Che-Wei Wang1* and Chin-Fang Chang2,3,4
1Department of Otorhinolaryngology, Head and Neck Surgery, Changhua Christian Hospital, Changhua, Taiwan
2Department of Otorhinolaryngology, Head and Neck Surgery, Jen-Ai Hospital, Taichung, Taiwan
3School of Medicine, Chung Shan Medical University, Taichung, Taiwan
4Central Taiwan University of Science and Technology, Taichung, Taiwan
Corresponding Author:
Chin-Fang Chang
Department of Otorhinolaryngology, Head and Neck Surgery, Jen-Ai Hospital, #483, Dongrong Rd, Dali Dist, Taichung City 412, Taiwan.
Tel: +886-4-2481-9900
E-mail: benglung@hotmail.com
Received date: May 12, 2016; Accepted date: June 13, 2016; Published date: June 16, 2016
Citation: Wang CW, Chang CF. The Association of Secondary Tonsillar Tuberculosis with Asymptomatic Pulmonary Focus. J Infec Dis Treat. 2016, 2:1.
Introduction
Tuberculosis is one of the most serious infectious problems in the world. Tuberculosis of the oral cavity is uncommon and tonsillar tuberculosis is one of the extremely uncommon forms of extrapulmonary tuberculosis [1]. Oral cavity tuberculosis could be either primary or secondary [2]. In this report, we describe a rare case of tonsillar tuberculosis in a middle aged female with asymptomatic pulmonary focus. A detailed review of the literature on tonsillar tuberculosis is also included.
Case Report
A 44 year old lady came to our outpatient department on Oct. 30th, 2009 presented with a one month history of sore throat and right neck movable tender mass. No previous history of chronic cough or other symptoms was mentioned. On physical examination a movable mass about 2 × 2 cm with tenderness was noted over right neck, and oral examination showed a hard swelling mass on right palatine tonsil. The chest film showed no abnormality. The full blood count, urine analysis and serum chemistry studies were normal. The CT scan of the neck revealed normal appearance of the nasaophrynx, oropharynx, hypopharynx and larynx. There was no evidence of cervical metastatic lymphadenopathy. On suspicion of malignancy, an excision biopsy of right tonsillar mass was performed. Histopathology revealed granulomatous inflammatory lesion with caseation necrosis (Figure 1). The acidfast stain for mycobacteria and PAS stain for fungus are negative. The Masson's trichrome stain is negative. The smears and cultures of sputum were positive for acid-fast bacilli. Based on these findings of histological examination, pathological examination, and oral examination, a diagnosis of tonsillar tuberculosis was made. Therefore, antituberculous agents (Ethambutol 800 mg/ day, rifampicin 450 mg/day) were given without any side effect. The patient showed marked improvement in symptoms and became asymptomatic within two months. She is presently under follow-up to complete her prescribed regimen.
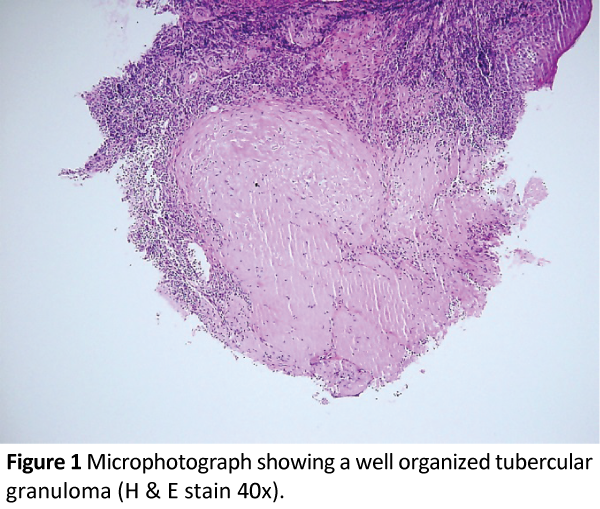
Figure 1: Microphotograph showing a well organized tubercular granuloma (H & E stain 40x).
Discussion
Tonsillar tuberculosis is a rare disease in developed countries. The upper respiratory tract is generally resistant to tuberculosis because saliva is thought to have an inhibitory effect on tubercle bacilli. The presence of saliva and saprohytes, the antagonism of the striated musculature, and the thickness of the protective epithelial layer are thought to have an inhibitory effect on tubercle bacilli. Tuberculosis of a tonsil can result from infection caused by contact with tubercle bacilli contaminated materials [3,4]. The site commonly involved is the tongue, followed by palate, gums and lips. In patients with oral or pharyngeal tuberculosis traumatic ulcers, aphthous ulcers, hematological disorders, actinomycosis, syphilis, midline granuloma, Wegner's disease and malignancy should always be kept in mind. Tuberculosis of the oral cavity has shown a decline in several parts of the world, and poor dental hygiene, dental extraction, periodontitis and leucoplakia are predisposing factors for primary oral tuberculosis.
The commonest local symptoms of tonsillar tuberculosis are hoarseness and difficulty in swallowing. Over one third of patients with cervical lymphadenitis can be observed on patients with tonsillar tuberculosis. Our patient had an obvious cervical lymphadenitis and her tonsil was hypertrophic, but on CT scan no obvious lyphadenopathy was noted. Diagnosis of tonsillar tuberculosis is based on histopathological findings and the identification of tubercle bacilli. In the present case, we can see typical tuberculosis finding of granulomatous inflammatory lesion with caseation necrosis that can help us make the diagnosis. Treatment is in the form of anti-tuberculosis therapy.
There is a rising incidence of tuberculosis not only the developing countries but also the developed ones. Some probable reasons may contribute to this resurgence of tuberculosis, such as the wide epidemic spread of human immunodeficiency virus (HIV), bad living and nutritional conditions, and the rising of mycobacterial strains resistant to the most available chemotherapeutic agents. The recent increase in cases with HIV infection has led to a resurgence of tuberculosis. Concomitant HIV infections may be present in 25% of patients with laryngeal tuberculosis. Our patient had no history of substances’ abuse and HIV testing was negative [5].
Although no pulmonary problem was observed on clinic and image study, the sputum culture acid fast stain showed positive. Also, the improvement of the symptoms after the administration of antituberculous agents confirmed the presence of pulmonary and laryngeal tuberculosis. Since most of tuberculosis of the oral cavity is secondary tuberculosis originating from pulmonary tuberculosis, [6] our case is thought to be a case of secondary tonsillar tuberculosis with primary pulmonary tuberculosis.
In summary, we have presented a rare case of tonsillar tuberculosis associated with asymptomatic pulmonary origin. Tonsillar tuberculosis should be considered as well as malignancy, when enlargement of the palatine tonsils is observed. A sore throat and or unexplained hoarseness should alert the clinician to the possibility of tuberculosis as a factor, not only developing countries but also the developed ones.
References
- Sutbeyaz Y, Ucuncu H, Murat Karasen R, Gundogdu C (2000) The association of secondary tonsillar and laryngeal tuberculosis: a case report and literature review. AurisNasus Larynx 27: 371-374.
- Weidman WN, Campbell HB (1939) Laryngeal tuberculosis. Am Rev Tuberc 40: 85-98.
- Verma A, Mann SBS, Radotra B (1989) Primary tuberculosis of the tongue. Ear Nose Throat J 68: 718-720.
- Brennan TF, Vrabec DR (1970) Tuberculosis of the oral mucosa Report of a case. Ann OtolRhinolLaryngol 79: 601-605.
- Sutbeyaz Y, Ucuncu H, Murat Karasen R, Gundogdu C (2000) The association of secondary tonsillar and laryngeal tuberculosis: a case report and literature review. AurisNasus Larynx 27: 371-374.
- Singh B, Balwally AN, Nash M, Har-El G, Lucente FE (1996) Laryngeal tuberculosisin HIV-infected patients: a difficult diagnosis. Laryngoscope 106: 1238-1240.
- Yamamoto K, Iwata F, Nakamura A, Iwashima Y, Miyaki T, et al. (2002) Tonsillar tuberculosis associated with pulmonary and laryngeal foci. Int med 41: 664-666.

