Özgür Gündüz1*, Deniz Öztürk Kara2, Pinar Atasoy3, Mehtap Kidir4 and Serkan Demirkan1
1Department of Dermatology and Venerology, University of Kirikkale, Turkey
2Department of Dermatology, Elazig Teaching Hospital, Turkey
3Department of Pathology, University of Kirikkale, Turkey
4Department of Dermatology, Dumlupinar University, Turkey
*Corresponding Author:
Özgür Gündüz
Department of Dermatology
University of Kirikkale
Yenisehir Mah. No: 14-71451
Yahsihan/Kirikkale, Turkey
Tel: +903182252485
Fax: +903182252484
E-mail: gunduzozgur@windowslive.com
Received date: March 31, 2016; Accepted date: April 25, 2016; Published date: April 30, 2016
Citation: Gündüz Ö, Kara DÖ, Atasoy P, et al. Tacrolimus-responsive lichen striatus. Clin Pediatr Dermatol. 2016, 2:2. Doi: 10.21767/2472-0143.100017
Keywords
Lichen striatus; Somatic mutation; Blaschko lines; Immune tolerance; Keratinocyte targeted T-cell mediated immune reaction; Calcineurin inhibitors
Introduction
Lichen striatus (LS) is a relatively uncommon, self-limited, linear dermatosis of unknown etiology that primarily affects children [1]. A linear eruption consisting of clustered, flat, pink-brown papules along Blaschko lines is its characteristic clinical feature. Histologic evaluation of skin biopsies suggest a T-lymphocyte mediated immune reaction against keratinocytes. Diagnosis is established on the distinctive clinical appearance and distribution pattern of the cutaneous lesions. Due to the self-limited nature of the disease, treatment is not mandatory, unless there is significant pruritus or psychological discomfort. Various therapeutic approaches have been tried for the treatment of LS. Rapid healing without cutaneous sequela like atrophy or hypopigmentation was observed in the patient treated with tacrolimus.
Case Report
Case 1
A 6-year old girl with a 1-month history of linear, erythematous rash extending from her right shoulder (Figure 1a) to the dorsum of proximal phalanxes of her third and fourth fingers on her right hand (Figure 2a) presented to our clinic. Physical examination revealed clustered, skin-colored papules in a linear arrangement. She had no relevant medical history and except the rash, she was in good general health. In histologic sections,focal keratosis and spongiosis in epidermis and a dermal lymphocytic infiltrate in perivascular and periadnexal regions and at the dermoepidermal junction was observed (Figure 1c). She was diagnosed with LS on the basis of clinical and histological findings and 0.03% tacrolimus ointment twice daily was started. After 12 weeks, all the cutaneous lesions were cleared (Figure 1b) and with the disapperance of cutaneous lesions, topical tacrolimus was stopped by the parents of the patient.. But 15-months later, the patient presented with evident longitidunal ridging and onycholysis on the radial halves of the fingernails of her right middle and ring fingers (on the distal end of the affected Blaschko line) (Figure 2b).
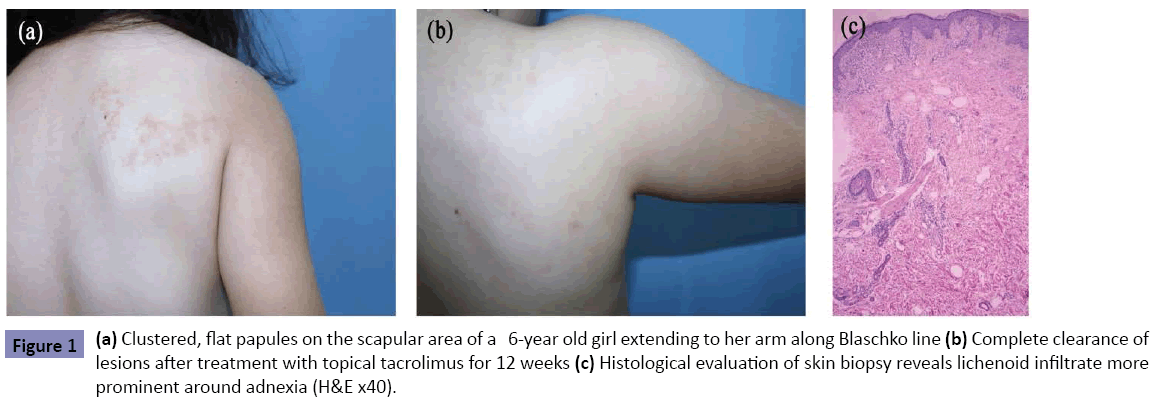
Figure 1: (a) Clustered, flat papules on the scapular area of a 6-year old girl extending to her arm along Blaschko line (b) Complete clearance of lesions after treatment with topical tacrolimus for 12 weeks (c) Histological evaluation of skin biopsy reveals lichenoid infiltrate more prominent around adnexia (H&E x40).
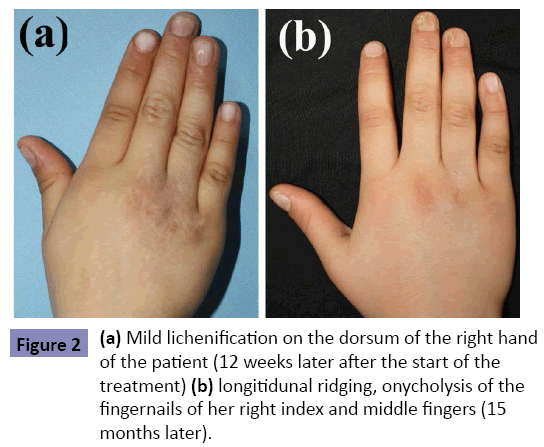
Figure 2: (a) Mild lichenification on the dorsum of the right hand of the patient (12 weeks later after the start of the treatment) (b) longitidunal ridging, onycholysis of the fingernails of her right index and middle fingers (15 months later).
Case 2
A 17-year old girl with 2-month history of linear, asymptomatic, erythematous papules extending from her left gluteal sulcus to the popliteal fossa presented our clinic (Figure 3a and 3b). Her medical history was noncontributory. LS was diagnosed on the basis of clinical and histopathological features (Figure 3e). 0.03% tacrolimus ointment was prescribed. This patient, then was lost to our follow-up. At her second visit 16 weeks later, she had dropped tacrolimus and instead, used mometasone furoate 0.1% ointment for 12 weeks. Active lesions among atrophic areas were observed (Figure 3c and 3d).
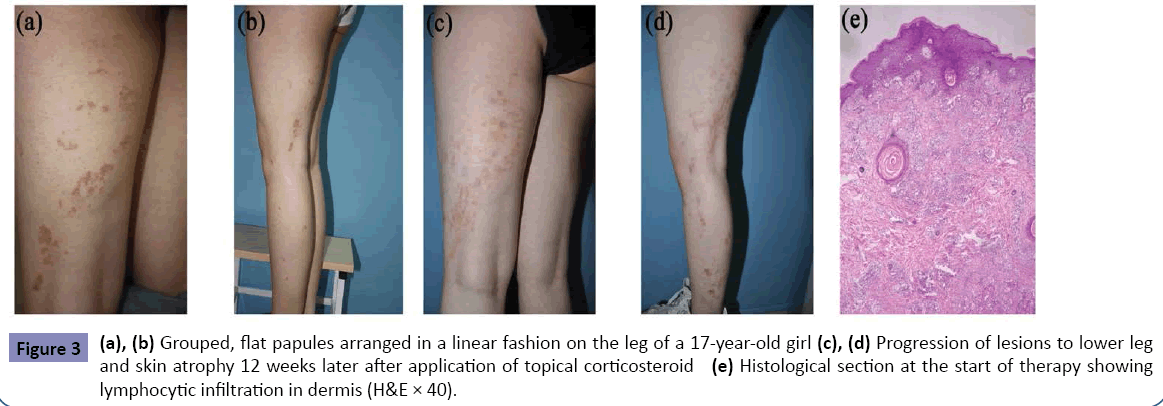
Figure 3: (a), (b) Grouped, flat papules arranged in a linear fashion on the leg of a 17-year-old girl (c), (d) Progression of lesions to lower leg and skin atrophy 12 weeks later after application of topical corticosteroid (e) Histological section at the start of therapy showing lymphocytic infiltration in dermis (H&E × 40).
Discussion
Lichen striatus (LS) is a benign skin disease with a self-limited course. LS usually manifests as erythematous or skin-colored milimetric papules following a Blaschko line. Skin biopsises usually show a lichenoid interface dermatitis, characterized by a dense inflammatory infiltrate (consisting predominantly of CD3+ lymphocytes) obscuring portions of dermoepidermal junction. CD8+ T-lymphocytes surrounding the necrotic keratinocytes and intraepidermal grouped Langerhans cells can be observed in the inflammatory infiltrate [2]. Although not pathognomonic, observation of lymphocytes surrounding the follicular epithelium and eccrine coils is a distinguishing feature for LS and may assist in differential diagnosis. Histo-pathological features may also mimick other inflammatory or neoplastic dermatoses, including mycosis fungoides [3]. The classic pattern of cutaneous lesions and histopathological features suggest a T-cell-mediated autoimmune response directed against a keratinocyte cell line with somatic mutation (somatic mosaicism) [1,2,4]. According to this theory, a possible causative factor like a viral infection [5,6] or cutaneous injury may disturb the immune tolerance to this divergent cell clone and trigger an autoimmune reaction, which may destroy the abberrant cell line and probably prevent the following relapses [1], but still, neither the mutations nor the exact trigger factors are identified. In 1990, a clinical entity with similar skin lesions, “Blaschkitis”, was described [7]. Since then, there has been much debate over whether “Lichen striatus” and “Blaschkitis” were seperate entities or not. Some reports define blaschkitis as a distinct disease emphasizing its truncal localization and more eczema-like histologic features [7,8] but other authors contradict this notion due to the similarity between the clinical features and clinical progress of LS and blaschkitis [9]. Other diseases, which should be included in the differential diagnosis are; inflammatory linear verrucous epidermal nevus (ILVEN), linear lichen planus, linear psoriasis and incontinentia pigmenti [10] (Table 1).
| Differrential Diagnosis for Lichen Striatus |
| Disease |
Clinical Presentation |
Biopsy |
| Lichen Striatus |
•Flat, scaly clustered papules following Blaschko lines
|
•Interphase dermatitis
• Sometimes psoriasiform pattern, mild acanthosis, perivascular, perifollicular lymphocytic infiltration |
| Blaschkitis |
•Continuous or interrupted papulovesicular eruption along the Blaschko lines.
•Frequently observed on trunk. |
•Spongiotic pattern |
| Linear Lichen Planus |
•Rare variant of lichen planus.
•Frequently seen in children.
•Pruritic, flat, violaceous, milimetric papules following a Blaschko line (not dermatomal) |
•Classic lichen planus histopathology.
•A band of lymphocytic infiltrate along the dermoepidermal junction.
•Epidermal acanthosis and hypergranulosis (wedge pattern)
•Necrotic keratinocytes (colloid bodies) in the epidermis and papillary dermis |
| Linear Psoriasis |
•Rare variant of psoriasis
•Unilateral erythematous flat papules or plaques with white scales following a Blaschko line |
•Classic psoriasiform pattern
•Epidermal hyperplasia, elongated retes
•Parakeratosis, hypogranulosis
•Neutrophils in the dermis (Munro’s microabscesses) |
| Incontinentia Pigmenti (Bloch-Sulzberger Syndrome) |
•an X-linked dominant neurocutaneous syndrome
•mutation in NF-κB essential modulator (NEMO) gene in chromosome Xq28
•lethal for males
•Early stages( in utero and infancy): Skin covered with bullous lesions (later verrucous leisons) distributed in a Blaschkoid pattern on trunk and extremities
•Late stages ( three to six months of age): Hyperpigmentation
•Second – third decade: hypopigmentation, atrophy
•Also observed; wooly hair, dental anomalies (conical teeth deformities), abnormalities of retinal vessels (ischemic optic neuropathy), seizures
|
•Vesiculo-bullous stage: eosinophilic spongiosis. Apoptotic keratinocytes and eosinophil containing vesicles in epidermis, eosinophils in dermis
•Verrucous stage: Epidermal acanthosis, hyperkeratosis, papillomatosis. Apoptotic keratinocytes in epidermis. Dermal perivascular lymphocytes. Scarce dermal eosinophils. Melanin incontinence
•Hyperpigmentation stage: Melanin incontinence, melanophages in dermis. Lack of epidermal hyperplasia
•Hypopigmentation stage: Epidermal atrophy, reduced number of melanocytes. Lack of melanin incontinence and other inflammatory cells (10). |
| Inflammatory linear verrucous epidermal nevus (ILVEN) |
•Rare variant of epidermal nevus
•Usually occurs in early childhood
•Unilateral, pruritic , erythematous, hyperkeratotic papules along the lines of Blaschko |
•Psoriasiform epidermal hyperplasia
•Alternating bands of para-and orthokeratosis
•Chronic inflammatory infiltrate in dermis |
Table 1: Differential diagnosis for Lichen Striatus.
Mean duration time for LS is reported to be about 9,5 months [4], but LS cases with active phases over 2-years have been described [11]. This protracted course may cause emotional distress, particularly when the disease manifests on the face or a visible part of the body, such as nails and these patients and their families may benefit from a therapeutic intervention. Due to the rarity of the disease, no established treatment guidelines are available, but there are anecdotal reports of successful treatments with topical calcineurin inhibitors (CI) [12-14], systemic corticosteroids [15] and photodynamic therapy [16]. Considering the previous reports [12-14], we prescribed topical tacrolimus twice daily for our patients and observed dramatical and rapid improvement in case 1. Cutaneous lesions were cleared in 12 weeks, a considerably short healing time when compared to reported mean duration time. Also, there weren’t any skin atrophy or hypopigmentation in this patient. The only negative outcome was the dystrophic nail changes. Nail damage was attributed to premature discontinuation of the treatment. The outcome with case 2 was worse. This non-compliant patient had still active lesions and also cutaneous atrophy due to prolonged use of topical steroids after 12 weeks, indicating the risk of inappropriate choice (and probably inappropriate use) of topical drugs for the treatment of LS.
Conclusion
No definitive conclusion can be reached with our two-case experience but, since LS is an uncommon disease, large case series to evaluate the treatment options are practically unavailable. Therefore case reports are the only references for the physicians treating LS patients. Although LS is a benign, self-limited disease, it may cause emotional stress in patients and parents, causing them to self-medicate, which, in turn, can have worse side-effects than LS. Also, LS can affect nails and cause permanent dystrophic changes, due to partial destruction of nail matrix.
Tacrolimus is an established immunosuppressant, which works by inhibiting calcineurin and preventing T cell activation, which is a constant feature of LS histopathology. Tacrolimus has also been found out to be as effective as potent topical corticosteroids and more potent than mild topical steroids in atopic dermatitis, in which activated cutaneous lymphocytes also play an important role [17]. Inhibitory effects of tacrolimus on lymphocytes and various case reports, including ours, [12-14] suggest that tacrolimus and probably the other CI may be a good therapeutic option for LS. Without the side-effects of topical steroids, topical CI seem to be also the safer choice. We also suggest that topical CI should applied on the periungual areas (under occlusion if possible) of the nails, which are on the affected Blaschko line to prevent a permanent nail damage.
References
- Patrizi A, Neri I, Fiorentini C, Bonci A, Ricci G (2004)Lichen striatus: clinical and laboratory features of 115 children.Pediatr Dermatol 21:197-204.
- Gianotti R, Restano L, Grimalt R, Berti E, Alessi E, et al. (1995) Lichenstriatus--a chameleon: an histopathological and immunohistological study of forty-one cases. J Cutan Pathol 22:18-22.
- Mascolo M, Russo D, Scalvenzi M, Di Lorenzo P, Cerroni L (2014) Lichenstriatus histopathologically mimicking mycosis fungoides. J Dtsch Dermatol Ges 12:1048-1050.
- Taieb A, Youbi AE, Grosshans E, Maleville J (1991) Lichen striatus: a blaschko-linear acquired inflammatory skin eruption. J Am Acad Dermatol 25: 637.
- Ishikawa M, Ohashi T, Yamamoto T (2014) Lichenstriatus following influenza infection. J Dermatol. 41:1133-1134.
- Kennedy D, Rogers M (1996) Lichen striatus. Pediatr Dermatol 13:95-99.
- Grosshans E, Marot L (1992) Blaschkite de l’adulte. Ann Dermatol Vénéréol 119:577.
- Katharina D, Katharina F (2011) Blaschkitis in children – a new entity? J Dtsch Dermatol Ges 9:48-49.
- Hofer T (2003) Lichen striatus in adults or ‘Adult Blaschkitis’? Dermatology207:89-92.
- Fraitag S, Rimella A, de Prost Y, Brousse N, Hadj-Rabia S, et al. (2009) Skin biopsy is helpful for the diagnosis of incontinentia pigmenti at late stage (IV): a series of 26 cutaneous biopsies. J Cutan Pathol 36:966-971.
- Feely MA, Silverberg NB (2014) Two cases of lichen striatus with prolonged active phases. Pediatr Dermatol 31:e67.
- Jo JH, Jang HS, Park HJ, Kim MB, Oh CK, et al. (2007) Early treatment of multiple and spreading lichen striatus with topical tacrolimus. J Am Acad Dermatol 57:904-05.
- Fujimoto N, Tajima S, Ishibashi A (2003) Facial lichen striatus: succesful treatment with tacrolimus ointment. Br J Dermatol 148:587-590.
- Campanati A, Brandozzi G, Giangiacomi M, Simonetti O, Marconi B, et al. (2008) Lichen striatus in adults and pimecrolimus: open, off-label clinical study. Int J Dermatol 47:732-736.
- Lee DY, Kim S, Kim CR, Kim HJ, Byun JY, et al. (2011) Lichen striatus in an adult treated by a short course of low-dose systemic steroid. J Dermatol 38:298-299.
- Park JY, Kim YC (2012) Lichen striatus succesfully treated with photodynamic therapy. Clin Exp Dermatol.
- Ashcroft DM, Dimmock P, Garside R, Stein K, Williams HC (2005) Efficacy and tolerability of topical pimecrolimus and tacrolimus in the treatment of atopic dermatitis: meta-analysis of randomised controlled trials. BMJ 330:516-524.

