Keywords
Autism; ASD; Behavioral therapy; PRT; Pivotal response treatment; Multiple cue responding; Stimulus over selectivity; Tunnel vision; Mental synthesis; Cognitive therapy; Language therapy; Early intervention; ABA
Introduction
The Centers for Disease Control (CDC) estimates that 1 in 68 children is affected by autism spectrum disorder (ASD), a neurological disorder that disrupts early development in cognition and communication, leading to impairment in cognitive and social functions, and difficulty in acquiring new adaptive behaviors. The CDC estimates that ASD affects a staggering 1 in 68 children [1], and approximately two thirds of children with ASD grow up to have a significant cognitive impairment [2]. There is broad scientific consensus that early and intensive behavioral intervention can result in sizeable gains in cognitive, communication, social, academic, and adaptive skills, and has the greatest chance of significantly improving outcomes, sometimes even resulting in a complete loss of diagnosis [3-5]. Accordingly, the American Academy of Pediatrics (AAP) recommends universal screening of 18- and 24-month-old children for ASD, and also that individuals diagnosed with ASD begin to receive no less than 25 hours per week of treatment within 60 days of identification [6]. Despite the AAP recommendation, two-thirds of US children on the autism spectrum under the age of 8 fail to get even the minimum recommended treatment [7] because of major problems with the availability, quality, and general funding for early intervention programs [8-10]. Since the AAP’s 2007 recommendation of universal, early screening, there has been a sharp increase in demand for ASD-related services (58% on average) [11]. According to a recent study, however, most states have reported an enormous shortage of ASD-trained personnel, including behavioral therapists (89%), speech-language pathologists (82%), and occupational therapists (79%) [11]. In many states children are getting less than 5 hours/week of service, and this immense shortage disproportionally affects African American and Latino children [11]. Families of newly diagnosed children often face lengthy waitlists for therapy, leaving children without treatment during the most critical, early period of development and parents without the guidance on how they can help. The failure to provide adequate early intervention services ends up costing society (USA) an estimated $126 billion per year [12]. The use of technology in the delivery of much needed therapy promises to be effective for shrinking the gap between the therapy that is recommended for children with ASD and the amount they receive. Recently, there has been a trend towards computer-based interventions which capitalize on the often-observed preference that children with ASD show for flat screen information [13-15] as well as evidence suggesting that tablets specifically have been a great learning tool for children on the spectrum [16,17]. However, since there is scant research on computer-based interventions for children with ASD, many questions remain to be answered: At what age are children diagnosed with ASD capable of being fully engaged with computer-based interventions? Can parents implement and administer computer-based therapy?
In order to answer these questions, we developed a tabletbased therapeutic application for children with ASD, which we call Mental Imagery Therapy for Autism (MITA) [18]. In this report, we describe data from a feasibility study of MITA that included 832 children with ASD who worked with the application for three to ten months. We discuss MITA usability, feasibility, fidelity of implementation and promise of outcomes. To our knowledge, this report is the first to study of tablet-based cognitive exercises administered to two-year-old toddlers with autism and it is also the largest study of an early parentadministered intervention tool to toddlers with autism.
MITA’s tasks and overall curriculum are grounded in some of the best scientifically supported and established, evidencebased therapies for ASD [19], drawing most heavily from Applied Behavioral Analysis (ABA) and Pivotal Response Training (PRT). MITA focuses on one of the four key, or “pivotal,” areas of development targeted by PRT that in turn affects a wide range of behaviors. MITA’s educational objective is to develop a child's ability to notice and respond to multiple cues presented simultaneously. To understand this ability, imagine that you are instructed to pick up a red crayon that is under the table. This may seem like a trivial task, but in order to accomplish it successfully, you need to notice three different features, or “cues,” of the object: its color (red), its shape (crayon) and its location (under the table). You must then mentally integrate all three pieces of information into a new mental image, a red crayon under the table, in order to take the correct action. The ability to integrate multiple cues is highly developed in individuals not afflicted by ASD well before the age of 6, but it is known to be a common challenge for children on the spectrum [20], resulting in a phenomenon called stimulus overselectivity, whereby an individual focuses on only one aspect of an object or environment while ignoring others [21-23]. When asked to pick up a red crayon under the table, a child with ASD may hyperattend to the cue "crayon" and ignore both its location and the fact that it should also be red, therefore picking up any available crayon. It is often said that individuals with ASD “can't see the forest for the trees”: they pay too much attention to specific parts, get lost in the details and miss the whole picture (or Gestalt). The consequences of attempting to navigate the world with an impaired ability to respond to multiple cues can be profound and can affect virtually every area of functioning [20]. However, using PRT to develop responsivity to multiple cues has been shown to reduce stimulus overselectivity and, most importantly, to lead to improvements in general learning [1,24]. In addition to developing a child’s ability to respond to multiple cues, MITA also aims to train receptive language, starting with simple vocabulary, and progressing towards higher forms of language, such as adjectives, verbs, pronouns, and syntax [25,26].
Methods
Subjects
MITA was made available for free at all major app stores in February 2016. Once the app was downloaded, the user was asked to register and provide demographic details, including the child’s diagnosis as well as month and year of birth (the exact birth date was not collected to maintain patient privacy). In addition, parents were required to complete questionnaires. The first questionnaire was administered approximately one month after the first use of MITA and once 100 puzzles had been completed. The subsequent questionnaires were administered at three month intervals. Parents were asked to complete questionnaires independently of a child’s actual use of MITA.
During the course of seven months, from February to September 2016, the app was registered 21,453 times. From this pool of potential study subjects we selected subjects based on the following three criteria:
1. The subject must have filled out at least two questionnaires at least three months apart: Since our application was available for free to the general public, we expected a large volume of downloads by people of widely ranging commitment. We needed a benchmark to discern those who had serious intentions in working with a therapeutic application and those who did not. Parents who invested the time to truthfully fill-out an extensive questionnaire on two separate occasions demonstrated such minimal commitment. (Questionnaires that were suspected of containing false answers, 16.5% of all questionnaires, were deleted from the pool). This automatically selected subjects who used MITA for at least four months. As of December 2016, the number of subjects who completed two or more questionnaires was 1,319, which corresponds to 6% of all potential subjects who registered MITA from February to September 2016.
2. The subject must have self-reported their diagnosis as ASD: Since our primary interest is early intervention for ASD, only data from ASD subjects, independent of ASD severity, were analyzed for this report. Out of the 1,319 subjects who completed at least two questionnaires, 852 self-reported their diagnosis as ASD. Other subjects reported diagnoses of various neurodevelopmental disorders. Some subjects chose not to report a diagnosis since this was not a required field.
3. The subject must have been 12 years of age or younger at the time of registration: Since we are interested in the effects of early intervention, we decided to limit our analysis to subjects who were twelve years of age or younger at the time of the first questionnaire. Therefore, we excluded another 29 subjects because of age. Thus, the total number of subjects included for analysis was reduced to 823 (4% of all February to September 2016 registrants).
The subject must have been 12 years of age or younger at the time of registration: Since we are interested in the effects of early intervention, we decided to limit our analysis to subjects who were twelve years of age or younger at the time of the first questionnaire. Therefore, we excluded another 29 subjects because of age. Thus, the total number of subjects included for analysis was reduced to 823 (4% of all February to September 2016 registrants).
Table 1 The number of subjects in each age group.
| Age |
Age marked on the graphs |
Number of subjects in each age group |
% subjects in each age group |
| 1.5 to 2.9 |
2 |
190 |
23 |
| 3 to 3.9 |
3 |
265 |
32 |
| 4 to 4.9 |
4 |
143 |
17 |
| 5 to 5.9 |
5 |
79 |
10 |
| 6 to 6.9 |
6 |
56 |
7 |
| 7 to 12.9 |
7 to 12 |
90 |
11 |
| Total |
|
823 |
100 |
Table 1: The number of subjects in each age group.
Statistical analysis
Data presented in this report is distributed non-normally with significant positive skewness and therefore presented as median with interquartile ranges (IRQ, 25th and 75th percentiles). Differences between groups were calculated with the Mood’s Median Test.
MITA exercises
MITA consists of nine different developmental activities, all of which follow a systematic approach to train the skill of multiple cues responding, and eight of the activities provide this training outside of the verbal domain [18]. This unique feature allows the activities to be within reach of those who are either nonverbal or minimally verbal. While these children may not be able to follow an explicit verbal command (such as “pick up the red crayon under the table”), results from our studies have demonstrated that they can follow a command implicit in the visual set-up of the puzzle.
To teach children to follow visual commands that require attending to multiple cues, the MITA program starts with puzzles that require attending to one cue, such as color (Figure 1A) or size (Figure 1B), and then progresses to two cues, such as both color and shape (Figure 1C) or color and size (Figure 1D) and eventually to three or more cues (Figure 1E).
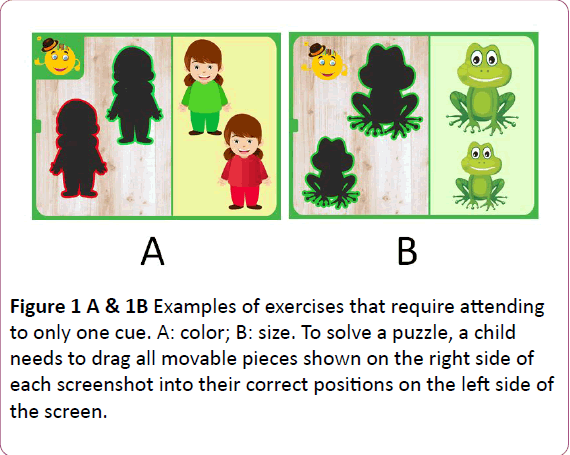
Figure 1A & 1B: Examples of exercises that require attending to only one cue. A: color; B: size. To solve a puzzle, a child needs to drag all movable pieces shown on the right side of each screenshot into their correct positions on the left side of the screen.
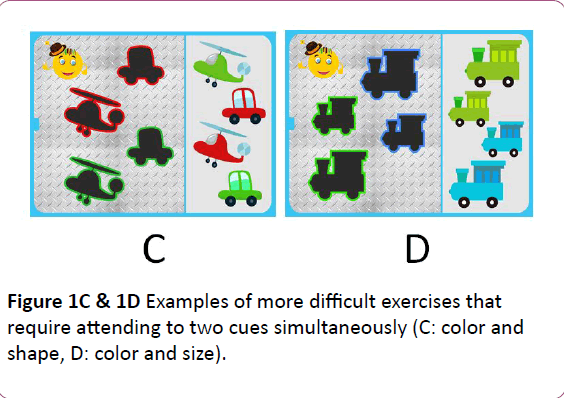
Figure 1C & 1D: Examples of more difficult exercises that require attending to two cues simultaneously (C: color and shape, D: color and size).
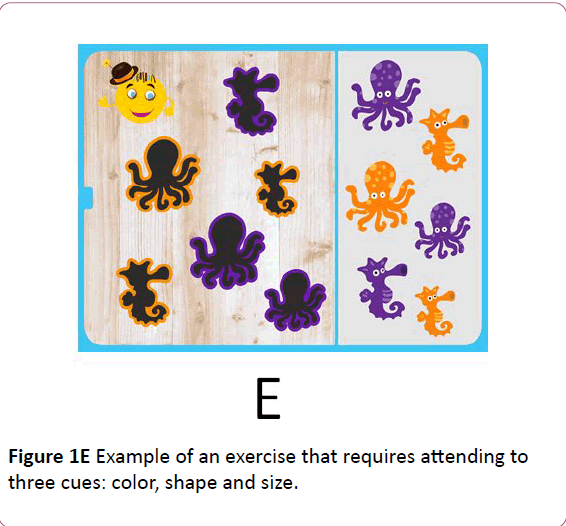
Figure 1E: Example of an exercise that requires attending to three cues: color, shape and size.
In addition to color, shape and size, MITA activities sometimes require attention to an object’s orientation in space as well as minor visual details. The choice of these particular stimuli was made to reflect those commonly used by PRT behavioral therapists who intentionally structure the therapeutic environment to include objects of various color, shape and size and then ask the child to find an object based on two (or more) of these features (25).
Daily session
MITA activities are organized into daily sessions. The length of the daily session is determined by the number of activities presented on the screen as well as the number of puzzles in each activity. The length of the daily session automatically adjusts based on age and performance. These benchmarks were based on recommendations from ABA specialists.
The initial number of activities in each session was set to four activities for children younger than six years of age, five activities for children between the ages of six and eight, and six activities for older children. The number of activities automatically increased by one (until the maximum of six) once the child had shown progress by completing at least half of the difficulty levels in any two activities.
In addition to these automated settings, the number of activities could also be manually adjusted to anywhere from one to six activities per session (with a minimum of 5 puzzles in each activity). Once children complete all the puzzles in each of the daily session’s activities, they are rewarded with Playtime.
Following the recommendations of consulting ABA specialists, we advised parents to exercise with MITA for approximately 10 minutes each day until the child is able to reach the top difficulty level in each activity, which is likely to take as long as two to three years for a typical subject.
Measuring cognitive growth
MITA uses adaptive-learning technologies, meaning that the exercises adapt to a child’s performance, resulting in a customized learning experience. The delivery of the exercises within each activity is entirely responsive to the child's progress and is determined through measurable criteria for mastery. In order to progress to the next level of difficulty for any particular activity, a child needs to answer correctly on the first attempt for 7 out of 10 consecutive puzzles in that activity. This strict algorithm avoids the undesirable situation in which a child progresses to the next level by simply using trial-and-error without mastering a particular skill.
The difficulty level is reduced if a child makes 12 or more errors in 10 consecutive puzzles. Accordingly, only a child engaged with the exercises can progress over difficulty levels, making progress along difficulty levels a useful indicator of child’s engagement with each activity. The adaptive algorithm ensures that the puzzles are adequately challenging but not too difficult. We also advised parents to monitor progress and adjust difficulty levels and settings to avoid child frustration as much as possible.
Results and Discussion
In this manuscript we report data from a feasibility study of parent-administered tablet-assisted therapy for children with ASD. We were especially interested in the performance of the youngest participants in our study, since it is one of first and largest studies to examine the feasibility of administrating tablet-based cognitive exercises to two-year-old toddlers diagnosed with ASD. We have measured and analyzed the performance of 823 children who have been working with the Mental Imagery Therapy for Autism (MITA) application for four to ten months. We evaluated the application along four parameters: usability, feasibility, fidelity of implementation, and promise of outcomes.
Usability: Are children able to understand and physically use the application?
To assess basic MITA usability quantitatively we calculated the following daily averages by age group: (1) the number of puzzles solved (Table 2) and (2) the amount of time spent engaging with the MITA app (Table 3).
| Age group |
2 |
3 |
4 |
5 |
6 |
7 to 12 |
| Median |
31 |
36 |
35 |
42 |
51 |
60 |
| QUARTILE1 |
22 |
25 |
25 |
29 |
29 |
40 |
| QUARTILE3 |
49 |
51 |
56 |
55 |
69 |
75 |
| 9th percentile |
16 |
20 |
19 |
19 |
22 |
28 |
| 91st percentile |
73 |
76 |
76 |
84 |
105 |
102 |
Table 2: The number of puzzles solved per day in multiple age groups.
| Age group |
2 |
3 |
4 |
5 |
6 |
7 to 12 |
| Median |
9.3 |
10.3 |
9.8 |
10.9 |
13 |
14.4 |
| QUARTILE1 |
6.6 |
7.2 |
6.2 |
7.8 |
8 |
10.6 |
| QUARTILE3 |
12.7 |
14.1 |
14.7 |
14.6 |
17.1 |
21.4 |
| 9th percentile |
4.8 |
5 |
4.7 |
5.4 |
6.3 |
7.6 |
| 91st percentile |
20.6 |
22.7 |
21 |
23 |
31.4 |
26.3 |
Table 3: Theduration in minutes of MITA exercises per day in multiple age groups.
1. The median (IQR) number of puzzles solved per day by twoyear- old subjects was 31.4 (21.5-48.6, Figure 2), which was just above the therapist-recommended benchmark for that age group. Pair-wise comparison between all contiguous age groups showed no statistical significance in the number of puzzles solved per day between the two- and three-year-old age group, between the three- and four-year-old age group, or between the four- and five-year-old age group. There was a statistical significance between the five- and six-year-old age groups (P=0.03) as well as the six- and seven to twelveyear- old age group (P=0.04). This was likely a result of the automated app settings which require older children to complete a greater number of puzzles before earning Playtime.
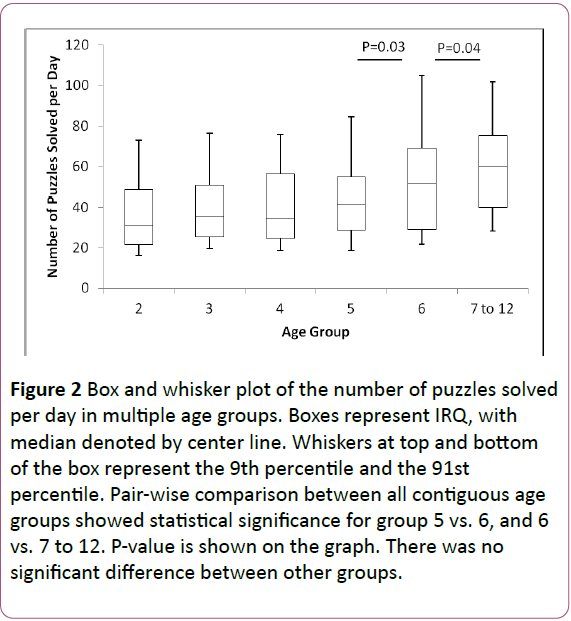
Figure 2: Box and whisker plot of the number of puzzles solved per day in multiple age groups. Boxes represent IRQ, with median denoted by center line. Whiskers at top and bottom of the box represent the 9th percentile and the 91st percentile. Pair-wise comparison between all contiguous age groups showed statistical significance for group 5 vs. 6, and 6 vs. 7 to 12. P-value is shown on the graph. There was no significant difference between other groups.
2. The median (IQR) amount of time spent with the MITA exercises per day by two-year-old subjects was 9.3 minutes (6.6-12.7, Figure 3), which fell just below our recommendation of ten minutes per day. There was no statistically significant difference in the duration of MITA exercises per day between any of the age groups. The small increase in the duration of MITA exercises in older children is again the result of the automated app settings which require older children to complete a greater number of puzzles before earning Playtime.
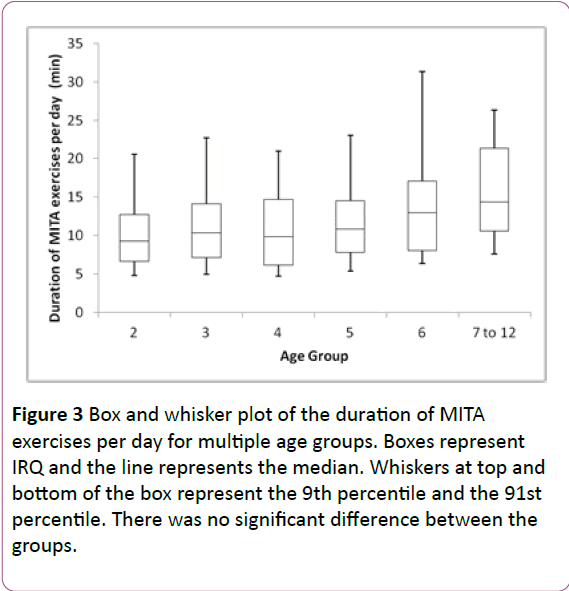
Figure 3: Box and whisker plot of the duration of MITA exercises per day for multiple age groups. Boxes represent IRQ and the line represents the median. Whiskers at top and bottom of the box represent the 9th percentile and the 91st percentile. There was no significant difference between the groups.
The quantitative data allows us to conclude that children as young as two are able to engage with the activities contained in a therapeutic app for close to ten minutes per day, and are able to complete a recommended daily session.
Feasibility: Can the application be used over an extended period of time?
In this study, all participants exercised with MITA for four to ten months. Over this interval, the median (IRQ) number of days each child worked with MITA was 39 (23-64) and the median (IRQ) total number of solved puzzles was 1,377 (748-2,814).
MITA usage indicates that children were able to come back to MITA day after day over the course of months. However, MITA exercises are expected to have their greatest effect in those who exercise consistently over several years. Given the rate of progress of an average child, MITA was developed to last for two to three years. All participants were advised to continue working with MITA as often as possible and as long as possible. Unfortunately, there was significant dropout from the study, Figure 4.
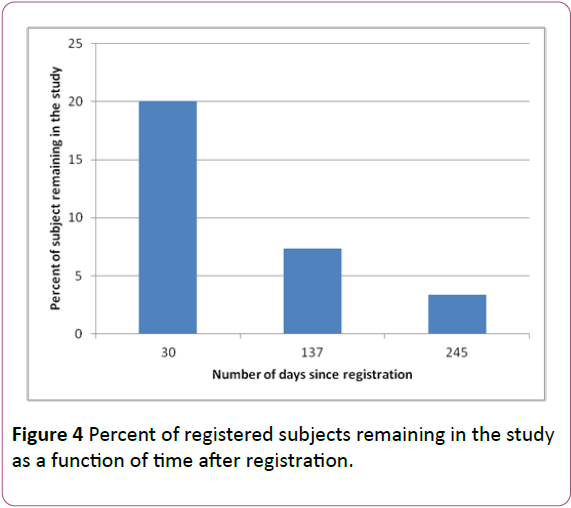
Figure 4: Percent of registered subjects remaining in the study as a function of time after registration.
One of the main reasons cited by parents for dropping out of the study is that their child lost interest in Playtime, MITA’s primary reward structure. MITA’s activities require a significant cognitive effort that is balanced by a Playtime at the end of each daily session. We made the Playtime virtually unlimited; once a child completed a daily session, he could enjoy any one of six Playtime activities for as long as he wanted until the next daily session.
Parents who worked with MITA for over six months indicated that their children initially enjoyed and looked forwards to Playtime but eventually lost interest requiring parents to move their incentive to involve alternative physical or emotional rewards such as small gifts, verbal praise and hugs. At the time of writing this manuscript, the monotonous and unlimited Playtime may be the main culprit of children losing interest in MITA. We are currently working to improve our incentive/ reward structure by making it more varied and time-limited as well as allowing parents to personalize it to reflect their child’s unique interests, with the goal of maintaining engagement for a variety of kids over the course of years.
MITA usage data indicates it is feasible for a therapeutic application to be used over the course of months by kids as young as two, but there is insufficient data about the feasibility of multi-year usage. We are continuing our study and will be able to report in the future about the effects of an improved reward structure on subject retention.
Fidelity of Implementation: Is the application being used as it was intended? How does actual usage compare to recommended usage?
To assess the fidelity of implementation we compared usage recommendations with actual performance data. We recommended that MITA be used daily. Although there was one subjects who worked with MITA every day for over six months, confirming that it is possible to work with MITA on a daily basis, the actual median (IQR) number of days MITA was used per week was 1.6 (0.9-2.6), significantly less than our recommendation. Only 161 subjects (20%) worked with MITA more than 3 days per week; only 60 subjects (7%) worked with MITA more than 4 days per week; and only 24 subjects (3%) worked with MITA more than 5 days per week.
Notably, there was a trend toward a reduction of the number of days per week MITA was used in older children, Table 4 and Figure 5. Three-year-old children used MITA significantly fewer times per week than two-year-old children (p<0.005), and four year old children used it fewer times per week than three-yearold children (p<0.001).
| Age group |
2 |
3 |
4 |
5 |
6 |
7 to 12 |
| Median |
2 |
1.6 |
1.2 |
1.5 |
1.4 |
1.4 |
| QUARTILE1 |
1.2 |
1 |
0.7 |
0.6 |
0.6 |
0.8 |
| QUARTILE3 |
3.1 |
2.6 |
1.9 |
2.5 |
2.4 |
2.7 |
| 9th Percentile |
0.9 |
0.6 |
0.5 |
0.3 |
0.3 |
0.5 |
Table 4: The number of days MITA was used per week in multiple age groups.
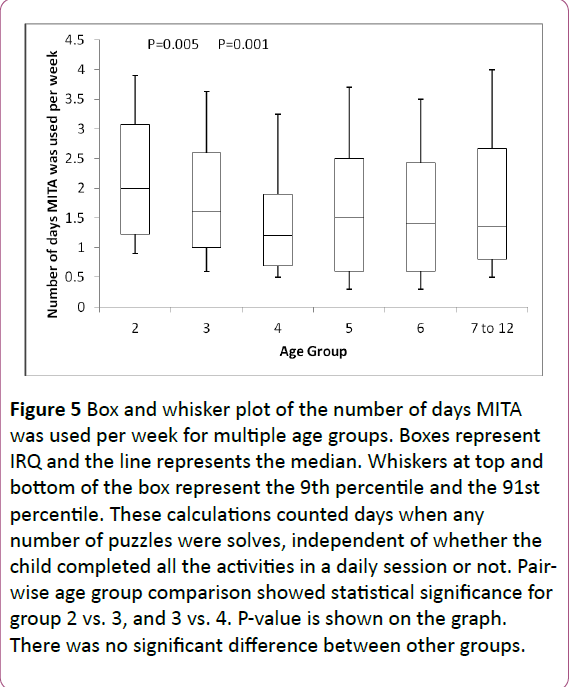
Figure 5: Box and whisker plot of the number of days MITA was used per week for multiple age groups. Boxes represent IRQ and the line represents the median. Whiskers at top and bottom of the box represent the 9th percentile and the 91st percentile. These calculations counted days when any number of puzzles were solves, independent of whether the child completed all the activities in a daily session or not. Pairwise age group comparison showed statistical significance for group 2 vs. 3, and 3 vs. 4. P-value is shown on the graph. There was no significant difference between other groups.
The reasons for the less frequent use of MITA by older children may include a greater competition in the app space for older children. In addition, since the vast majority of participants were from the USA where a plethora of services are available to older children diagnosed with ASD, it is possible that this pattern of use may be explained by enrollment in other therapies. Since there are fewer services available for younger children [7] parents may be more likely to fill in the gap by working with kids on their own. When services do become available, parents may be less willing to administer MITA on their own.
Though we cannot conclusively comment on fidelity of implementation over a long period of time, we can conclude that the observed trend rejects the hypothesis that MITA administration is difficult with two-year-old children. On the contrary, our data shows a more consistent use of MITA in twoyear- old children compared to any other age group.
It is unclear whether changes in the app design could influence parents’ decision to use MITA daily. It is possible though that if MITA benefits were confirmed and a physician or a therapist was to recommend daily exercises with MITA, parents could work with MITA more regularly.
Promise of Outcomes: Can a child show improvement within an activity?
A child’s ability to improve was assessed by their progression through pre-set difficulty levels. As described in methods, difficulty level is automatically increased when a child answers correctly on the first attempt in at least 7 out of 10 consecutive puzzles. The difficulty level is reduced if a child makes 12 or more errors in 10 consecutive puzzles. Any automatic increase in an activity’s difficulty level from the first use to the last use of MITA (an interval of anywhere from four to ten months) was defined as “progress.” Progress was calculated separately for each activity and used as an indicator of both understanding of requirements of that activity and engagement in that activity. Staying at the same difficulty level or a drop in difficulty level was defined as “no progress.” Note that children in the “no progress” group were still able to complete all the puzzles, albeit with errors.
Overall, 818 out of 823 children (99%) progressed in at least one activity; 98% of children progressed in half of the activities they attempted (e.g. 2 out of 4 activities attempted, 3 out of 6 activities attempted, or 4 out 8 activities attempted); 91% progressed in 75% of activities attempted; and 69% progressed in 100% of activities attempted. Figure 6 shows the progress rate calculated for each age group. The decrease in “progress in 100% of activities” in the 5, 6, and 7-12 age groups compared to younger children was the result of the initial MITA setting requiring older kids to start activities at a higher difficulty level and also requiring them to play a greater number of more difficult activities.
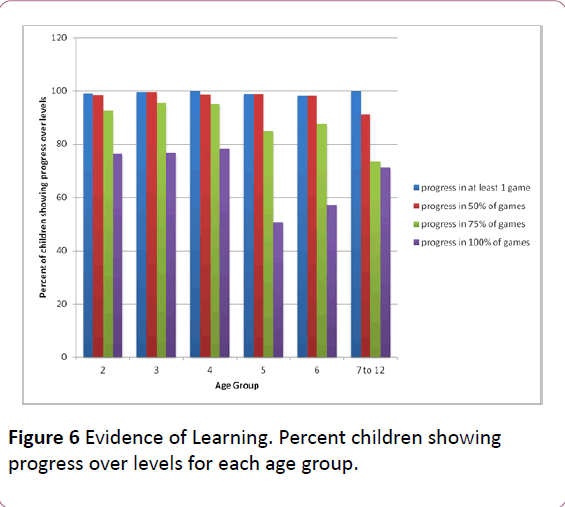
Figure 6: Evidence of Learning. Percent children showing progress over levels for each age group.
Furthermore we have been interested in the number of subjects who showed significant progress. Significant progress in an activity was defined as the progress of 5 or more levels. Overall, 738 out of 823 children (90%) showed significant progress in at least one activity; 66% of children showed significant progress in half of the activities they attempted; 40% showed significant progress in 75% of activities attempted; and 14% showed significant progress in 100% of activities attempted.
Figure 7 shows the significant progress rate calculated for each age group.
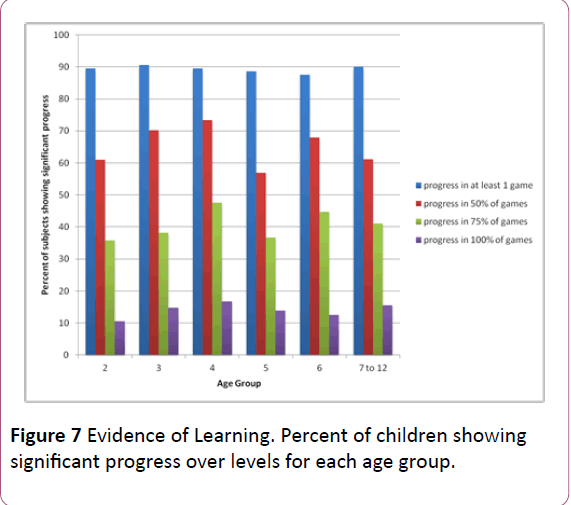
Figure 7: Evidence of Learning. Percent of children showing significant progress over levels for each age group.
The data allows us to conclude that the majority of children were showing progress and climbing along their cognitive ladder. Crucially, there was no significant difference in progress between the two-year-old group and older children.
Conclusions
In this manuscript we report data from a feasibility study of parent-administered tablet-assisted therapy for children with ASD. To our knowledge, it is the first study of tablet-based cognitive exercises administered to two-year-old toddlers with autism. It is also the largest study of an early parentadministered intervention tool to toddlers with autism (compare to Ref. [26]). By looking at the performance of 823 children who have been working with the Mental Imagery Therapy for Autism (MITA) computerized learning application for four to ten months, we conclude that 1) MITA works as designed; 2) Parents are capable of administering tablet-based therapy; 3) children with ASD were fully engaged with the MITA application; 4) children as young as two years of age (as well as older children) were able to engage with MITA exercises.
MITA effectiveness is currently being tested in a larger longitudinal clinical trial. The goal of the longitudinal clinical trial is to test the hypothesis that regular practice with MITA will result not only in a greater ability to attend to multiple cues, but also in vast improvements on transfer tasks measuring visuospatial as well as communicative skills. Furthermore, we hope to show that MITA, coupled with an effective vocabulary training program, can lead to improvements in the realm of language comprehension. We predict that children who begin training at an early age, and who make consistent progress over the course of training, will see drastic improvements in their language function. Since many kids diagnosed with ASD are already receiving ample vocabulary training, what's missing is the skill to attend to various syntactic combinations of learned words, i.e. true flexible language comprehension. For example, a child who has learned the words "fish," "ate" and “cat” but who cannot mentally synthesize those words into a novel scene, would struggle to understand the difference between “a fish ate a cat” and “a cat ate a fish”, while a similar child who has learned mental synthesis will be successful with the task. Combining the mental synthesis ability with vocabulary knowledge, will result in an understanding of a full syntactic language, which will eventually lead to a significant reduction of the severity of the ASD diagnosis and ultimately to a more productive and independent life.
Competing Interests
Rita Dunn, Jonah Elgart, Lisa Lokshina, Alexander Faisman, Yuriy Gankin, and Andrey Vyshedskiy have financial interests in ImagiRation LLC, the developer of Mental Imagery Therapy for Autism (MITA) application for children with ASD. Other than that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.
References
- Wingate, M (2014) Prevalence of autism spectrum disorder among children aged 8 years-autism and developmental disabilities monitoring network, 11 sites, United States, 2010. MMWR SurveillSumm 63: 2.
- Yeargin-Allsopp M, Rice C, Karapurkar T, Doernberg N, Boyle C, et al. (2003) Prevalence of autism in a US metropolitan area. Jama 289: 49-55.
- Eldevik S, Hastings RP, Hughes JC, Jahr E, Eikeseth S, et al. (2010) Using participant data to extend the evidence base for intensive behavioral intervention for children with autism. Am. J. Intellect. Dev. Disabil 115: 381-405 .
- Peters-Scheffer N, Didden R, Korzilius H, Sturmey P (2011) A meta-analytic study on the effectiveness of comprehensive ABA-based early intervention programs for children with autism spectrum disorders. Res Autism SpectrDisord 5: 60-69.
- Virués-Ortega J (2010) Applied behavior analytic intervention for autism in early childhood: Meta-analysis, meta-regression and dose–response meta-analysis of multiple outcomes. ClinPsychol Rev 30: 387-399.
- Maglione MA, Gans D, Das L, Timbie J, Kasari C (2012) Nonmedical interventions for children with ASD: Recommended guidelines and further research needs. Pediatrics 130: 169-178 .
- Hume K, Bellini S, Pratt C (2005) The usage and perceived outcomes of early intervention and early childhood programs for young children with autism spectrum disorder. Top Early Child Spec Educ 25: 195-207.
- Johnson E, Hastings RP (2002) Facilitating factors and barriers to the implementation of intensive home-based behavioural intervention for young children with autism. Child Care Health Dev 28: 123-129.
- Bibby P, Eikeseth S, Martin NT, Mudford OC, Reeves D (2002) Progress and outcomes for children with autism receiving parent-managed intensive interventions. Res Dev Disabil 23: 81-104.
- Jacobson J W (2000) Early intensive behavioral intervention: Emergence of a consumer-driven service model. Behav Anal 23: 149.
- Wise MD, Little AA, Holliman JB, Wise PH, Wang CJ (2010) Can state early intervention programs meet the increased demand of children suspected of having autism spectrum disorders. J Dev BehavPediatr 31: 469-476.
- Mandell D, Knapp M (2012) Estimating the economic costs of autism. Invest Our Future Econ. Costs Autism Summit ESF Cent. Quarry Bay Hong Kong.
- Shukla-Mehta S, Miller T, Callahan KJ (2010) Evaluating the effectiveness of video instruction on social and communication skills training for children with autism spectrum disorders: A review of the literature. Focus Autism Dev Disabil 25: 23-36.
- Bernard-Opitz, V, Sriram N, Nakhoda-Sapuan S (2001) Enhancing social problem solving in children with autism and normal children through computer-assisted instruction. J Autism Dev Disord31: 377-384.
- Schreibman L, Whalen C, Stahmer AC (2000) The use of video priming to reduce disruptive transition behavior in children with autism. J Posit BehavInterv 2: 3-11.
- Jowett EL, Moore DW,Anderson A (2012) Using an iPad-based video modelling package to teach numeracy skills to a child with an autism spectrum disorder. Dev Neurorehabilitation 15: 304-312.
- Kagohara DM, Sigafoos J, Achmadi D, O’Reilly M, Lancioni G (2012) Teaching children with autism spectrum disorders to check the spelling of words. Res Autism SpectrDisord 6: 304-310.
- Vyshedskiy A, Dunn R (2015) Mental Imagery Therapy for Autism (MITA)-An Early Intervention Computerized Brain Training Program for Children with ASD. Autism Open Access 5: 2.
- WilczynskiS. et al. (2009) National standards report: The national standards project: Addressing the need for evidence-based practice guidelines for autism spectrum disorders.Natl Autism Cent.
- Lovaas OI, Schreibman L, Koegel R, Rehm R (1971) Selective responding by autistic children to multiple sensory input. J AbnormPsychol 77: 211.
- Schreibman L (1988) Diagnostic features of autism. J Child Neurol 3: 57-64.
- Lovaas OI, Koegel RL, Schreibman L (1979) Stimulus overselectivity in autism: A review of research. Psychol Bull 86: 1236-1254.
- Ploog BO (2010) Stimulus overselectivity four decades later: A review of the literature and its implications for current research in autism spectrum disorder. J Autism Dev Disord 40: 1332-1349.
- Burke JC, Cerniglia L (1990) Stimulus complexity and autistic children’s responsivity: Assessing and training a pivotal behavior. J Autism Dev Disord 20: 233-253.
- Hiniker A, Daniels JW, Williamson H (2013) Go go games: therapeutic video games for children with autism spectrum disorders. Proceedings of the 12th International Conference on Interaction Design and Children 463-466.
- Venkatesh S, PhungD, Duong T, Greenhill S,Adams B (2013) TOBY: early intervention in autism through technology.Proceedings of the SIGCHI Conference on Human Factors in Computing Systems 3187-3196.

