Keywords
Childhood obesity; Healthy habits; Education; School based programs; School-nursing
Background
The prevalence of overweight and obese children and adolescents is at an alarming all-time high. It is currently estimated in The United States that 8% of children aged 2-5 years, 18% of children aged 6-11 year, and 21% of adolescents aged 12-19 years are obese [1]. Obesity at an early age can be indicative of lifelong health complications such as: diabetes, high cholesterol, high blood pressure, joint and muscular problems, gastro-esophageal disease, gallstones, fatty liver disease, cardiovascular disease, and psychological and social problems [2-7].
Furthermore, research indicates that children who are overweight or obese have a higher probability of becoming overweight later in life [8,9]. Research has shown that poor dietary habits, excessive screen time, and inadequate physical activity is directly associated with obesity [10]. Poor eating habits and a lack of physical activity are being seen at a younger age in today’s society. An approximated 678,000 deaths occur each year in the United States as a result of obesity-related diseases [11]. Recent data shows that approximately only thirty percent of children are following the standard national guidelines, put forth by the American Heart Association or the American Academy of Pediatrics (AAP), for recommended dietary servings/nutrition or daily physical activity [11-13]. The United States Department of Health and Human Resources recommends that children and adolescents participate in a total of 60 minutes of moderate to vigorous daily physical activity [11]. Therefore, in order to reverse the trend of obesity; interventions must be aimed at increasing physical activity and improving dietary habits. However, given the accelerating trajectory of obese children and adolescents there is a shortage of available programs and interventions. The shortage of available programs is due to a combination of several factors that include: the rapidly growing rate of children/adolescents who are overweight or obese, financial challenges of establishing/sustaining programs that can last for several years, and the number of programs that are available that have shown with proven statistical results to have led to significant decreases in weight [14].
The purpose of this study was to implement a three month school based program (Alex Chan and his balanced body bands) aimed at developing healthy habits in elementary aged students. The specific aims were to: a.) increase daily servings of: fruit, vegetables, dairy, and protein; b.) increase daily physical activity, c.) decrease daily screen time, and d.) increase daily number of kind gestures and communication (regarding health/fitness) between child and parent This pilot study was the first study to implement Alex Chan and his balanced body bands as a schoolbased intervention.
Review of the Literature
The focus of this review was to examine the literature on the effectiveness of published studies on school-based interventions. The following key words were utilized singly or in various combinations, and inputted into journal search engines (PubMed, CINAHL, Medline, and Google Scholar): pediatric obesity, childhood obesity, causes, diet, nutrition, physical activity, sedentary behavior, school, school-based programs, causes, associations, and interventions.
School Based Interventions
Extensive research has been conducted to assess the success of school-based interventions. Brown and Summerbell conducted a systemic review of school-based interventions and their outcomes on obesity reduction. The researchers included 38 studies in their analysis. Three of the 38 studies utilized a dietary intervention to reduce BMI. Fifteen studies implemented an intervention based on increasing physical fitness. The remaining twenty studies incorporated a mixed intervention program of nutrition, fitness, and reducing sedentary activities. Results of the systemic review revealed: 33% of the dietary, 33% of the physical fitness, and 45% of the mixed school-based interventions demonstrated statistically significant decreases in BMI post implementation [15].
Additionally, Kropski et al. preformed a systemic review of 14 studies to assess the effectiveness of school-based obesity reduction programs. 85% of the programs had significant positive changes in at least one core measure. Core measures were identified as: nutrition/diet, physical activity, or sedentary behavior. Additionally, the researchers observed that the home environment played a large role in the overall effectiveness of these programs. This is largely due to the role of behavior modeling between the parent and the child. Therefore, it is recommended that school-based programs include both a school and home component for maximum successfulness [16].
In further support, researchers Jang et al. conducted a systematic review to evaluate intervention programs that target parents as a method of decrease childhood obesity. Interestingly, these researchers discovered that programs targeting the parents as the intervention population led to more significant changes in childhood obesity than those programs targeting children alone or in combination with their child. Parental involvement has emerged as a key element in effective childhood obesity interventions. Parents play a major role in establishing the health behaviors of their children through modeling of lifestyle habits, parental control over child’s eating patterns, and accessibility and availability of various food types [17].
Evans et al. completed a meta- analysis of 21 studies. The focus of this meta-analysis was on various school-based interventions that focused on improving the daily fruit and vegetable consumption in children ages 5 to 12 years of age. The researchers found that school-based interventions were successful in increasing daily servings of fruit by 0.25 portions (95% CI, 0.06, 0.43 portions). However, there was no statistically significant increase in daily servings of vegetables [18].
Recent randomized control studies have shown that schoolbased programs that implemented educational sessions as a means to improve the participant’s knowledge on healthy eating/nutrition and physical activity have been successful in creating significant changes in decreasing sedentary behaviors, improving dietary consumption, and decreasing BMI [19-21].
On the contrary, Harris et al. conducted a meta-analysis to investigate school-based programs that utilized physical activity interventions. Their review consisted of 18 different studies which involved over 18,000 children and adolescents. These results revealed that the physical activity interventions lead to no statistically significant changes in BMI [22].
In summary, there has been extensive research conducted on school-based programs and their effects on obesity reduction in children and adolescents. The results have been mixed with some programs leading to significant changes in: BMI, diet, screen time usage, and physical activity. Whereas other studies have found no significant changes. What research has shown, is that programs that implement multiple components of health (physical fitness, diet, reducing sedentary behavior, etc.) are more successful than programs that only focus on one component [15,16]. Additionally, programs are more successful if they incorporate an intervention that can be integrated within both the school and the home environment, as children and adolescents are more likely to engage in behavior changes when the behavior is being modeled by their parent/guardian [16,17]. Therefore, based on this evidence, additional efforts should be made to collaborate alongside school educators to promote additional school-based obesity prevention interventions. These interventions should include multiple components of health and be integrated within the home environment as well.
Methods
Intervention
Alex Chan and his balanced body bands was designed and created by Mommies Mission. Mommies Mission is a company that was started by two local Midwestern moms with the goal of promoting healthy lifestyles to children and adolescents. The intervention bundle included: an illustrated story book, 21 wrist bands, a sticker shield, access to a mobile application, and participation in educational rallies. The story book, Alex Chan and his balanced body bands, highlights the importance of establishing healthy habits to help fight off obesity. In the book, Alex Chan, a racially neutral superhero, shares his story on how he earned his super powers. The story book describes how children can also become super heroes as they gain super powers by wearing the 21 balanced body bands. These wrist bands provided a visual reminder to children of healthy habits (e.g. eating three servings of fruit, engaging in physical activity, being kind, etc.). At the start of the day, the child places all of the wrist bands on his/her left wrist. After they complete a “habit” they move the wrist band to his/her right wrist. The goal was for the child to complete all 21 habits and successfully move all the bands to his/her right wrist. After completing all 21 habits they have earned their super powers for the day and are awarded a sticker for the sticker shield. The sticker shield has 21 spots to reinforce the premise that after 21 consecutive days of completing a behavior a new habit is formed.
This belief originated from the 1960s, by a plastic surgeon who later became a psychologist, Dr. Maxwell Maltz. Dr. Maltz had done extensive research and conducted numerous studies that revealed recent amputees needed approximately 21 days to overcome phantom limb pain. Since then much additional research has been conducted to further strengthen this long held belief [23].
The mobile application provided an electronic tool for tracking the participant’s prescribed activities in the program. The participant logged on the mobile application and tracked their daily habits. A parent/guardian was required to confirm the child’s completion log which encouraged daily communication regarding healthy habits between the child and parent/guardian. The participant’s progress on the mobile application provided validation of his/her participation in the program. Educational rallies were held at the school. During these rallies the children received additional education on the importance of eating healthy/nutrition, physical fitness, and kindness. Incentives were awarded numerous times (two weeks, one month, two months, and three months) throughout the program, during the rallies, to participating children to reward their active engagement/ completion in this program. The incentives that were awarded included: jump ropes, water bottles, Frisbees, and backpacks. These incentives were chosen specifically as they help encourage increased physical activity. Additionally, at the final assembly all children who participated for all three months were placed into a larger prize drawing. These prizes included: Razor scooters, outdoor balls, volleyball net/set, etc. (Figure 1).
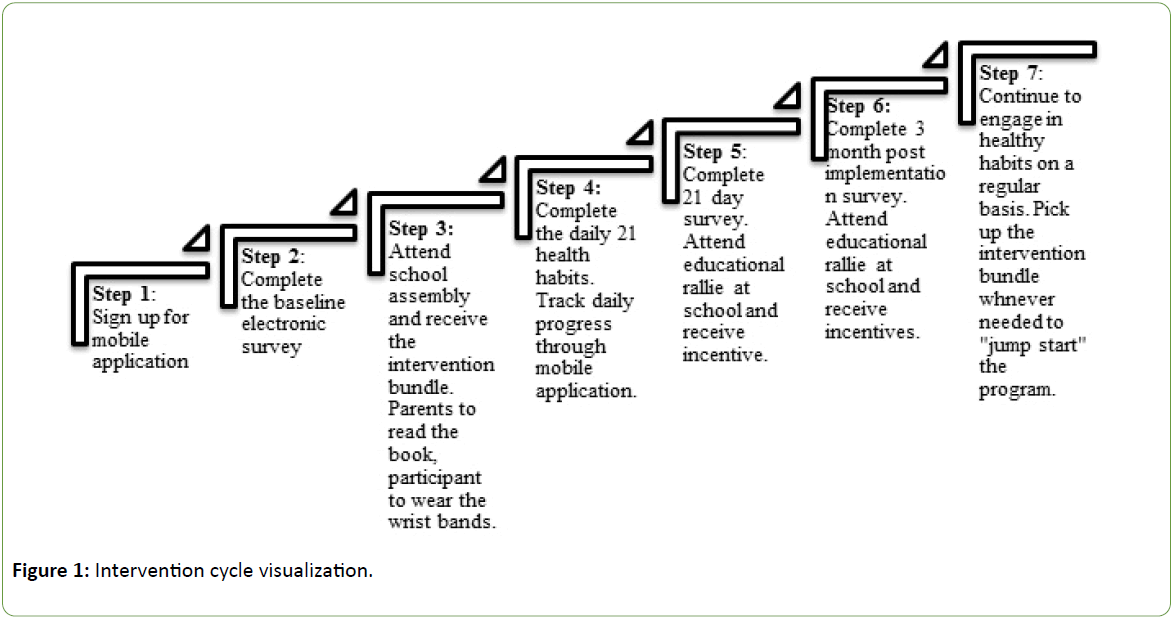
Figure 1: Intervention cycle visualization.
Design
This was a pilot program of school-aged children to determine the effectiveness of the Alex Chan and his balanced band body program intervention. The approach utilized for measuring significant changes in healthy habits, as specifically outline by the aims, was analyzed through a pre-and post-survey design. Participation in the program was verified through tracking on a mobile application. The program was three months in duration and was conducted from September to December of 2015. Creighton University IRB approved the study.
Population
School selection was limited to elementary parochial schools within a particular county as designated based on requirements from the Preventing Childhood Obesity Community Grant. Numerous parochial schools in the assigned county were contacted and interviewed based on their willingness to participate. The final school selected was based on a large potential sample size, location within the appropriate county, and voluntary participation within the needed time constraints. This school was a large predominately white, English speaking, Midwestern parochial school. Children and their associated parents/guardians from kindergarten to fifth grade were invited to participate (N=515 parent/child dyads). All students/families who wanted to participate were enrolled. There was no exclusion criterion.
Procedures
Prior to the start of the school year, an educational meeting was held with the principal, school nurse, and the teachers. There the researchers introduced The Balanced Body Band Program to staff. A brief introductory video was shown describing the intervention and its components. Each staff member was able to visualize an intervention bundle. Following the meeting, the principal e-mailed all of the parents, (of children from kindergarten to fifth grade), and informed them of this free program that was available to their child. The e-mail included a handout attachment describing the program as well as a link to the website for additional information. Prior to the start of the school year each family is required to attend the back to school meeting. At the meeting, I along with the creators of this program, were at the school handing out flyers for the program. For interested families, we assisted with registration on the mobile application and completion of the baseline survey. All invited children (N=515) received the intervention bundle at the first school rally. Consent for participation in this program was accepted, through the completion of the survey and enrollment in the mobile tracking application.
Measures
Outcome variables that were evaluated included measurable changes: in a.) daily servings of fruit, vegetables, dairy, protein; b.) increased daily participation in physical activity; c.) decreased daily screen time; d.) increased daily numbers of kind gestures and communication between child and parent (on healthy habits). The outcome variables were assessed and measured through the survey responses.
Instrument/Data collection
The survey utilized was created solely for the purpose of this program. The survey questions were created by myself and were verified by a statistician at Creighton University to be deemed reliable and valid. The survey was generated and accessed electronically through an internet site (Qualtrics). The first four survey questions (Table 1) were used to gather participant and demographic information. The remaining question (Table 1: #5-13, Table 2: #3-16) were used to gather information on the participant’s lifestyle and healthy habits. The survey questions were assessed to have a satisfactory Flesch-Kincaid Grade Level of 9.4 and Flesch Reading Ease score of 56.4. Prior to use, the survey was completed by numerous “blinded” adults to ensure proper comprehension of each question. A statistician confirmed the validity of each question and its correlation for future statistical analysis.
| S. No. |
Survey Questions |
| 1 |
Name (First and Last) and school grade of child participating in the Balanced Body Bands Program |
| 2 |
Name and email address of parent filling out the survey |
| 3 |
Child’s ethnicity origin (race) |
| 4 |
Parent’s highest level of school (degree) completed, if currently enrolled, highest level of degree received |
| 5 |
Are you concerned with your child’s current level of physical activity? |
| 6 |
On a typical day, outside of school, about how much time does your child spend doing some type of physical activity? |
| 7 |
On a typical day, how much time does your child spend watching television, playing video games, or using the computer (other than for homework)? |
| 8 |
Overall, how would you rate your child’s understanding and knowledge of healthy habits? |
| 9 |
For the following (sugary/processed foods, fruits, vegetables, protein, dairy/milk, and water) do you think your child needs to eat/drink more, eat/drink less, or is eating/drinking the correct amount? |
| 10 |
On a typical day, how many servings of the following (fruit, vegetables, protein, dairy) does your child consume? |
| 11 |
Rate your satisfaction as dissatisfied, neutral, or satisfied with the following: (level of kindness/respect your child shows you, their siblings, other family/friends, and time spent in prayer/blessings) |
| 12 |
Do you and your child talk about healthy habits/lifestyles on a typical day? |
| 13 |
How many minutes on a typical day, do you and your child spend in communication regarding what constitutes a healthy habit/lifestyle? |
Table 1: Baseline survey questions.
| S. No. |
Survey Questions |
| 1 |
Name (First and Last) and school grade of child participating in the Balanced Body Bands Program |
| 2 |
Name and email address of parent filling out the survey |
| 3 |
Are you concerned with your child’s current level of physical activity? |
| 4 |
On a typical day, outside of school, about how much time does your child spend doing some type of physical activity? |
| 5 |
On a typical day, how much time does your child spend watching television, playing video games, or using the computer (other than for homework)? |
| 6 |
Overall, how would you rate your child’s understanding and knowledge of healthy habits? |
| 7 |
For the following (sugary/processed foods, fruits, vegetables, protein, dairy/milk, and water) do you think your child needs to eat/drink more, eat/drink less, or is eating/drinking the correct amount? |
| 8 |
On a typical day, how many servings of the following (fruit, vegetables, protein, and dairy) does your child consume? |
| 9 |
Rate your satisfaction as dissatisfied, neutral, or satisfied with the following: (level of kindness/respect your child shows you, their siblings, other family/friends, and time spent in prayer/blessings) |
| 10 |
Do you and your child talk about healthy habits/lifestyles on a typical day? |
| 11 |
How many minutes on a typical day, do you and your child spend in communication regarding what constitutes a healthy habit/lifestyle? |
| 12 |
Have you seen a positive change in your child’s healthy habits since beginning the Balanced Body Bands program? |
| 13 |
How would you describe your child’s interest in their health since starting the program? |
| 14 |
How would you describe your child’s eating habits since starting the program? |
| 15 |
How would you describe your child’s level of activity and fitness since starting the program? |
| 16 |
How would you describe your child’s level of kindness/level of respect since starting the program? |
| 17 |
If you would please take a moment to give us some feedback about the program |
Table 2: One and three month survey questions.
Data collection was obtained through survey responses and verification of tracking on the mobile application. The surveys were completed by the participant’s parent/guardian three times during the intervention cycle (baseline, one month, and three month). Data obtained from the surveys were exported, coded, and various statistical analyses were utilized. These analyses were conducted at set intervals which ranged from baseline to 1 month, 1 month to 3 months, and from baseline to 3 months. In order to assess measureable changes in dietary habits (Table 1 survey question #9-10) Bowker’s Test of Symmetry was utilized. To assess measurable change in physical activity, screen time, and daily communication with parent (Table 1 survey questions 6, 7 and 13) Paired T-Tests were conducted. McNemar’s Test of Symmetry was ran to assess measurable changes in levels of kindness and basic understanding of healthy habits (Table 1 survey questions 5, 8 and 11). Change was deemed as significant based on a set p value: <0.05
Results
The invited sample included 515 students. At baseline 284 participants had completed the survey. 82 participants completed the first month cycle. Of the original participants (N=284), 30 completed all three months yielding a response rate of 12.6% (Figure 2).
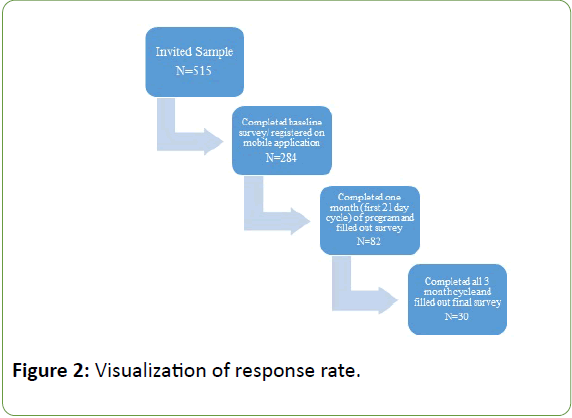
Figure 2: Visualization of response rate.
Demographic distributions revealed the average participant was 7 years of age, white, and originated from a family with a high level of parental education. (For complete demographic results see Table 3)
| Gender |
Female: 45% |
| Male: 55% |
| Age |
Range from 4-10 years of age |
| Mean age: 7.14 |
| School Grade |
K: 18% |
| 1st: 27% |
| 2nd: 20% |
| 3rd: 16% |
| 4th: 16% |
| 5th: 2% |
| Race/Ethnicity |
White: 93% |
| Asian/Pacific Islander: 2% |
| Hispanic/Latino: 3% |
| Prefer to leave blank: 2% |
| Parental Education/Degree |
High School/GED: 2% |
| Associate: 2% |
| Some college/no degree: 6% |
| Bachelor: 46% |
| Master: 24% |
| Doctorate: 16% |
| Professional: 4% |
Table 3: Demographic Distribution of Final Sample (N=30).
Regarding dietary habits, there was a statistically significant increase in the participant’s daily servings of vegetables (p=0.015) (Figure 3), protein (p=0.016) (Figure 4), and dairy (p=0.019) (Figure 5) between baseline and one month. However, the results were not seen in duration past one month. Findings supported a statistically significant decrease in individual’s usage of screen time. After three months, active participants were engaging in screen time usage 20.9 minutes less (p=0.000) (Figure 6) when compared to baseline. There were no significant changes post implementation in the following: increases in daily servings of fruit at one or three months (p=0.265 and p=0.986), increases in physical activity at one or three months (p=0.303 and p=0.304), increases in daily kind gestures (p=0.317), or increases in daily communication with parents regarding healthy habits (p=0.272).
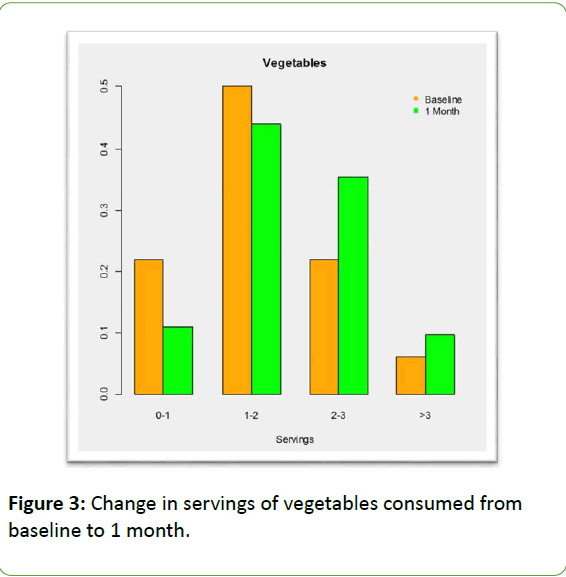
Figure 3: Change in servings of vegetables consumed from baseline to 1 month.
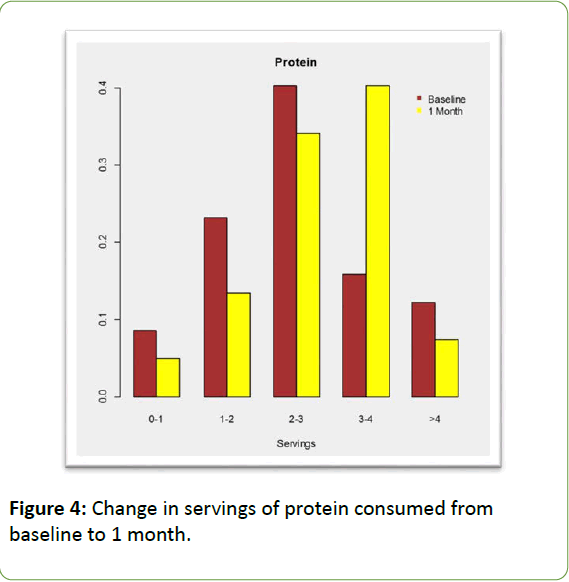
Figure 4: Change in servings of protein consumed from baseline to 1 month.
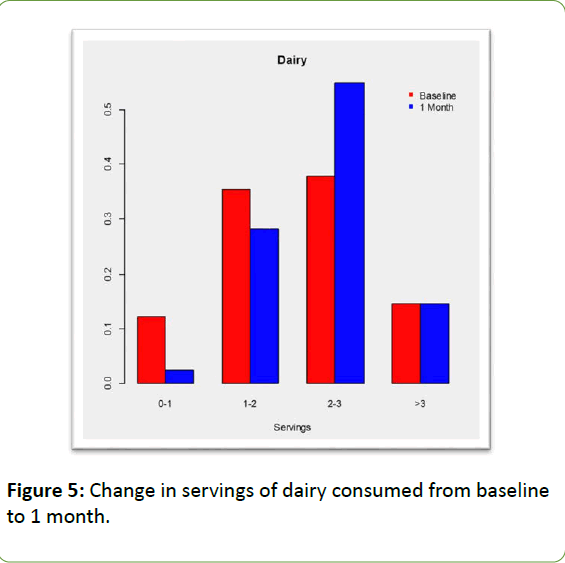
Figure 5: Change in servings of dairy consumed from baseline to 1 month.
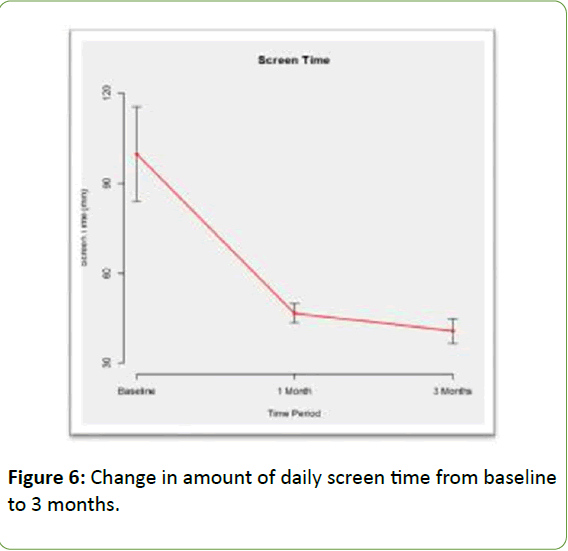
Figure 6: ChangeChange in amount of daily screen time from baseline to 3 months.
Overall, 82% of participants were satisfied with the program and its results. Furthermore, 86% of the participants’ parents felt that this program was effective in motivating their child to develop healthier habits. Feedback responses from the survey were examined. Of the 30 participants, who completed all three months; 43% of them took the time to leave comments regarding their child’s experience with the program. Responses were read separately by two different researchers with qualitative experience and coded for common themes. The following themes were identified: awareness, communication, and healthy choices. The following are two examples of feedback that were included: “Since starting the program, my child is more aware of the food she needs to eat to stay healthy. She also has become more physically active.” "We have been doing all activities every day now. He loves talking about healthy choices and reading food labels. We work on finding new activities to stay active and keep it fun."
Limitations
This study utilized voluntary participants from one parochial elementary school. Given the limited response rate (12.6%), from a single site, it is difficult to generalize these results. A questionnaire was sent to participants’ parents who enrolled at baseline and did not complete the three month program (N=254) to assess the rationale for drop out. The majority of responses indicated technical complications in navigating the mobile application as the main reason for drop out. Secondly, parents felt that the start of the school year was a busy time and did not feel there was enough time each day to go in and log their child’s daily progress electronically.
In addition the program was of short duration and did not utilize a control group to test the effectiveness of the program. Lastly, the school demographics showed a lack of diversity of ethnicity and socioeconomic status. Similar population demographics have influenced the findings, as those originating from higher economic status are generally able to afford healthier options with regards to diet and lifestyle habits. To further evaluate the effectiveness of this program, additional studies of longer duration should be conducted in a variety of different school settings.
Conclusion/Implication for School Nursing Practice
Alex Chan and his balanced body bands program was effective in helping children establish healthier habits as seen through changes in lifestyle habits. This program provided a limited number of children and their families (N=30) with general knowledge in order to maintain a healthy and balanced lifestyle. Being a pilot program, there were several lessons learned. First, the program was implemented at the start of the school year which is known to be a busy time for families and school staff. Secondly, participation in the program required verification of tracking on a mobile application, which leads to significant technological difficulties. Thirdly, the program required daily parental involvement (completion of mobile application), which lead to numerous parental questions. In moving forward, to further assess the effectiveness of this program, it would be recommended to implement this program later in the school term. Additionally, researchers should provide additional instructions (handout, video tutorial) for parents on how to properly navigate the mobile application. Moreover, researchers should invite parents to participate in the rallies throughout the program to further support/encourage their involvement in this program. Lastly, new research and data shows that health habits are actually formed after 66 days versus the previous held belief of 21 days [24]. Therefore, the program cycle duration should have been for at least 10 weeks to ensure adequate time was allowed for habit formation.
Implication for School Nursing Practice
Schools are an ideal location for the implementation of costeffective and sustainable interventions/programs aimed at reducing childhood obesity. Schools provide a location where a large number of children can be addressed at once. Furthermore, children spend a large majority of their waking hours in school, and thus would be exposed to interventions initiated within this setting. Lastly, school-based interventions can easily be implemented through mandated changes in school policy/curriculum. School nurses are often considered the health experts within the school and thus play an integral role within obesity prevention programs.
Based on the results of the Alex Chan and his balanced body bands program, several implications can be made. Currently, the participating school’s curriculum only offers a health class for fourth graders. Based on the survey data/responses generated, parents felt their child’s understanding of health was poor. Additionally, parent’s responded they were concerned with their child’s current level of physical activity. The school nurse can help advocate to school administrators for increased nutrition/ physical activity education or courses. Another implication is to involve the school nurse in the implementation of the program. They could have a larger role such as helping with the educational rallies which may help generate a higher participation response within the children. Lastly, the school nurse can serve as a contact person at the school who works as a liaison between the participants (and their parent) and the researchers. In conclusion, collaboration between the school nurse, educators, administration, and the students’ families is the key building block for promoting strong and sustainable programs.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this brief report.
Funding
The author(s) disclosed receipt of the following finical support for the research, authorship, and/or publication of this article: This pilot program was funded by Children’s Hospital and Medical Center (Omaha, NE) with the Preventing Childhood Obesity Community Grant Award.
References
- Center for disease control and prevention (2014) Overweight and Obesity: Data and Statistics.
- Adams A, Kessler J, Deramerian K, Smith N, Black M, et al. (2013) Associations between childhood obesity and upper and lower extremity injuries: Injury Prevention. J Int Soc Child Adolescent Inj Prev 19: 191-197.
- Castetbon K, Andreyeva T (2012) Obesity and motor skills among 4 to 6-year-old children in the United States: Nationally-representative surveys. BMC Pediatrics, 1228.
- Center for disease control and prevention (2012) Childhood obesity causes and consequences.
- Chrostowska M, Szyndler A, Paczwa P, Narkiewicz K (2011) Impact of abdominal obesity on the frequency of hypertension and cardiovascular disease in Poland: Results from the IDEA study (international day for the evaluation of abdominal obesity). Blood Press 20:145-152.
- Halfon N, Larson K, Slusser W (2013) Associations between obesity and comorbid mental health, developmental and physical health conditions in a nationally representative sample of United States children aged 10 to 17. Acad Pediatr 13: 6-13.
- Jarvandi S, Davidson N, Jeffe D, Schootman M (2012). Influence of lifestyle factors on inflammation in men and women with type 2 diabetes: Results from the National Health and Nutrition Examination Survey, 1999-2004. Ann Behav Medicine 44: 399-407.
- Merten M (2010) Weight status continuity and change from adolescence to young adulthood: Examining disease and health risk conditions. Obes Silver Spring Md 18:1423-1428.
- Ludington-Hoe S, Gittner L, Haller H (2013) A pilot study: Does obesity begin in the first year of life? Clinic Pediatr, 52: 507-512.
- Taveras E, Gillman M., Kleinman, K, Rick-Edwards J, Rifas-Shiman S (2010) Racial/ethnic differences in early-life risk factors for childhood obesity. Am Acad Pediatr J 125: 686-695.
- Flores G, Lin H (2013) Factors predicting overweight in US kindergartners. Am J Clinic Nutr 97: 1178-1187.
- United States Department of Agriculture (2015) Food consumption and nutrient intakes.
- American Academy of Child and Adolescent Psychiatry (2014) Obesity in children and teens.
- Reedy J, Krebs-Smith S (2010) Dietary sources of energy, solid fats, and added sugars among children and adolescents in the United States. J Am Diet Assoc 110: 1477-1484.
- Karnik S, Kanekar A (2012) Childhood obesity: A public health crisis. Int J Prevent Med 3: 1-7.
- Brown T, Summerbell C (2009) Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: An update to the obesity guidance produced by the National Institute for Health and Clinical Excellence. Obes Rev 10:110-141.
- Kropski J, Keckly P, Jensen G (2008) School-based obesity prevention programs: An evidence based review. Obes J 16: 1009-1018.
- Jang M, Chao A, Whittemore R (2015) Evaluating intervention programs targeting parents to manage childhood overweight and obesity: A systematic review using the re-aim framework. J Pediatr Nursing 30: 877-887.
- Evans C, Christian M, Cleghorn C, Greenwood D, Cade J (2012) Systemic review and meta-analysis of school-based interventions to improve daily fruit and vegetable intake in children aged 5 to 12 y. Am J Clinic Nutr 96: 889-901.
- Llargues E, Franco R, Recasens A, Nadal A, Vila M, et al. (2011) Assessments of school-based intervention in eating habits and physical activity in school children: The Avall Study. J Epidemiol Commun Health 65: 896-901.
- Neumark-Sztainer D, Friend S, Flattum C, Hanna P, Story M, et al. (2010) New moves-preventing weight related problems in adolescent girls; A group randomized study. Am J Preventive Med 39: 421-432.
- Sacchetti R, Dallolio L, Musti M, Guberti E, Garulli A, et al. (2015) Effects of a school based intervention to promote healthy habits in children 8-11 years old, living in the Iowland area of Bolgona Local Health Unit. Ann Ig 27: 432-446.
- Harris K, Kuramoto L, Schulzer M, Retallack J (2009) Effects of school-based physical activity interventions on body mass index in children: A meta-analysis. Can Med Assoc J 180: 719-726.
- Lally P, Gardner B (2013) Promoting habit formation. J Health Psychol Rev 7: 137-158.

