Keywords
Anesthesia information management systems; Interoperability; Data access; Business intelligence; Extract-transform-load; Power BI
Background
An anesthesia consultation is a clinical evaluation medical appointment carried out before any anesthetic act, with the objective of programming the next steps towards this act [1]. This appointment is performed by a Clinic/Hospital Anesthesiology Team where the patient will be submitted to the anesthetic-surgery procedure, preferably several days before the programmed surgery. In this appointment, the anesthesiologist doctor questions a patient in order to be informed about physical and psychological conditions and any clinicalconcerning information about that patient. This information helps in the measure of the anesthetic-surgery risk [2]. In addition, anesthesia medical appointments help establishing doctor-patient relationship, diminishing anxiety and increasing patient confidence, leading to a proper preparation of future events, diminishing the chances of a postponed surgery [1,2].
A patient’s anesthetic documentation in the medical record is quite different from other clinical encounters such as writing a surgical procedure note. Anesthesia records are suited to accurately capture a patient’s anesthetic experience in a succinct format, allowing anesthesiologists to make proper diagnoses and correct treatment decisions. An Anesthesia Information Management Systems (AIMS) is built around the electronic anesthesia record and incorporates anesthesia-relevant data pulled from different systems such as laboratory, imaging, communication, pharmacy, and scheduling [1]. These systems can provide a lot of benefits if they are fully integrated with the other health information technologies. The ability of an anesthesia information management system to collect data automatically enables anesthesiologists to reliably create an accurate record anytime, regardless of other concurrent demands [3]. AIMS were developed based on various technological platforms and different programming languages, coexisting in the same organization with large number of heterogeneous and spread systems. This is the reason why interoperability of AIMS with other health information systems is still very weak and one of the main reasons why development projects of these systems in this sector are difficult to implement [2].
The process of recording the data obtained during an anesthesia consultation has evolved over time with new systems being developed and upgraded to make data management and distribution easier from a user point of view [3]. There has been a substantial increase in the adoption of electronic health records among hospitals that made AIMS, integral components in health information systems. Nowadays, the number of operating rooms with AIMS is expected to be dramatically higher based on the presence of more AIMS being available from product vendors, the financial incentives (and penalties) that have been offered by the governments across the world and because of the ease of use that these systems represent.
Healthcare organizations procude significant volumes of data and have a lot of information to deal with in order to make the best decision as fast as possible [4,5]. One solution that can improve the decision-making process is Business Intelligence (BI) [6]. BI tools can help transform raw data into smart information and knowledge. BI refers to methodologies and technologies for the collection, integration, analysis and presentation of all relevant information [6]. There are many BI tools such as extract transform and load (ETL), data warehouse (DW), online analytical processing (OLAP), and dashboards [7-9]. Health Information Systems deals with resources, devices, and methods required to optimize the acquisition and use of information in health and biomedicine [10]. With the evolution of Information Technologies, many healthcare institutions like hospitals and clinics started implementing informatic systems to increase the quality of their services [11]. Healthcare information systems are fundamental in managing, organizing and processing clinical information due to the fact that resources and time are critical in this environment [10-12].
The model presented heareby allows users to take advantage of Business Intelligence motholodogies in order to provide better care to patients. Accessing information anytime anywhere can ensure better patient treatment and better service.
Methods
A data warehouse is a collection of technologies aimed at enabling the decision maker to make better and faster decisions. They differ from operational databases due to the fact that they are oriented to a subject, integrated, time variant, larger, summarized, not normalized and perform OLAP [7].
To build a DW, it should be run an ETL process constituted by three phases, which are complex procedures that are in charge of feeding a data repository starting from data sources [9]. The first phase is named Extraction, which consists in data extraction from different data sources with their distinct set of characteristics that need to be managed in order to effectively extract data for the ETL process. These characteristics such as communication protocol or operating systems can be different from source to source. This extraction task can be divided in Initial Extraction if it is the first time we get data from the sources or in Incremental Extraction if the ETL processes refresh the DW with the modified and added data in the source systems since the last extraction [9]. The second phase is called Transformation, where data previously extracted is transformed and cleansed with the objective of turning it into accurate data which is correct, complete, consistent and unambiguous. In this step, data is joined from different sources and is converted to the same dimension, using the same units, there is the generation of surrogate keys and aggregates and it may be necessary sorting and deriving new calculated values, for example [9]. The third and last phase is Loading, where extracted and transformed data is written into the dimensional structures actual accessed by end users and application systems. In this step, it is required the loading of both dimension and fact tables. This process is a can lead, in case of anesthesia to better AIMS, by improving its usability, performance, maintainability, security, interoperability, recovery systems and functionality [8].
The case study was centered in the anesthesia medical appointment data from various hospitals concerning the year of 2016. The objective was to treat information about 8339 anesthesia episodes in a. xslx document in order to analyze it correctly and facilitate its future consultation. Due to this big amount of data, the first step was to organize the information section in a multidimensional schema. The ETL process was made and after transformation, the data was loaded in MySQL. The last step was building indicators with the objective of presenting the information is a more intuitive and clear way, so it is easier for people to understand it and take value from it. The multidimensional schema describes the data mart from a static point of view, specifying the facts to be monitored, their measures, the hierarchies to be used for aggregation. Specifically, a star schema is a methodology to organize information that consists in a collection of tables that are logically related to each other. To organize the information in a star schema is especially helpful when we are working with a large volume of data as it is designed to measure performance of database products in support of classical data warehousing [8].
The facts table was called “anesthesia” and it is considered “the center of the star schema” as it contains the facts (episodes/ entries in anesthesia). It was necessary to add more information to the facts table such as age, which would be relevant to analyze in the future in order to obtain useful information.
The tables surrounding the facts table, such as “status”, “report”, “module” or “gender” represent the dimension tables. For each dimension, there would be N facts related (relation 1—N). With the exception of the age, birthday, fill_time and creation_date, which represent measures, all the other facts in the anesthesia table correspond to foreign keys that match the primary keys considered in the different dimension tables.
Results
Power BI is a cloud based data analysis, which can be used for reporting and data analysis from wide range of data sources [13]. Using this BI tool, we can visualize the data warehouse, create interactive dashboards and retrieve useful information in a user-friendly way. Figure 1 displays a dashboard that presents general information about the Anesthesis appoitnments. Namely, the monthly distribution of appointments, average age and the gender distribution. From a general perspective, during the year of 2016, 8140 entries in anesthesia have occurred in which women represent approximately 59% of the episodes and the average age is 57.
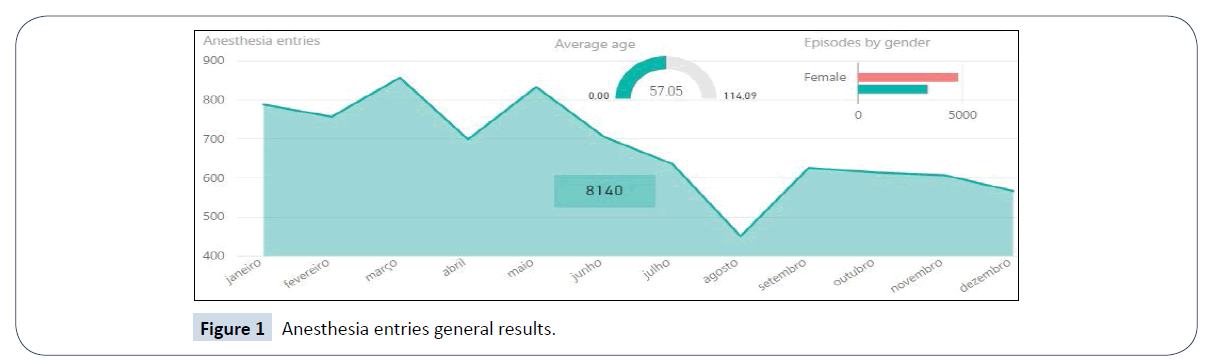
Figure 1: Anesthesia entries general results.
The goals of the pre-anesthetic consultation consist in the identification of clinical problems which may modify perioperative care, the evaluation of a known medical problem which may alter anesthesia care and the formulation of specific plans and alternatives for anesthesia care. Some of these risk factors were available in the data and were extracted in order to give us insights about the patients’ clinical condition, and can be seen in Figure 2.
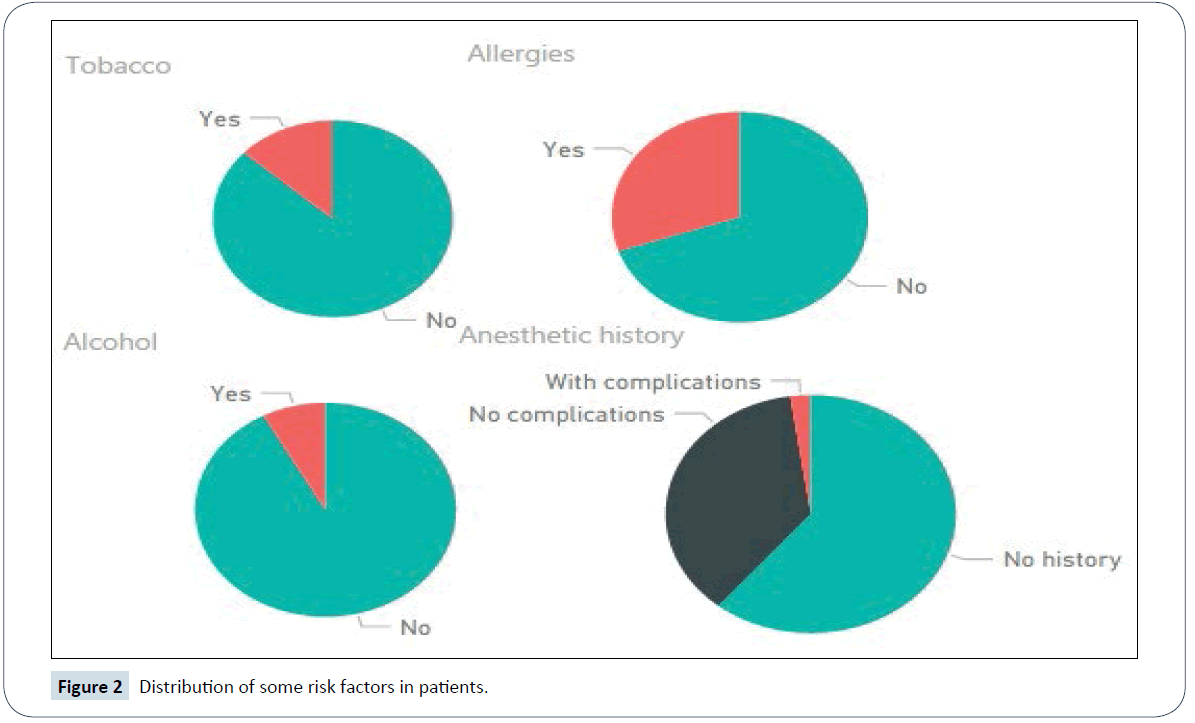
Figure 2: Distribution of some risk factors in patients.
Aging is a universal and progressive physiological phenomenon clinically characterized by degenerative changes in both the structure and the functional capacity of organs and tissues [14]. For this reason, the elderly people represent a significant part of the episodes in our data warehouse, totalizing approximately 34% of the entries.
Common diseases in the elderly have a significant impact on anesthesia and require special care. The risk from anesthesia is more related with the presence of coexisting disease than with the age of the patient. Thus, it is more important to determine the patient's status and estimate the physiologic reserve in the preanesthetic evaluation. Diabetes mellitus type II and cardiovascular disease are very common among geriatric patients being the first one a strong risk factor among the growing elderly population. In Figure 3, it can be observed the deviation in the average age of patients with diabetes mellitus type II, 10% higher than the average age of the patients who do not suffer from this disease.
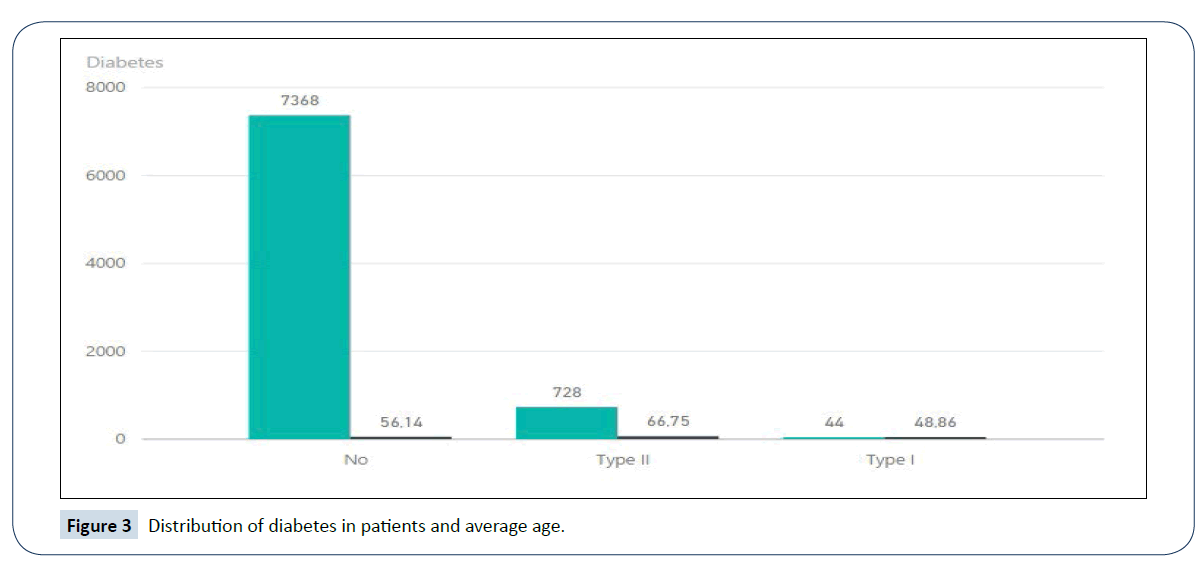
Figure 3: Distribution of diabetes in patients and average age.
To prove the strong incidence of diabetes type II in geriatric patients, the next two graphs presente in Figure 4 it can be observed a 14,47% incidence of diabetes type II in patients with ≥ 65 years whilst 5,73% in patients younger than 65.
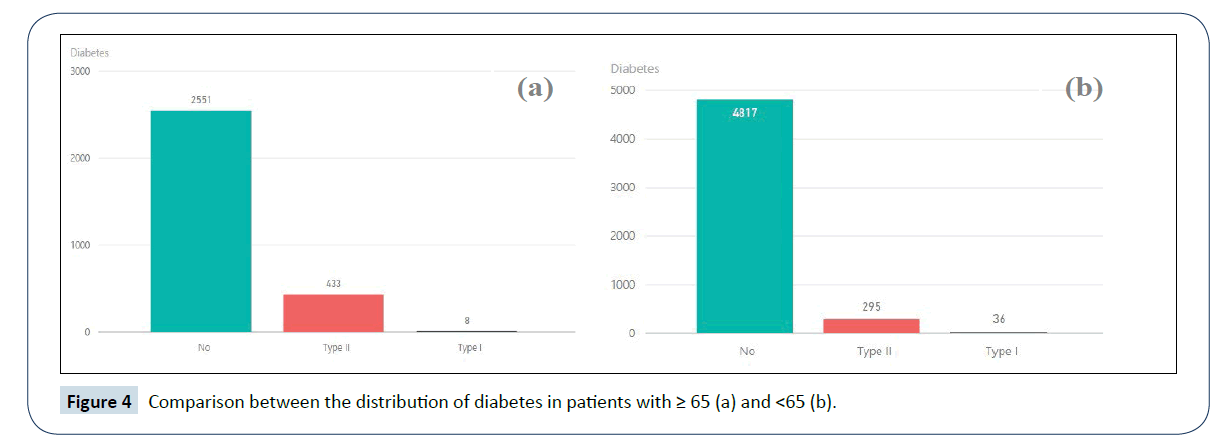
Figure 4: Comparison between the distribution of diabetes in patients with ≥ 65 (a) and <65 (b).
Discussion and Conclusions
A data warehouse allows performing statistics on data from different source systems. In this case study, was developed a data warehouse which stores information related to anesthesia procedures in its medical appointments. In this way, it was allowed to conduct analysis on data from the AIMS of some hospitals from the Northern region of Portugal. The data warehouse constructed has enhanced business intelligence techniques and consistent data with quality. In this way, can be used for clinical researches and for medico-economic purposes. ETL processes have a fast response time when loading and querying in the data warehouse. However, if the volume of data increases a lot in the system, optimization operations should be performed in order not to lose the high performance associated to this process. PowerBI, provided a visual flow of the system’s logic. Data now is presented in an easier way for users to consult. These usage of quality indicators in anesthesia is still not widespread in Portugal or around the world, so there are not many works to compare our data with. Depending on the subject of the information presented, different kind of graphics and techniques were used to present information in the clearest way possible. With maintainability and extensibility in mind, PowerBI provided a metadata-driven structure to the developers. In sum, they can be used to upgrade AIMS, by improving also their usability, security, interoperability, recovery systems and functionality. Anesthetic results, given by PowerBI, are dependent of the content of given data. In this case study, the data is mainly pre-operatively. It is possible, for example, to evaluate the number of anesthesia entries per day, week and month. With this information, hospitals have the ability to predict critical times and be prepared for these situations. This information presented can also determine if the entries in anesthesia are related to sex, to anesthetic history, to special conditions such as asthma or allergies or to important factors like tobacco and alcohol. As it is easy to observe the information in the interface, users can denote a pattern related to anesthesia records and quickly infer other valuable information such as risk factors. As it can be denoted, this whole process has innumerous advantages when integrated in AIMS as it is possible to accompany the quality of pre-operatively indicators, investigate relationships between data and identify good practices, for example. In sum, it helped in the evaluation of the efficiency and quality of the anesthesia process with the objective of improving patient care in hospitals and clinics in Portugal’s Northern region.
Acknowledgments
This work has been supported by Compete: POCI-01-0145- FEDER-007043 and FCT within the Project Scope UID/ CEC/00319/2013.
References
- Ehrenfeld JM, Rehman MA (2011) Anesthesia information management systems: a review of functionality and installation considerations. J Clin Monit Comput 25: 71-79.
- Deng F, Hickey JV (2015) Anesthesia information management systems: an underutilized tool for outcomes research. AANA J 83: 189-195.
- Kadry B, Feaster WW, Macario A, Ehrenfeld JM (2012) Anesthesia information management systems: past, present and future of anesthesia records. Mt Sinai J Med 79: 154-165.
- Jardim SVB (2013) The electronic health record and its contribution to healthcare information systems interoperability. Procedia Technology 9: 940-948.
- Peixoto H, Machado J, Neves J, Abelha A (2010) Semantic interoperability and health records. In E-HEALTH pp: 236-237.
- Jinpon P, Jaroensutasinee M, Jaroensutasinee K (2011) Business intelligence and its applications in the public healthcare system. Walailak Journal of Science and Technology 8: 97-110.
- El-Sappagh SHA, Hendawi AMA, Bastawissy AHE (2011) A proposed model for data warehouse ETL processes. Journal of King Saud University - Computer and Information Sciences 23: 1319-1578.
- Golfarelli M, Rizzi S (2011) Data warehouse testing: a prototype-based methodology. Information and Software Technology 53: 183-1198.
- Kimball R, Caserta J (2004) The data warehouse ETL toolkit: practical techniques for extracting, cleaning, conforming and delivering data. John Wiley & Sons.
- Cardoso L, Marins F, Portela F, Santos M, Abelha A, et al. (2014) The next generation of interoperability agents in healthcare. Int J Environ Res Public Health 11: 5349-5371.
- Miranda M, Salazar M, Portela F, Santos M, Abelha A, et al. (2012) Multi-agent systems for HL7 interoperability services. Procedia Technology 5: 725-733.
- Peixoto H, Santos M, Abelha A, Machado J (2012) Intelligence in interoperability with AIDA, foundations of intelligent systems: 20th International Symposium, Macau, China, pp: 264-273.
- https://powerbi.microsoft.com/en-us/guided-learning/
- Lamer A, Jeanne M, Vallet B, Logier R (2013) Development of an anesthesia data warehouse: preliminary results. IRBM 34: 76-378.

