Muaiyed M Buzayan*
Prosthodontics Department, Dental Faculty, Segi University, Petaling Jaya, Malaysia
*Corresponding Author:
Muaiyed M Buzayan
Prosthodontics Department
Dental Faculty, Segi University
Petaling Jaya, Malaysia
Tel: 00218924729577
E-mail: Muaiyed_zyan@hotmail.com
Received Date: August 08, 2017 Accepted Date: August 11, 2017 Published Date: August 14, 2017
Citation: Buzayan MM. The Hollow Bulb Obturator Fabrication, Where do We Stand in 2017. Periodon Prosthodon 2017, Vol.3 No.2:10. doi: 10.21767/2471-3082.100035
Copyright: © 2017 Buzayan MM. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Editorial
Maxillectomy defects can result in oroantral communication that may lead to difficulty in swallowing, deglutition, impaired speech, and not to mention the resultant facial disfigurement. The prosthodontist in addition to the surgeon of course, plays a significant role in restoration and rehabilitation of such defects, as good functional results have been reported for patients provided with obturator prostheses post surgically [1,2].
The Glossary of Prosthodontic Terms de- fines an obturator as “a maxillofacial prosthesis used to close a congenital or acquired tissue opening, primarily of the hard palate and/or contiguous alveolar/soft tissue structures” [3].
The bulb portion, as it obdurate the defect, it must also add up the retention and stability by extending adequately into the defect to achieve a seal [4,5]. On the other hand, more extension increases the weight of the prosthesis and with the gravitational force as a dislodging factor, that is going to be a real issue affects the prosthesis stability hence, the idea of making prosthesis with hollow bulb to make the prosthesis lighter became a crucial matter [4].
Numerous methods and techniques have been introduced and advocated for open/closed hollow bulb obturator fabrication. The open and close hollow bulb types of obturators, both are lightweight prostheses which is easily tolerated by the patient [6-8]. Yet, open hollow bulb obturators have that advantages of accumulating mucous, food, and fluids what lead to bad odour and taste (Figure 1). That necessitates numerous cleanings or a vent adding to eliminate accumulation in the bulb [9].
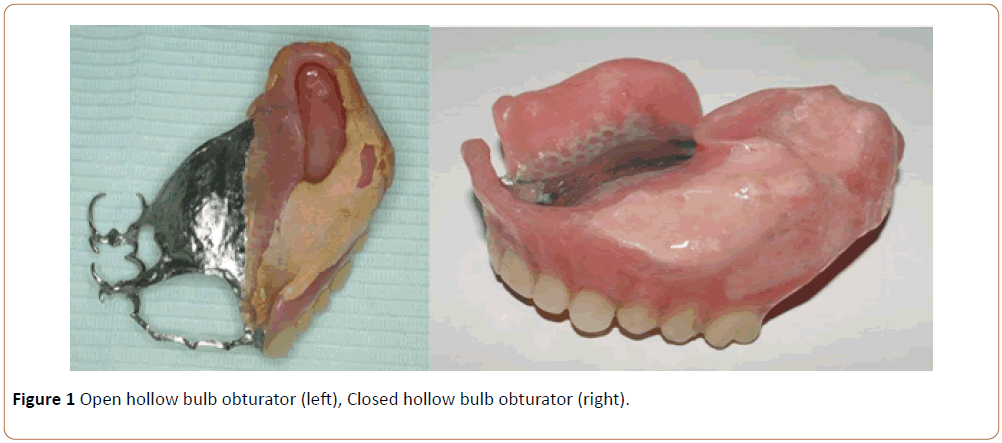
Figure 1: Open hollow bulb obturator (left), Closed hollow bulb obturator (right).
On the other hand, closed hollow bulb obturators, do not pool moisture and no accumulations of any type, while still extending adequately into the defect and providing more retention and support, various materials have been advocated for bulb fabrication [10]. Some of these materials include lightcured resin, autopolymerising acrylic resin, and silicone rubber [11,12]. Silicone rubber, while advantageous in particular clinical situations, yet, it has porous nature, and poor longterm durability, what necessitates routinely from period to period replacement [7,13]. Another advantageous material is heat-cured acrylic resin, which is still considered one of the most durable and biocompatible materials for fabrication of the obturator [3].
For the hollow bulb obturator, the major difficulty was how to fabricate it in reduced number of steps and minimal sealing areas Several methods have been introduced for the fabrication of the hollow bulb obturator, including the use of materials such as salt, sugar and ice as mediums inside the bulb to support its hollow nature during processing [14-18]. However, the previously mentioned methods generally cause contamination of the acrylic resin and create a sealed area, which is a potential site of leakage and discoloration. Not to mention the need for complex and multiple laboratory procedures. Others introduced the placement of an acrylic resin shim, and the incorporation of polyurethane foam into the defect area to produce the hollow section [19,20]. These methods have the disadvantages of adding more weight to the obturator and extra thickness to the hollow bulb obturator walls [9]. Minsley et al. [21] suggested the use of a plaster index for the fabrication of the hollow bulb of the obturator, while simultaneously fabricating a heat-cured acrylic denture base used for maxillomandibular records followed by final waxing and processing of the obturator. Another technique is the double-flask technique described by El Mahdy [22] allowing for the complete fabrication of the hollow bulb obturator from the wax try-in stage to completion of the prosthesis; however, this technique requires extra laboratory steps, including heat processing of the obturator bulb and the tooth portion separately with two denture flasks and then heat processing these sections for the second time togetherdouble processing. Acrylic resin may also flow into the hollow portion during the final processing stage [9].
Similarly, McAndrew et al. [9] introduced an investment method for fabrication of a closed hollow bulb obturator. That technique included the use of three sections of a denture processing flask; however, the procedure incurred additional laboratory procedures where multiple flasks were required.
Recently, another technique was introduced to fabricate the closed hollow bulb obturator with added group of advantages, it can be made in one step processing and yet no sealing area at all, therefore reducing laboratory time while maintaining the obturator’s light weight and cleanliness in which the author has built a plaster index to fabricate the bulb from thermoplastic material first then fixed in the defect area, after then, the conventional processing procedure was followed (Figure 2) [23].
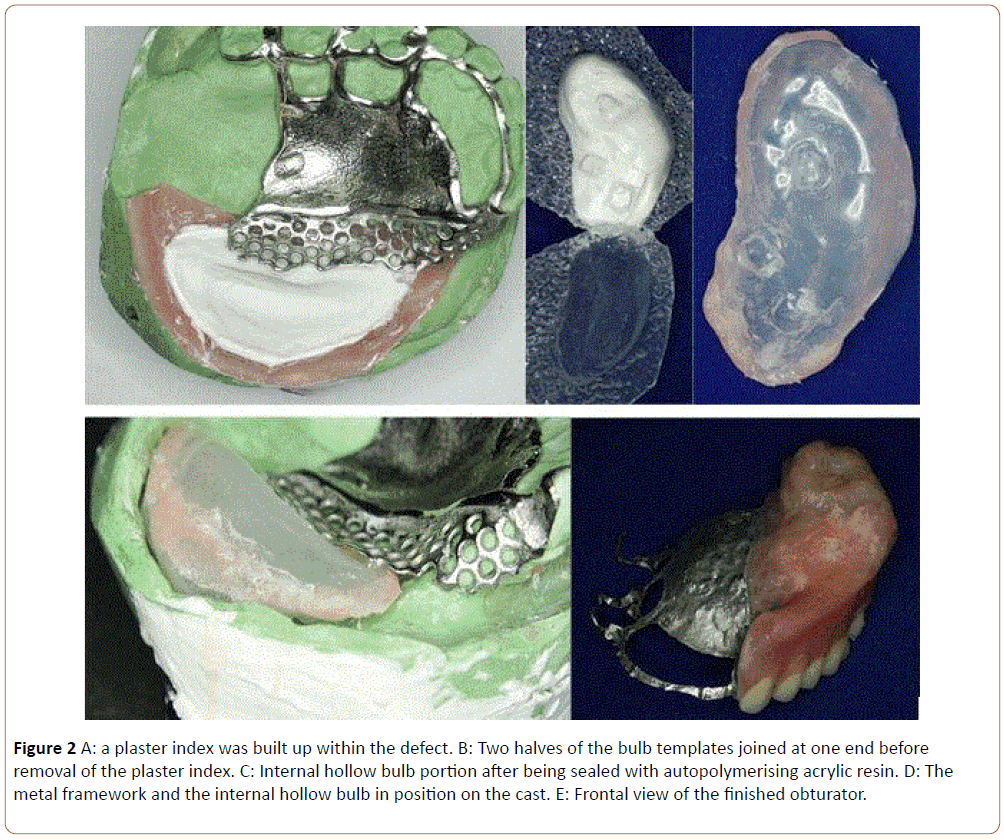
Figure 2: A: a plaster index was built up within the defect. B: Two halves of the bulb templates joined at one end before removal of the plaster index. C: Internal hollow bulb portion after being sealed with autopolymerising acrylic resin. D: The metal framework and the internal hollow bulb in position on the cast. E: Frontal view of the finished obturator.
We can feel while reading the upper paragraph, the evolving in the obturator fabrication methods, however, the target was always and still to get prosthesis which is lighter, easy to clean, hygienic, with minimal steps and that promotes the healing process. This was some sort the obturator fabrication history, so what about its future.
Now, the dentistry has entered new era where is the (3D) virtual treatment planning designing and fabricating of the prosthesis became very common and more handy, and in this era where the CAD-CAM dentistry started to be implicated in the prosthodontics. The thinking behavior in how to do and how to construct started to change. So, the question now is, when we are going to see an obturator that is made completely by the CAD-CAM technology, without the need for sophisticated impression and fabrication techniques.
References
- Irish J, Sandhu N, Simpson C (2009) Quality of life in patients with maxillectomy prostheses. Head Neck 31: 813-821.
- Rieger JM, Wolfaardt JF, Jha N, (2003) Maxillary obturators: the relationship between patient satisfaction and speech outcome. Head Neck 25: 895-903.
- Glossary of Prosthodontic Terms (2005) J Prosthet Dent 94: 10-92.
- Beumer J, Curtis TA, Marunick MT (1996) Maxillofacial Rehabilitation. In: Prosthesis and Surgical Considerations (ed 1). St Loius, Ishiyaku Euro America, pp. 226-283.
- Schaaf NG (2004) Maxillofacial prosthetics. In: Winkler S (eds) Essentials of Complete Denture Prosthodontics. St. Louis, Ishiyaku Euroamerica, pp: 403-416.
- Wu YL, Schaaf NG (1989) Comparison of weight reduction in different designs of solid and hollow obturator prostheses. J Prosthet Dent 62: 214-217.
- Brown KE (1970) Clinical considerations improving obturator treatment. J Prosthet Dent 24: 461-466.
- Desjardins RP (1978) Obturator prosthesis design for acquired maxillary defects. J Prosthet Dent 39: 424-435.
- McAndrew KS, Rothenberger S, Minsley GE (1998) An innovative investment method for the fabrication of a closed hollow obturator prosthesis. J Prosthet Dent 80: 129-132.
- Phankosol P, Martin JW (1985) Hollow obturator with removable lid. J Prosthet Dent 54: 98-100.
- Benington IC, Lappin C, Linden GJ (1996) The clinical success and periodontal evaluation of patients rehabilitated with light-cured obturators. J Oral Rehabil 23: 135-138.
- Kocacikli M, Yalug S, Yazicioglu H (2008) Fabricating a hollow obturator with visible light-cured resin system. J Prosthodont 17: 596-598.
- Taicher S, Rosen AG, Arbree NS (1983) A technique for fabrication of polydimethylsiloxane-acrylic resin obturators. J Prosthet Dent 50: 65-68.
- Matalon V, La FH (1976) A simplified method for making a hollow obturator. J Prosthet Dent 36: 580-582.
- Parel SM, LaFuente H (1978) Single-visit hollow obturators for edentulous patients. J Prosthet Dent 40: 426-429.
- Schneider A (1978) Method of fabricating a hollow obturator. J Prosthet Dent 40: 351.
- Brown KE (1969) Fabrication of a hollow-bulb obturator. J Prosthet Dent 21: 97-103.
- Browning JD, Kinderknecht J (1984) Fabrication of a hollow obturator with fluid resin. J Prosthet Dent 52: 891-895.
- Chalian VA, Barnett MO (1972) A new technique for constructing a one-piece hollow obturator after partial maxillectomy. J Prosthet Dent 28: 448-453.
- Tanaka Y, Gold HO, Pruzansky S (1977) A simplified technique for fabricating a lightweight obturator. J Prosthet Dent 38: 638-642.
- Minsley GE, Nelson DR, Rothenberger SL (1986) An alternative method for fabrication of a closed hollow obturator. J Prosthet Dent 55: 485-490.
- El Mahdy AS (1969) Processing a hollow obturator. J Prosthet Dent 22: 682-686.
- Buzayan MM, Ariffin YT, Yunus N (2013) Closed hollow bulb obturator-one-step fabrication: a clinical report. Journal of Prosthodontics 22: 591-595.

