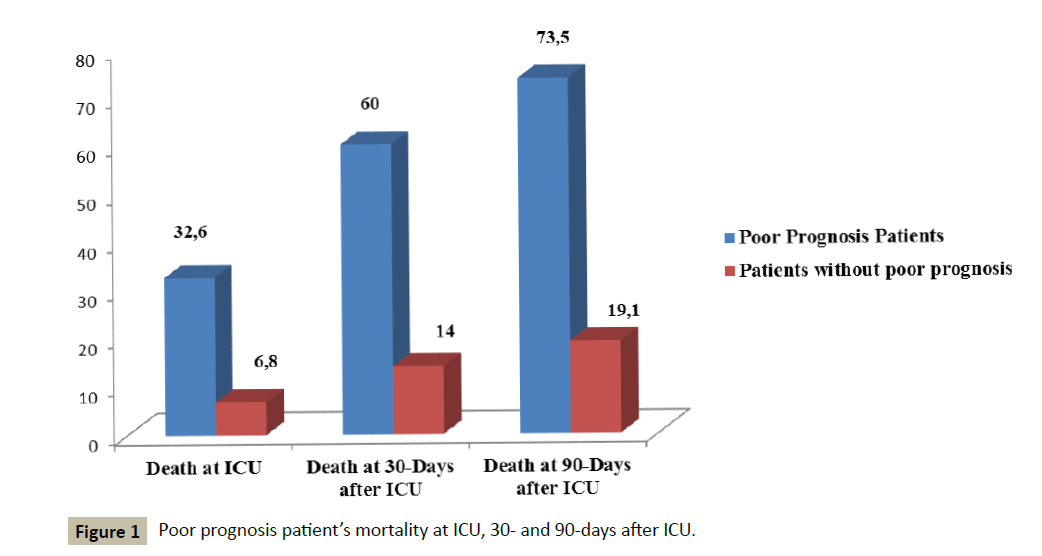
Figure 1 :Poor prognosis patient’s mortality at ICU, 30- and 90-days after ICU.
Finally, the greater limitation of this study is that we lacked the information about the number of patients attended by the Palliative Care team. Indeed, our hospital implemented a group of Palliative Care with close contact with the ICU team. This interaction should be an interesting point to us explore in our cohort. We know that the integration of Palliative Care with standard oncologic care may facility the optimal and appropriate administration of anticancer therapy, especially during the final months of life [11]. Nelson and colleagues show us various benefits of integrating Palliative Care in the ICU, including the increase of family satisfaction and comprehension and the decrease of symptoms of anxiety, depression and post-traumatic stress disorders [12].
Since the conclusion of SUPPORT [2], a number of studies have suggested that interventions to improve clinician–family communication in the ICU can result in improved quality of care. Communication about the goals of care in this setting should be a high priority as studies suggest that the effective ICU communication may diminish the psychological distress among family members of critically ill patients [10]. Many studies have shown that family members of patients who died in the ICU are at higher risk of developing PTSD [8,9,22-24].
In addition, we observed that too old patients with irreversible medical conditions were receiving advanced life care treatment notwithstanding higher ICU mortality [25]. Several studies pointed out that ICU refusal rates increase according to patient age, underlying disease, prior cognitive impairment, dependency status, and medical criteria [25-28]. Our ICU has an open model and the decision to admitted patients comes mainly from the external assistant physician and family, limiting our power to explore the recommendation.
Because the decision to recommend ICU admission is based on complex criteria, and to ensure appropriate utilization of ICU resources without depriving critically ill patients of a chance to recover, the European Societies of Critical Care Medicine has developed recommendations for ICU admissions, screening and discharge [29]. The implementation of these guidelines, improvement of communication with family members and integration of Palliative Care team is a challenge that deserves an interdisciplinary approach.
Conclusion
The impact of poor prognosis patients admitted to the ICU on their family members was stronger. We observed higher scores of symptoms of anxiety, depression and post-traumatic distress among this group. In addition, family witnessed great suffering involving loss of their loved ones.
Acknowledgement
The authors thank Eugênia Deheinzelin for English review.
Funding acknowledgement
This study was supported by “Fundação de Amparo à Pesquisa do Estado de São Paulo”- FAPESP- Process n° 11/05672-1.
Author’s Contribution
Study concept and design, Renata Rego Lins Fumis; acquisition of data, Renata Rego Lins Fumis; analysis and interpretation, Renata Rego Lins Fumis, Paulo Martins; drafting of the manuscript, Renata Rego Lins Fumis, Paulo Martins; and study supervision, Guilherme Schettino and Renata Rego Lins Fumis.
| Variables |
Family members of poor prognosis patients (n=90) |
Family members of patients without poor prognosis (n=381) |
p-value |
| Age (Years) , mean ± SD |
53.2 ± 12 |
52.6 ± 13 |
0.702 |
| Gender female |
71 (78.8) |
297 (77.9) |
0.847 |
| Spouse |
36 (40.0) |
186 (48.8) |
0.132 |
| College education |
75 (83.0) |
298 (78.2) |
0.282 |
| Religious background |
61 (67.7) |
263 (69.0) |
0.818 |
| Previous family experience with ICU |
60 (66.6) |
283 (74.2) |
0.144 |
| Family staying time in the ICU (hours/day), median [IQR] |
12 [8-19] |
12 [8-23] |
0.143 |
| Anxiety at ICU |
33 (36.6%) |
126 (33.0%) |
0.516 |
| Depression at ICU |
23 (25.5%) |
59 (15.5%) |
0.023 |
| Anxiety and Depression at ICU |
19 (21.1%) |
45 (11.8%) |
0.021 |
| HADS at ICU |
|
|
|
| Mean ± SD |
14.67 ± 8.5 |
12.16 ± 8.4 |
0.007 |
| Median [IQR] |
13 [9-20] |
11 [6-17] |
| 30-days after ICU (n=374) |
n=71 |
n=303 |
|
| Anxiety at 30 day |
18 (25.3%) |
45 (14.8%) |
0.033 |
| Depression at 30 day |
21 (29.5%) |
40 (13.2%) |
0.001 |
| Anxiety and Depression at 30 day |
15 (21.1%) |
22 (7.3%) |
<0.001 |
| PTSD at 30 day |
13 (18.3%) |
30 (9.9%) |
0.046 |
| HADS 30 |
|
|
|
| Mean ± SD |
13.72 ± 9.7 |
8.57 ± 8.5 |
<0.001 |
| Median [IQR] |
12 [6-21] |
7 [1-14] |
| IES 30 |
13.62 ± 15.7 |
8.50 ± 13.6 |
0.013 |
| Mean ± SD |
13.62 ± 15.7 |
8.50 ± 13.6 |
0.004 |
| Median [IQR] |
8 [0-23] |
1 [0-12] |
| 90-days after ICU (n=348) |
n=66 |
n=282 |
|
| Anxiety at 90 day |
12 (18.2%) |
34 (12.0%) |
0.186 |
| Depression at 90 day |
13 (19.7%) |
29 (10.3%) |
0.035 |
| Anxiety and Depression at 90 day |
8 (12.1%) |
20 (7.1%) |
0.176 |
| PTSD at 90 day |
11 (16.7%) |
29 (10.3%) |
0.143 |
| HADS 90 |
|
|
|
| Mean ± SD |
10.94 ± 10.1 |
6.65 ± 8.9 |
<0.001 |
| Median [IQR] |
10 [1-17] |
2 [0-11] |
| IES 90 |
|
|
|
| Mean ± SD |
10.11 ± 16.2 |
6.70 ± 13.8 |
0.056 |
| Median [IQR] |
0 [0-16] |
0 [0-4] |
| Median [IQR] |
17 [6-24] |
8 [4-14] |
Table 3: Characteristics of family members according to patients’prognosis status.
References
- Angus DC, Barnato AE, Linde-Zwirble WT, Weissfeld LA, Watson RS, et al. (2004) Use of intensive care at the end of life in the United States: An epidemiologic study. Crit Care Med 32:638-643.
- A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT).The SUPPORT Principal Investigators. (1995) JAMA 274:1591-1598.
- Puntillo KA, Arai S, Cohen NH, Gropper MA, Neuhaus J, et al. (2010) Symptoms experienced by intensive care unit patients at high risk of dying. Crit Care Med 38: 2155-2160.
- Ellershaw J, Ward C (2003) Care of the dying patient: The last hours or days of life. BMJ 326: 30-34.
- Constance Dahlin, ANP-BC, ACHPN, FPCN, FAAN (2013) National Consensus Project for Quality Palliative Care: Clinical practice guidelines for quality care.
- National Comprehensive Cancer Network (2015) Practice guidelines in oncology: Palliative care,USA.
- Wright AA, Keating NL, Balboni TA, Matulonis UA, Block SD, et al. (2010) Place of Death: Correlations with Quality of Life of Patients with cancer and predictors of bereaved caregivers? mental health. J ClinOncol 28: 4457-4464.
- Fumis RR, Ranzani OT, Martins PS, Schettino G, et al. (2015) Emotional Disorders in Pairs of Patients and Their Family Members during and after ICU Stay. PLoS One 10:e0115332.
- Azoulay E, Pochard F, Kentish-Barnes N, Chevret S, Aboab J, et al. Risk of post-traumatic stress symptoms in family members of intensive care unit patients. Am J RespirCrit Care Med171:987-994.
- Lautrette A, Darmon M, Megarbane B, Joly LM, Chevret S, et al. (2007) A communication strategy and brochure for relatives of patients dying in the ICU. N Engl J Med 356:469-478.
- Temel JS, Greer JA, Muzikansky A, Gallagher ER, Admane S, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med 363:733-742.
- Nelson JE, Bassett R, Boss RD, Brasel KJ, Campbell ML, et al. (2010) Models for structuring a clinical initiative to enhance palliative care in the intensive care unit: a report from the IPAL-ICU Project (Improving Palliative Care in the ICU). Crit Care Med 38:1765-1772.
- Back AL, Park ER, Greer JA, Jackson VA, Jacobsen JC, et al. (2014) Clinician roles in early integrated palliative care for patients with advanced cancer: a qualitative study. J Palliat Med 17:1244-1248.
- Botega NJ, Bio MR, Zomignani MA, Garcia C Jr, Pereira WA, et al. (1995) Mood disorders among inpatients in ambulatory and validation of the anxiety and depression scale HAD. Rev SaudePublica 29:355-363.
- Oliveira e Silva AC, Nardi AE, Horowitz M (2010) Brazilian version of the Impact of Event Scale (IES): translation and cross-cultural adaptation. Rev Psiquiatr Rio GdSul 32: 86-93.
- World Health Organization. Definition of Palliative Care.
- Erin KKross, Ruth A Engelberg, Cynthia J Gries, Elizabeth L Nielsen, Douglas Zatzick, et al. (2011) ICU care associated with symptoms of depression and posttraumatic stress disorder among family members of patients who die in the ICU. Chest 139:795-801.
- Azoulay E, Soares M, Darmon M, Benoit D, Pastores S, et al. (2011) Intensive care of the cancer patient: recent achievements and remaining challenges. Ann Intensive Care 1: 5.
- Conselho Federal de Medicina. Resolução CFM 1.805/2006 (2006) Diário Oficial da União, Seção I:169.
- Soares M, Terzi RG, Piva JP (2007)End-of-life care in Brazil. Intensive Care Med 33:1014-1017.
- Forte DN, Vincent JL, Velasco IT, Park M, et al. (2012) Association between education in EOLcare and variability in EOL practice: a survey of ICU physicians. Intensive Care Med. 38: 404-412.
- Schmidt M, Azoulay E (2012)Having a loved one in the ICU: the forgotten family.Curr Opin Crit Care 18: 540-547.
- Davidson JE, Jones C, Bienvenu OJ (2012) Family response to critical illness:postintensive care syndrome-family. Crit Care Med 40: 618-624.
- Gries CJ, Engelberg RA, Kross EK, Zatzick D, Nielsen EL, et al. (2010) Predictors of symptoms of posttraumatic stress and depression in family members after patient death in the ICU. Chest 137: 280-287.
- Sprung CL, Artigas A, Kesecioglu J, Pezzi A, Wiis J, et al. (2012) The Eldicus prospective, observational study of triage decision making in European intensive care units. Part II: intensive carebenefit for the elderly. Crit Care Med 40:132-138.
- María-Consuelo P, Patricia V, Natalia GG, Jimena L, Rocío M, et al. (2013)Characteristics and outcomes of elderly patients refused to ICU. Scientific World Journal. 2013: 590837.
- Garrouste-Orgeas M, Montuclard L, Timsit JF, Reignier J, Desmettre T, et al. (2005) Predictors of intensive care unit refusal in French intensive care units: a multiple-center study. Crit Care Med 33:750-755.
- Reignier J, Dumont R, Katsahian S, Martin-Lefevre L, Renard B, et al. (2008) Patient-related factors and circumstancessurrounding decisions to forego life-sustaining treatment, including intensivecare unit admission refusal. Crit Care Med 36: 2076-2083.
- Society of Critical Care Medicine Ethics Committee (1994) Consensus statement on the triage of critically ill patients. JAMA 271: 1200-1203.

