Hasan T1*, Wong G2,3, Webster A2,3, Gilroy N1, Chen S1,3, Woodhouse E2, Kable K2 and Edmiston N
1Centre for Infectious Diseases and Microbiology, Westmead Hospital, New South Wales, Australia
2Centre for Transplant and Renal Research, Westmead Hospital, New South Wales, Australia
3School of Medicine, University of Sydney, New South Wales, Australia
4HIV/Sexual Health Services, North Coast Public Health, New South Wales, Australia
Corresponding Author:
Tasnim Hasan
Department of Infectious Diseases
Westmead Hospital, Hawkesbury Road
NSW 2145, Australia
Tel: +61(2)88906012
Fax: +61(2)98915317
E-mail: tasnim.hasan@health.nsw.gov.au
Received date: September 11, 2017; Accepted date: October 23, 2017; Published date: October 30, 2017
Citation: Hasan T, Wong G, Webster A, Gilroy N, Chen S, et al. (2017) The First Simultaneous Pancreas, Renal Transplant in a Patient with HIV in Australia. J HIV Retrovirus.Vol. 4 No.1:2
Keywords
HIV; Renal-pancreas; Transplant; Anti-retroviral; Australia
Introduction
Recent experiences suggest that transplantation can be safely conducted in patients with human immunodeficiency virus (HIV) infection. Balancing medication interactions between antiretroviral therapy and immunosuppressive therapy remains a challenge. Eight cases of simultaneous pancreas and kidney (SPK) transplantation in HIV patients with type 1 diabetes mellitus (T1DM) have been reported with good outcomes [1-5]. At transplantation, all patients were under the age of 50 years, with undetectable HIV RNA blood levels. Most were on nucleoside reverse transcriptase inhibitor (NRTI) based regimes. Here we report the first SPK transplantation case in Australia. We highlight that successful transplantation can be achieved in the context of viral resistance, with the use of novel anti-retroviral medications.
Case
A 45 year old male with HIV-1 infection was referred to our facility from a regional area, for SPK transplantation. T1DM was diagnosed aged 19 years, complicated by nephropathy requiring home haemodialysis in the three years leading up to transplantation. HIV was diagnosed, aged 24 years. Eight years later, lamivudine/zidovudine and efavirenz was commenced at a nadir CD4 count of 160 cells/mL. History was notable for coronary artery bypass grafting, previous seizures and fractured humerus.
Over twenty years, modifications to his anti-retroviral regime were necessary because of adverse effects and virological failure (Table 1). In 2011, mutations at positions M184V, K103N, M41L and T215CF were found, precluding the use of most NRTIs. In 2014, despite good virological control, anti-retroviral medications were modified in preparation for transplantation. Protease inhibitors (PI) and etravirine were avoided due to cytochrome P450 inhibition. Instead, a novel combination including subcutaneous enfuviritide was used, along with dolutegravir, maraviroc (CCR5 tropic virus) and renal-adjusted tenofovir disoproxil fumarate (TDF).
| |
June 2002-December 2004 |
January 2005-July 2004 |
July 2005 |
January 2011 |
May 2011-July 2014 |
July 2014-Transplant |
Current |
| NRTI |
Lamivudine/Zidovudine |
Lamivudine/Abacavir |
Lamivudine/Zidovudine/Abacavir/Tenofovir |
Lamivudine/Abacavir |
- |
Tenofovir disoproxil |
Tenofovir alafenamide/Emtricitabine |
| |
| NNRTI |
Efavirenz |
Efavirenz |
- |
- |
Etravarine |
- |
Rilpivirine |
| Protease inhibitor |
- |
- |
Lopinavir/Ritonavir |
Lopinavir/Atazanavir |
Darunavir/Ritonavir |
- |
- |
| Integrase inhibitor |
- |
- |
- |
- |
Raltegravir |
Dolutegravir |
Dolutegravir |
| CCR5 inhibitor |
- |
- |
- |
- |
- |
Maraviroc |
Maraviroc |
| Fusion inhibitor |
- |
- |
- |
- |
- |
Enfuviritide |
- |
| Reason for change |
Adverse effect (anaemia) |
Viral failure |
Patient choice (treatment interruption) |
Side effects (hypotension) |
Avoid potential drug interactions |
Side effects (injection site reactions) |
- |
Table 1: Anti-retroviral regimes over time.
Twelve months later, at the time of transplantation, CD4 count was 518 cells/mL, HIV viral load was undetectable and CMV and EBV IgG were negative. The donor-recipient was 0/6 mismatched on HLA loci. Standard induction therapy included basiliximab, mycophenolate and prednisone. Maintenance immunosuppression was continued with mycophenolate, renally adjusted tacrolimus, a calcineurin inhibitor (CI) and prednisone. Valganciclovir prophylaxis was added.
Therapeutic drug monitoring (TDM) allowed gradual escalation of the CI dose, with the aim to achieve adequate, yet safe, immunosuppression to optimise graft survival. Renal function fully recovered over three weeks, allowing gradual escalation to standard doses of TDF (Figure 1).
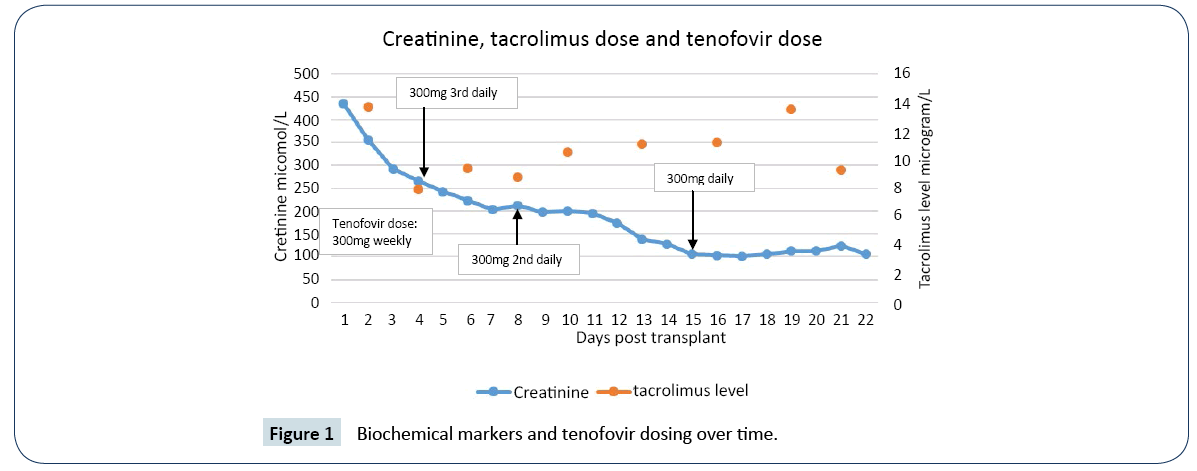
Figure 1: Biochemical markers and tenofovir dosing over time.
Insulin was no longer required post operatively. At discharge, proton pump inhibitor was ceased and enfuviritide was changed to rilpivirine (absorbed in acidic environments). TDF was replaced by Tenofovir alafenamide combined with emtricitabine, a new agent with reduced nephrotoxicity. His general health improved, despite several admissions with psoas collection and a splenic infarct. His 12-month biopsy showed no evidence of acute rejection, with a BANFF score of 0 (t0, i0, g0, cg0, ah0, v0, vv0, ct0, mm0). However, there were signs of early glomerulopathy. HIV viral load remained undetectable.
Discussion
The current case demonstrates that the presence of complex antiretroviral drug resistance patterns, requiring thoughtful antiretroviral treatment regimens, can be managed successfully to allow organ transplantation in HIV patients. The favourable outcome here was consistent with the other case reports (Table 2). Only one patient has been reported as having died, after SPK transplantation, resulting from bacterial sepsis at nine months [1]. Graft failure has been reported in two cases [1,2]. The remaining five organ grafts have functioned at follow up between 5 and 84 months [2-5].
| |
Country |
Age/Sex |
comorbidities |
CD4 at Tx |
HIV VL at Tx |
ART pre Tx |
Days ART w/h post Tx |
ART post Txb |
Major complications |
Survival |
F/U |
| |
|
|
|
|
|
|
|
|
|
Patient |
Pancreas |
Kidney |
|
| Toso et al. [4] |
Switzerland |
39/F |
PVD |
600 |
<50 |
Nil |
N/A |
Nil |
MI |
Y |
Y |
Y |
7 years |
| Genzini et al. [5] |
Brazil |
43/M |
NS |
803 |
<50 |
NS |
NS |
NS |
ATN |
Y |
Y |
Y |
5 months |
| Miro et al. [1] |
Spain |
40/M |
HTN |
523 |
<39 |
Nil for 6 months |
13 |
3TC, TDF, RAL |
Abscess, sepsis, CMV |
N |
N |
Y |
9 months |
| Akthar et al. [3] |
UK |
50/M |
HTN, hyperlipidemia |
752 |
<50 |
RAL, DRV/r, ETV |
Continued |
RAL, DRV/r, ETV |
Nil |
Y |
Y |
Y |
NS |
| Grossi et al. [2] |
Italy |
35/M |
NS |
470 |
<50 |
d4T, 3TC, NFV |
25 |
ZDV, 3TC, EFV |
Pancreatitis, haematoma, abscess |
Y |
N |
Y |
NSd |
| |
Italy |
44/M |
Ex-IVDU, HCV |
470 |
80000 |
Nil |
58 |
3TC, ABC, FPV/r |
TB, bleeding, cholecystitis, abscess |
Y |
Y |
Y |
NS |
| |
Italy |
31/F |
NS |
698 |
<50 |
FTC, NVP, ATV/r |
27 |
3TC, ABC, ATV/r |
Genital HSV, AKI, bleeding, abscess |
Y |
Y |
Y |
NS |
| |
Italy |
49/M |
NS |
598 |
<50 |
d4T, 3TC, EFV |
41 |
3TC, ABC, RAL |
Acute renal rejection, cholecystitis |
Y |
Y |
Y |
NS |
| |
Australia |
41/M |
IHD, seizures, OP |
518 |
<20 |
TDF, DTG, MVC, T20 |
Continued |
TDF, DTG, MVC, T20 |
MI, psoas abscess, splenic infarct |
Y |
Y |
Y |
18 months |
a. All patients transplanted for type 1 diabetes complicated by end stage renal disease, necessitating haemodialysis
b. Immediately post transplantation/ when ART recommenced
c. The patient described was a long-term non progressor HIV patient
d. Exact follow up for each patient not specified, however between 2-5 years
UK: United Kingdom; F: Female; M: Male; PVD: Peripheral Vascular Disease; NS: Not Specified; HTN: Hypertension; IVDU: Intravenous Drug Use; HCV: Hepatitis C Virus; IHD: Ischaemic Heart Disease; OP: Osteoporosis; Tx: Transplantation; HIV: Human Immunodeficiency Virus; VL: Viral Load; ART: Antiretroviral Therapy; RAL: Raltegravir; DRV: Darunavir; r: Ritonavir; ETV: Etravirine; d4T: Stavudine; 3TC: Lamivudine; NFV: Nelfinavir; FTC: Emtricitabine; NVP: Nevirapine; ATV: Atazanavir; EFV: Efavirenz; TDF: Tenofovir; DTG: Dolutegravir; MVC: Maraviroc; T20: Enfuviritide; ZDV: Zidovudine; ABC: Abacavir; FPV: Fosamprenavir; N/A: Not Applicable; MI: Myocardial Infarction; ATN: Acute Tubular Necrosis; CMV: Cytomegalovirus; TB: Tuberculosis; HSV: Herpes Simplex Virus; AKI: Acute Kidney Injury; Y: Yes; N: No; F/U: Follow Up
Table 2: Characteristics of all patients undergoing SPK transplantation in the setting of HIV and T1DM.
Despite recommendations [6] against anti-retroviral treatment interruptions, the peri and post-operative approaches to antiretroviral therapy in SPK transplantation have varied. In one case, anti-retrovirals were withheld, without virological failure, pre-operatively and seven years post [4]. In a case series, antiretrovirals were withheld in the pre and peri-transplantation period to avoid medication interactions. Reintroduction was at 25-58 days, with CD4 counts 71-195 [2]. Our recipient and two other cases received uninterrupted anti-retroviral treatment [3,5].
The challenges faced in managing such patients are diverse. The primary challenge is that drug-drug interactions need to be considered. PIs inhibit the metabolism of CI, necessitating lower doses of CIs [6]. Conversely non-nucleoside reverse transcriptase inhibitors (NNRTI) can increase CI metabolism, necessitating higher doses of CIs [6]. Despite prior PI and NNRTI use, our recipient was prescribed TDF (a NRTI), regardless of risk of nephrotoxicity, as it has minimal interactions with immunesuppressive drugs [6,7] and has antiviral activity despite his resistance profile.
The other agents used: integrase inhibitors (dolutegravir), maraviroc and enfuviritide exhibit minimal interactions with immunosuppressive regimes [6-8]. Enfuviritide, is administered by subcutaneous injection, limiting long-term use. However, once successfully transplanted an alternate regime was established safely.
Other challenges in managing patients requiring SPK transplantation include infective complications. The commonly reported infective complications included abscesses [1,2], urinary tract infections [2,4], CMV viraemia [1], wound infection, bacteraemia and pneumonia [4]. Interestingly, one case was complicated by a psoas abscess, with good recovery, similar to our recipient [2]. Other reported long term complications, included bleeding [2], haematoma [2], cholecystitis [2], mild graft rejection [5] and minor myocardial events [4]. Our case also experienced a myocardial event and splenic infarct but has recovered subsequently.
The ethical implications of transplantation in potential candidates with HIV must be considered. Simultaneous pancreas kidney transplantation is the treatment of choice for most patients with type 1 diabetes mellitus and ESKD because it saves lives, improves the quality of life and is cost-effective [9]. Recently, the advent of antiretroviral therapy, HIV positive patients with concurrent ESKD are expected to have similar expected graft survival as non-HIV patients [10]. However, the proposals to transplant HIV positive patients have also raised several ethical concerns. Apart from the interactions between antiviral agents and immunosuppression, the increased risk of acute rejection observed in HIV transplant recipients also poses major challenges balancing the dose and types of immunosuppression use and the inherent risk of opportunistic infections associated with immunosuppression such as T cell depleting agents for the management of acute rejection.
Nonetheless, this case supports that SPK transplantation is generally safe, with favourable short-term outcomes for young patients with T1DM, renal failure and HIV, if a tailored and planned program is used. Future studies and cases should expand on complex HIV patients with genotype mutations requiring transplantation.
References
- Miro JM, Ricart MJ, Trullas JC, Cofan F, Cervera C (2010) Simultaneous pancreas-kidney transplantation in HIV-infected patients: A case report and literature review. Transpl P 42: 3887-3891.
- Grossi PA, Righi E, Dalla Gasperina D, Donati D, Tozzi M (2012) Report of four simultaneous pancreas-kidney transplants in HIV positive recipients with favourable outcomes. Am J Transplant 2: 1039-1045.
- Akhtar MZ, Patel N, Devaney A, Sinha S, Shankar S, et al (2011) Simultaneous pancreas-kidney transplantation in the HIV-positive patient. Tranpl P 43: 3093-3904.
- Toso C, Berney T, Oberholzer J, Chave J, Martin P, et al (2003) Kidney pancreas transplantation in a long term non progressor HIV infected recipient. Am J Transplant 3: 631-633.
- Genzini T, Noujaim HM, Mota LT, Crescentini F, Antunes I, et al (2010) Simultaneous pancreas-kidney transplantation in human immunodeficiency virus-positive recipient: A case report. Transpl P 42: 591-593.
- The British Transplantation Society (2015) UK guidelines for kidney and pancreas transplantation in patients with HIV. National Health Service.
- Primeggia J, Timpone JG, Kumar PN (2013) Pharmacologic issues of antiretroviral agents and immunosuppressive regimens in HIV-infected solid organ transplant recipients. Infect Dis Clin N Am 27: 473-486.
- Baisi A, Nava F, Baisi B, Rubbiani E, Guaraldi G, et al (2016) Kidney transplantation in HIV infected recipients: Therapeutic strategy and outcomes in monocentric experience. Transpl P 48: 333-336.
- Wai PY and Sollinger HW (2011) Long term outcomes after simultaneous pancreas-kidney transplant. Curr Opin Organ Tran 16: 128-134.
- Stock PG, Barin B, Murphy B (2010) Outcomes of kidney transplantation in HIV-infected recipients. N Engl J Med 363: 2004-2014.

