Keywords
Accident and emergency (A&E); Elasticity; Hospitalization; Patientsharing; Jamaica
Introduction
Public hospital management has had to deal with a number of operating fundamentals and management challenges inclusive of inadequate infrastructure, inefficient analytic processes, insufficient staffing and recruitment pool, increased patient demands and new re-emerging health conditions, resource constraints and physio-psychological trauma [1,2]. Furthermore, public healthcare managers need to be armed with the necessary data and information to assist them to be more proactive in managing the limited resources allotted. Information in health care planning is needed to bolster the health system to respond to new and ongoing challenges like virus outbreaks, the impact of government policies aimed at addressing health care challenges and the need to improve patient satisfaction. Therefore, having information in health care planning is critical to effective management practices. One of the difficulties in health care planning in Jamaica is imperfect information or the lack of accurate, current, and relevant information, especially from empirical inquiry. This hampers effective and futuristic planning. How do health care providers plan for health epidemics such as Chikungunya that occurred in 2014 when there is no prior warning in the health literature or public health alerts? Communicable diseases such as Chikungunya and Zika have taken Jamaica by surprise over the years and the severity of the matter overburdened the health care facilities because of health care management deficiency [3-7]. The challenge for health specialists and planners is having the ability to effectively manage issues such as increased patient usage due to new and re-emerging health outbreaks. Patient-sharing is a necessary and effective management solution to inadequate resources; however, lack of necessary administrative data can result in numerous public health implications which may significantly retard effective hospital management.
Kingston Public Hospital (K) is the only national trauma facility in Jamaica and it was the first hospital to be built in the nation (South East Regional Health Authority (SERHA) was built and became operational on December 12, 1776. It is the largest trauma center in the English-Speaking Caribbean [8] and provides services like Hemodialysis and Radiotherapy for Jamaica and the wider English-Speaking nations. The very nature of K makes it a hug for patient-sharing when other hospitals are unable to adequately address the trauma experienced by the patient. K is located in Kingston, the capital of Jamaica, in the midst of many violence pruned communities in Western Kingston (Hannah Town; Tivoli Gardens; Matthews Lane, Pink Lane; Craig Town (Figure 1)–Map of Jamaica showing the location of Kingston Public Hospital and Spanish Town Hospital).
Figure 1: Map of Jamaica by Parishes.
Although a government hospital is located in each parish in Jamaica certain cases must be referred to the Kingston Public Hospital depending on the severity of those cases. As a consequence of the specialized services offered by the K, many trauma cases outside of the parish of Kingston and St. Andrew are referred to this institution as well. The Spanish Town Hospital is one of the many government hospitals in Jamaica that dispatches patients to the national trauma centre on a daily basis.
The Spanish Town Hospital, like Kingston Public Hospital, is located in the midst of violence proned communities in the neighboring parish of St. Catherine. such as Thompson Pen, Lakes Pen, Lauriston, Shelter Rock, St. Johns Road, De la Vega City, Lime Tree and De la Vega City (Figure 2). With the location of the hospital, in the capital of Spanish Town, there is a greater demand for this institution to manage trauma cases from sporadic gun violence between rivaling gangs [9-17] to more critical types of trauma.
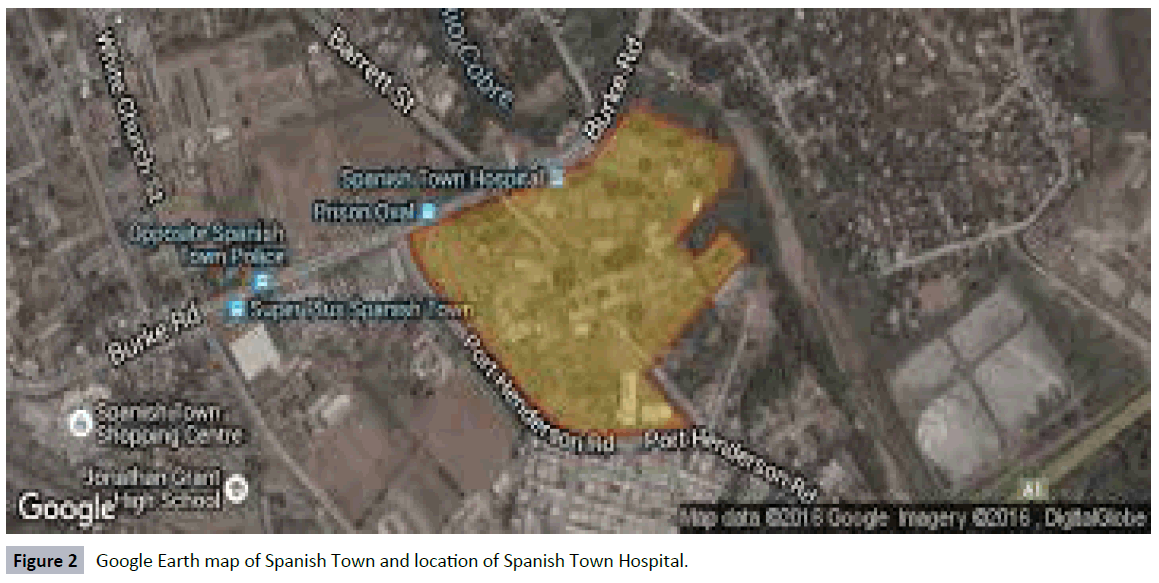
Figure 2: Google Earth map of Spanish Town and location of Spanish Town Hospital.
Spanish Town Hospital, established June 18, 1952 by Sir Hugh Foote, is relocated on 10 Kings Street in Spanish Town to St. Jago Park sugar and banana plantation. The Spanish Town Hospital is arguably the busiest Type-B hospital in Jamaica. It serves the entire parish of St. Catherine as well as the growing housing development in Portmore, a dormitory community in the parish with a population of nearly 300,000 (3013). In 2015, the Spanish Town Hospital had a medical and ancillary staff of approximately 688 personnel (i.e., professional, technical and administrative personnel) to serve some 41,260 patients. This means that, on average, there are 60 patients for every 1 staffer. The numbers are even more staggering for nurses and patient care personnel. For example, there are, roughly 126 nurses to service all patients seen at the hospital. This figure includes registered nurses, registered midwives; enrolled nurses; patient care assistants and assistant theatre technicians.
Health care professionals in Jamaica face the arduous task of long term planning because of situations such as: 1) Virus outbreaks; 2) Migration of health care professionals; 3) Changes in government policies; and 4) Change of political administration [18-20]. On April 1, 2008, months after the island experienced a change in political administration; the new government implemented a policy that sought to remove user fees from public health care institutions. This resulted in the unplanned increase in visits to the government hospitals as a major barrier to hospital access was removed. Importantly, this policy was implemented within the context of a shortage of health professionals leading to overburdening of the human and physical resources. The lack of strategic planning to support the new policy directives created additional challenges for health specialists in this nation.
The crisis that obtains as a result of the shortage of nurses in the public hospitals in Jamaica [18,21-23] is no different from the crisis that exists in other nations [24-27]. The undue pressures placed on health care institutions are always high in public discussion. However, due to budget constraints among other issues resolution to this crisis is slow to come and this places additional stress on health care facilities
In 2007, a group of scholars conducted a national stratified probability cross-sectional survey and found that dissatisfaction with the services of the health sector was identified as the fourth of 20 leading national problems indicated by Jamaicans. Upon examination of the literature, no study emerged that examined patient-sharing at hospitals. Consequently, the probabilities of these occurrences and elasticities of patient-sharing are unknown. Although many studies have been conducted on patient-sharing outside of Jamaica, whether inside or outside of Jamaica [28-30], none of the research evaluated the issue from the perspective of probabilities of patient-sharing, and modeling patient-sharing between two hospitals. This study aims to bridge the gap in the literature by evaluating the following objectives: 1) Probabilities of hospitalization at two government hospitals in Jamaica; 2) Elasticities of hospitalization between two government hospitals in Jamaica; 3) Response-ability between the two government hospitals in Jamaica in relation to patient-sharing; and 4) The dual effect of patient-sharing in two government hospitals in Jamaica.
Theoretical Framework
Regression analysis is an econometric tool that is widely used in quantitative research. It allows for the examination of many independent variables on a single dependent variable. Econometricians such as Hill et al. [31], Mamingi [32] and Wooldridge [33] have shown how Ordinary Least Square (OLS) can be used to model many linear variables simultaneously influenced by a single dependent variable. Harcourt [34] applied regression analysis established youth population rates, macroeconomic conditions, and demographic characteristics on lagged homicide for the United States. He used 68 years of panel data to develop this model-a mathematical model that examines the relationship between homicide rates and institutionalization at a mental health facility in the United States presented in equation (1):
logHomicide Ratessy = α + βInstitutionalization Ratesy + θControlssy + ϒs + δy + ϒ + Ã (1)
“where ‘s’ represents states and ‘y’ reflects the year. The dependent variable of interest in this class of models is the natural log of the annual homicide rate for each state, which is obtained using vital statistics measures of death by homicide. The key explanatory variable of interest is the 1-year-lagged rate of aggregated institutionalization in state and federal prisons, in public mental hospitals, and in other institutions for the mentally ill. The model uses a weighted least squares regression, with weights equal to the annual population of the states, clustering standard errors at the state level. The model conditions on state and year fixed effects (ϒs and δy) to account for unmeasured factors that influence crime and either are constant within states over the study period or change over time but exert a constant influence over the entire set of states” [34].
For this study, we also used hospitalization in one hospital (Kingston Public hospital) and hospitalization at another government hospital (Spanish Town Hospital) in Jamaica for time period t [equation (2)]:
Kt= ƒ(St) (2)
Where Kt denotes hospitalization at the national trauma hospital (i.e., Kingston Public hospital) and St is Spanish Town hospital–both hospitals are government institutions.
Methods and Materials
The data for this study were taken from the Ministry of Health publication (2006-2015). In addition, admission data to a Jamaican national mental health public hospital (Bellevue Hospital), for the period of 2006-2015, were obtained from the Ministry of Health. The period for this work is from 2006 through to 2015. Data were recorded, stored and retrieved using the Statistical Packages for the Social Sciences (SPSS) for Windows, Version 24.0. The level of significance that is used to determine statistical significance is less than 5% (0.05) at the 2-tailed level of significance. Ordinary Least Square (OLS) regression was used to determine factors of hospitalization to Kingston Public hospital as well as the strength of the relationship, using R2. Curve estimations were used in order to determine other functions with the purpose of ascertaining a best fit function.
In order to meet the use of the OLS application, for this study, all the assumptions were met before usage. Where highly intercorrelated variables (r > 0.7) are employed their tolerance were checked and if multi-colinearity was discovered, one of the variables was dropped and used separately in a model without the highly correlated variable.
Probabilities of hospitalization (or admission): This is the total number of people who are admitted at a hospital (Σ Admission for time period t) divided by the total number of who attend the hospital to the accident and emergency (A&E) department for a given time period, t (Σ attendance for time period, t):

Specialized probabilities of hospitalization
Probability of admissions at Spanish Town hospital for time period, t:

Probability of admissions at Kingston Public hospital for time period, t:

Probability of patient-sharing between Kingston Public and Spanish Town hospitals for time period t:

Where P (St) denotes the probability of hospitalization at Spanish Town hospital and P (Kt) means the probability of hospitalization at the Kingston Public hospital for time period i. Given that hospitalization to one hospital precludes a simultaneous admission to another, it follows that patient-sharing would be independent events and so it is a multiplication between P (St) and P (Kt).
Elasticities of hospitalization

Where η is the elasticity of hospitalization,
% Δ denotes the percentage change in hospitalization for t+1 and t.
Interpretations of elasticities results:
η > 1: elastic hospitalization or highly responsive hospitalization meaning that a one percentage change in the denominator will result in a more than 1 percentage change in the numerator;
η < 1: inelastic hospitalization or lowly responsive hospitalization which denotes that a one percentage change in the denominator will result in a less than 1 percentage change in the numerator;
Interpreting signs of the elasticities
Negative sign means substitution effect or one product can operate outside of the other and for this study it means that hospitalization in one health institution is taken care of there, only;
Positive sign means complementary effect or one product operates jointly with another and for this study it means patientsharing is occurring between hospitals.
Substitution effect
η < -1: This is a substitution effect that is highly responsive.
η < -1: This is a substitution effect this is lowly responsive.
Complementary effect
η > -1: This is a complementary effect that is lowly responsive.
η < +1: this is a complementary effect that is highly responsive.
Findings
Table 1 presents data on admissions at two government hospitals in Jamaica, Spanish Town and Kingston Public Hospitals. Kingston Public Hospital is the national trauma center for the country. Over the last 10 years (2006-2015), the average number of hospitalization to Kingston Public Hospital was 25,853 ± 2124, 95% CI: 24333-27372 compared to 17556 ± 2124, 95% CI: 16930- 18184 at Spanish Town Hospital. In the first five years (2006- 2010), the average number of hospitalization was 17,037 ± 553, 95% CI: 16,351-17,725 at Spanish Town Hospital compared to 24,167 ± 1,631, 95% CI: 22,142-26,192 at the Kingston Public Hospital. However, in the latter five years (2011-2015), the mean number of hospitalization at Spanish Town Hospital was 18077 ± 864, 95% CI: 17,004-19,151 compared to 27539 ± 619, 95% CI: 26,770-28,307 at Kingston Public Hospital. This means that the percentage increases over the two periods for Spanish Town Hospital was 6.1% compared to 14.0% for the Kingston Public Hospital.
| Year |
Hospitalizations |
| Kingston Public Hospital |
Spanish Town Hospital |
| 2006 |
21,603 |
16,214 |
| 2007 |
24,660 |
17,666 |
| 2008 |
23,596 |
16,799 |
| 2009 |
25,556 |
17,250 |
| 2010 |
25,419 |
17,259 |
| 2011 |
26,530 |
17,638 |
| 2012 |
28,708 |
17,099 |
| 2013 |
27,610 |
17,822 |
| 2014 |
28,228 |
18,482 |
| 2015 |
27,618 |
19,346 |
Table 1: Hospitalizations at Spanish Town and Kingston Public Hospitals in Jamaica.
Although, admissions at Kingston Public hospital has generally been trending downwards in the last five years (2011-2015), an exponential rise in hospitalization occurred in 2014 over 2013 (i.e., 68.4% hospitalization rate)–Table 1. This exponential rise in hospitalization was primarily owing to the Chikungunya virus outbreak. On the other hand, Spanish Town hospital has been experiencing constant increases in hospitalization in the latter five years (2011-2015) compared to the former five years (2006- 2010), with a marginal rise in 2014 over 2013.
Table 2 presents probabilities of hospitalization at Kingston Public and Spanish Town Hospitals in Jamaica. The probabilities are somewhat different for each hospital in the study as generally the values have been increasing for Spanish Town Hospital compared to the decline for the Kingston Public Hospital, with the exception of 2014. It should be noted that in 2014, Jamaica had an outbreak of the Chikungunya virus and accounted for a percentage of the rise in visits to the hospital and emergency (A&E) departments, and later by the rise in hospitalization.
| Year |
P(Kt) |
P(St) |
P(Kt).P(St) |
| 2006 |
0.445 |
0.366 |
0.163 |
| 2007 |
0.420 |
0.393 |
0.165 |
| 2008 |
0.365 |
0.351 |
0.128 |
| 2009 |
0.523 |
0.287 |
0.150 |
| 2010 |
0.361 |
0.366 |
0.132 |
| 2011 |
- |
0.421 |
- |
| 2012 |
0.338 |
0.416 |
0.141 |
| 2013 |
0.302 |
0.420 |
0.127 |
| 2014 |
0.684 |
0.440 |
0.301 |
| 2015 |
0.304 |
0.469 |
0.143 |
Table 2: Probabilities of hospitalization at Kingston Public Hospital (Kt) and Spanish Town Hospital (St) as well a patient-sharing [P(Kt).P(St)].
Patient-sharing is also captured by this mathematical formula, P(Kt).P(St). Based on the probabilities for P(Kt).P(St), patientsharing has always occurred between Kingston Public and the Spanish Town hospitals in Jamaica. In fact, for the 10-year period, the average patient-sharing rate was 17.8%, with highest rate being in 2014 during the Chikungunya virus when admission was the highest at Kingston Public and second highest at Spanish Town hospitals. During the outbreak of the Chikungunya virus, patient-sharing stood at the most between the two government hospitals. Such findings support the claim that Kingston Public is the national trauma institution for Jamaica.
Table 3 is a detailed presentation of elasticities of hospitalization between two hospitals in Jamaica. All the positive elasticities (η being positive) indicate patient-sharing (complementary effect). Such findings (2007, 2008, 2011, and 2014) indicate patientsharing between the national trauma hospital (Kingston Public Hospital) and Spanish Town Hospital. The substitution effects are also occurring in Jamaica as is evident from the current data, a situation in which the patients are treated solely at one hospital.
| Year |
Kingston Public Hospital
(K) |
Spanish Town Hospital |
% Δ in Admissions
at
K |
% Δ in Admissions at
Spanish Town Hospital |
η |
| 2006 |
21,603 |
16,214 |
- |
- |
- |
| 2007 |
24,660 |
17,666 |
14.15 |
8.96 |
1.58 |
| 2008 |
23,596 |
16,799 |
-4.31 |
-4.91 |
0.88 |
| 2009 |
25,556 |
17,250 |
8.31 |
2.68 |
3.09 |
| 2010 |
25,419 |
17,259 |
-0.54 |
0.05 |
-10.27 |
| 2011 |
26,530 |
17,638 |
4.37 |
2.20 |
1.99 |
| 2012 |
28,708 |
17,099 |
8.21 |
-3.06 |
-2.69 |
| 2013 |
27,610 |
17,822 |
-3.82 |
4.23 |
-0.90 |
| 2014 |
28,228 |
18,482 |
2.24 |
3.70 |
0.60 |
| 2015 |
27,618 |
19,346 |
-2.16 |
4.67 |
-0.46 |
Table 3: Elasticities of hospitalization between two hospitals in Jamaica(i.e., K and SPH).
Figure 3 depicts a scatter diagram of hospitalizations at the Spanish Town and Kingston Public Hospitals in Jamaica, using data from 2006-2015. Instead of using OLS regression to arrive with a model, the researcher examined the best fit for the scatter values and these are presented in Table 3 and 4.
| Dependent Variable: Hospitalization at Kingston Public Hospital |
| Equation |
Model Summary |
Parameter Estimates |
| R Square |
F |
df1 |
df2 |
Sig. |
Constant |
St |
St2 |
| Linear |
0.560 |
10.164 |
1 |
8 |
0.013 |
-5968.6 |
1.812 |
|
| Logarithmic |
0.578 |
10.937 |
1 |
8 |
0.011 |
-293847.3 |
32715.5 |
|
| Quadratic |
0.720 |
8.987 |
2 |
7 |
0.012 |
-290490.9 |
33.836 |
-0.001 |
| Power |
0.578 |
10.936 |
1 |
8 |
0.011 |
0.072 |
1.309 |
|
| Exponential |
0.558 |
10.116 |
1 |
8 |
0.013 |
7221.2 |
7.246E-5 |
|
Independent variable: Hospitalization at Spanish Town Hospital
Table 4: Model summary and parameter estimates.
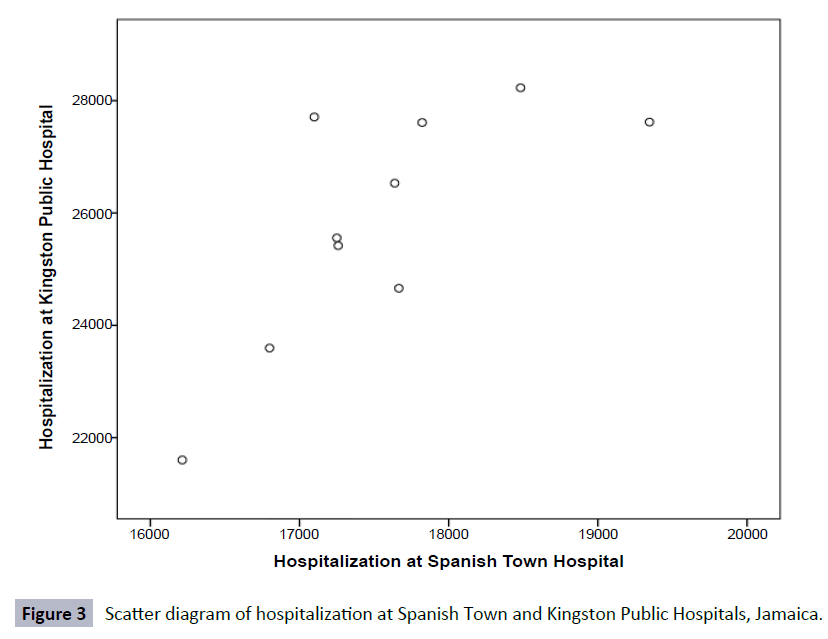
Figure 3: Scatter diagram of hospitalization at Spanish Town and Kingston Public Hospitals, Jamaica.
Table 3 presents a model summary and the estimates of the data using five different models. On examination of the squared R values, the best fit for the data is a quadratic function (i.e., 2-degree polynomial) because this accounts for 72.0% of the data values. Hence, hospitalizations at Kingston Public Hospital is represented by equation (3)
Kt = α + β1St + β2St2
Where β1 and β2 coefficients of hospitalizations at Spanish Town hospitals
Kt = -290490.9 + 33.836St - 0.001St2
With the coefficient of St2 being negative, the curve is concave downwards (Figure 4).
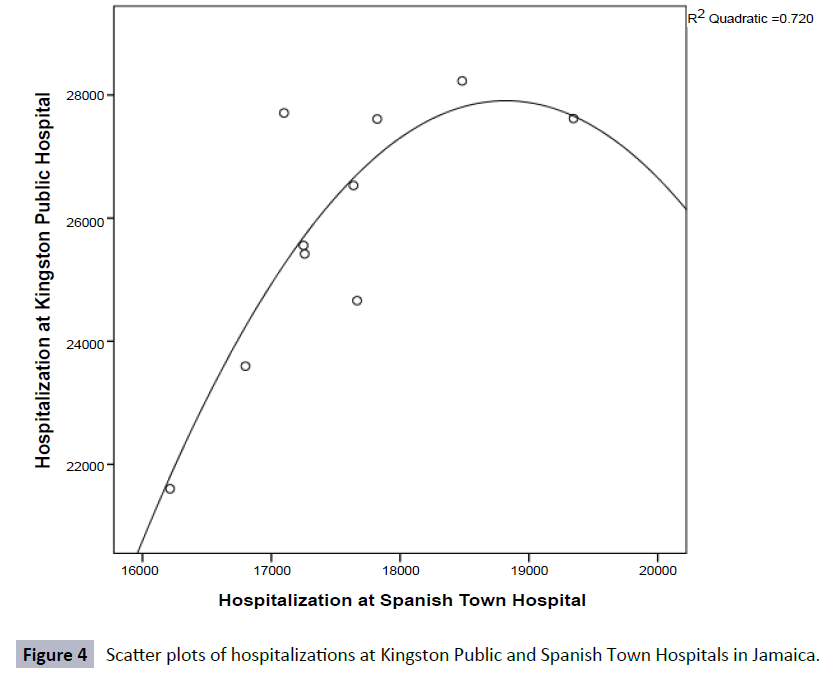
Figure 4: Scatter plots of hospitalizations at Kingston Public and Spanish Town Hospitals in Jamaica.
Figure 4 depicts a scatter plot of hospitalizations at Kingston Public and Spanish Town hospitals in Jamaica super-imposed at 2-degree polynomial function (concave downwards). The general increasing rate between hospitalization at Kingston Public and Spanish Town hospitals is observed in the graphical presentation of the scatter points.
Discussion
With Kingston Public Hospital being Jamaica’s national trauma center and the fact that many health care services are exclusively provided therein, patient-sharing is nothing new between many other hospitals and K. The current study has provided actual values to a concept that is well known as well as underresearched in Jamaica. Empirical evidence emerged from this study that showed that patient-sharing was the highest during the Chikungunya virus outbreak. It can be inferred from this study that communicable diseases outbreak will result in exponential rise in attendance at A&E across Jamaica, hospitalizations and that this will translate into high patient-sharing was recorded between K and SPH. There are many accounts of the rise in incidence of hospitalization among the populace following the outbreak of the Chikungunya virus [35-37]. Over the 10- year period for this study, in 2014, Kingston Public Hospital recorded the largest percentage hospitalization of patients and saw the greatest percentage patient-sharing between itself and Spanish Town (30.1%). Such statistics provide for the increase in hospitalization in Jamaica as the Chikungunya virus had become an epidemic [37] and this was translating into increased health care demand, particularly for K. Clearly both K and SPH were experiencing increases in in-patients, hospitalization and dual patient hospitalizations.
In all the cases, there were dual effects unfolding as inelastic complementary, inelastic substitution effects as well as elastic complementary and elastic substitution effects. Furthermore, there were occasions in which hospitalization at Kingston Public Hospital highly responded to admissions at Spanish Town Hospital, for 2007, 2009, 2010, 2011, and 2012. In the same depth, high patient-sharing occurred in 2007, 2009 and 2011. It should be noted here that patient-sharing between the two hospitals happened in 2014 during the outbreak of Chikungunya virus (ƞ was positive)-Southern Regional Health Authority (SRHA) [7]; Christmas, Palmer, and Mansingh [35].
The consequences associated with of the political policy directives as it relates to health care were captured in the data. In 2008, the government of Jamaica removed user fees from public hospitals and it can inferred from the current findings that rise in attendance at A&E departments in government hospitals was owing to and not limited to change in the political policy. It should be noted that Kingston Public Hospital saw an 8.3% rise in hospitalization compared to a 2.7% rise at Spanish Town Hospital. Generally, over the 10-year period, the largest rise in attendance at A&E departments occurred one year following the policy change in user fees. At that time patient-sharing was the highest over the 10 years of hospitalization at both health institutions.
For decades, Jamaicans have been lamenting their dissatisfaction with the services given the dire state of the health care system with the shortage in equipment and staffers [18,21-23,24-27,38]. The public debates were sometimes explosive however; there was no formal national probability research to describe the population’s dissatisfaction with the various public institutions in the society. The advent of social media has provided an avenue for public opinion and the feedback tends to be negative. In 2007, a national probability cross-sectional survey was conducted by Powell, Bourne and Waller and it was revealed that the Jamaican health care system was ranked as the eighth of 20 national problems identified by the sampled respondents. This fueled a rationale for the need to have public sector reform of the health care system. In September 2007, the health care system in Jamaica began a transformation process based on a mandate from the government to change the health system in keeping with a 21st standards, even though regionalization of public hospitals began in 1997 [39].
The island is divided into four health regions with each region being managed by a board and operated a set of hospitals. The board is totally responsible for the management and administration of the public hospitals in its region. The four regions are 1) South East Regional Health Authority (SERHA); 2) North East Regional Health Authority (NERHA); 3) Western Regional Health Authority (WRHA) and 5) Southern Regional Health Authority (SRHA). There are 23 government hospitals in Jamaica, with the University Hospital of the West Indies being the only quasi-government institution. The Kingston Public Hospital is the only national trauma hospital in the national and it is the largest trauma hospital in the English-Speaking Caribbean. Within the context of the nature of Kingston Public hospital, many patients are sent there for health care. This paper found that patient-sharing is occurring between Kingston Public and Spanish Town hospitals In Jamaica.
The issue of patient-sharing is a widely practiced phenomenon around the globe [28-30]. Some health care institutions do not encourage or want to support patient-sharing because it is said to expose patients to hospital-infections [40-44]. While the reality of hospital-infections is a part of patient-sharing [45-50], some patients in Jamaica must be transferred to Kingston Public hospital if there is a specialized trauma issue. Patient-sharing cannot be avoided between public hospitals in Jamaica, especially between the national trauma institute and other hospitals.
Patient-sharing is a staple between Kingston Public and Spanish Town hospital in Jamaica with at least 12% of admitters being transferred between them both. This study unearthed that during a period of national virus outbreak, for example the Chikungunya virus in 2014, patient-sharing can increase up to 30% which is unprecedented in the 10-year period of this research. Over the 10-year studied period, the average patient-sharing rate was 17.8%, with highest rate being in 2014 during the Chikungunya virus when admission was the highest at Kingston Public and second highest at Spanish Town Hospital. During the outbreak of the Chikungunya virus, patient-sharing stood at the most between the two government hospitals. Such findings support the claim that Kingston Public is national trauma institution for Jamaica.
This paper went further than merely describing patient-sharing to empirically establish a response-ability of the institutions to patient-sharing, the extent of patient-sharing during a national outbreak of a virus, and to establish a patient-sharing function. It was discovered that there are periods in which there was a high response-ability to patient-sharing and that patientsharing between Kingston Public and Spanish Town Hospitals is a non-linear function, suggesting that health planning and administration must take into consideration the responsivity of the patient-sharing as outside customer dissatisfaction will rise to unprecedented level. Such realities will place additional stressors on the national trauma centre if responsiveness is not planned for when implementing new policies. A platform is now set to further explore patient-sharing in Jamaica. Without an understanding of the extent of this phenomenon as well as the likelihood of this occurring temporally and spatially, health care administration will continually face significant shortfall. Customer dissatisfaction with the health care system in Jamaica is partly owing to the imperfect information on patient-sharing that obtains in the health sector. This raises the concern of unintended consequences associated with changes in government policy, example no user fees and the strain on already inadequate resources.
The resultant effect of high stressors associated with the new government policy (i.e., no user fees) placed on nurses has seen increased fatigue, physical illness (inclusive of. back pain and burn out), frustrations and absenteeism among nurses at various government hospitals owing to an influx of patients. Studies have empirically established that ‘burnout’ is a feature of high stress jobs including nursing [51-54], with no information on increased patient-sharing because of policy changes the health care sector is left to languish in the interim. The current work shows that there was a complementary effect between hospitalization at Kingston Public and Spanish Town Hospitals in 2009 after the introduction of user fees. The complementary effect represents patient-sharing and that no user-fee had greater effect on patient-sharing than the outbreak of a disease like Chikungunya virus.
Given the recent changes in the healthcare delivery landscape in coupled with resource constraints there is a continued disproportionate burdening of the already fraught foundation as it relates to care and planning. As evidenced by the study, although there are increases in the hospital visits and hospitalization there was no presentation of an increase in staff to manage this workload. This suggested that patients were likely to go without the required care or could receive sub-optimal medical services. While it is necessary to highlight these disparities, it is not sufficient as further examination and actions must be taken before critical conditions reach a crisis state. Policy makers, government officials and health care professional must be cognizant of the need to act with some sense of urgency to address the critical concerns. Through proper planning and the implementation of appropriate systems changes in policy directives or virus outbreaks will lead to increased access to relevant medical services however there will be corresponding effective sector-wide response resulting in improved health outcomes.
Assessment of the location of the hospitals, in proximity to the population served the size and types of services provided and the change in patients’ visits and hospitalization over time is paramount to ensure the needs of the population are met. Furthermore, it would provide the data needed to respond more readily to disease outbreaks or other public health emergencies. Patients should have the ability to access services and be provided with the appropriate medical intervention when sought. This current study points to the lack of accurate data to support the planning for health care and delivery of such. In the absence of data to demonstrate where there are gaps in the system, it becomes difficult to implement and support policies that will have far reaching impact on the human and financial resources of the sector especially within the context of resource insufficiency.
It is also crucial to take into consideration the shift in population (urban vs. rural), health care needs, population age, reduction in specialty services and unanticipated public health concerns in order to plan more effectively and improve delivery of medical services to patients. Although it will take time and effort to address the concerns raised as they relate to health care planning, and the coordination of services to patients, the current state of the infrastructure must be at the fore as health care systems especially in small island developing states can quickly become overwhelmed by the increased risk of chronic diseases due to their outdated systems and structure.
In addition to planning the delivery of services to patients, health care professionals and policies makers should seek ways to improve communication within and across health care institutions and decide on the frequency of such communication [55]. With the increase in electronics these institutions can create tools to leverage the technology to improve the exchange of information more efficiently. Kingston Public hospital is a national referral trauma centre, which is the case in other nations [55], and it for this reason why information is critical to effective health care management. This study, therefore, provides germane information from an empirical perspective on the matter of patient-sharing between Kingston Public and Spanish Town hospitals that can be used for policy and research framework.
Conclusion
It is clear that more robust planning and collaboration between and across hospitals can help alleviate some of the concerns raised in this study. Where possible, more integrated planning that utilizes the skills of researchers and which examines the ability to shift patient load to help in balancing resources to deliver more timely care is needed.
As evident in the study findings, small percentage change in hospitalizations usage in major hospitals, over a short period of time can increase the staff’s workload and burden the already constrained resources. The lack of integrative planning bolstered by evidence based research to inform policies can result in increased customer dissatisfaction which proves to be counter-productive to the goals of the policies. Furthermore, tools are needed to assist with the implementation and sharing of information within the health care system in a more timely and efficient manner. Additional research is required, however, to pinpoint specific actions required to improve health care planning and sharing of information and data across institutions.
Conflict of Interests
The researchers have no conflict of interest to report at this time.
References
- Agarwal R, Green R, Agarwal N, Randhawa K (2016) Management practices in Australian healthcare: can NSW public hospitals do better? Journal of Health Organization and Management 30: 331-353.
- De Vos P, Ordunez-Garcia P, Santos-Pena M, Van der Stuyft P (2010) Public hospital management in times of crisis: lesson learned from Cienfuegos, Cuba (1996-2008). Health Policy 96: 64-71.
- Cunningham A (2015) From Chik-V to Zika: Jamaica on high alert for another mosquito borne disease. Kingston: Jamaica Gleaner.
- Gammon K (2014) The cost of chikungunya to Jamaica. Kingston: Jamaica Observer.
- Jamaica Observer (2014a) Chikungunya has been the beast of 2014. Kingston: Jamaica Observer.
- Seiveright D (2014) Chikungunya havoc in Jamaica. Kingston: Jamaica Gleaner.
- Southern Regional Health Authority (2014) Chikungunya virus in Jamaica. Kingston: Southern Regional Health Authority.
- Hall J, Wynter E (2003) Kingston Public Hospital: the high seat of medicine in Jamaica. Kingston: Pelican Publishers.
- Jamaica Gleaner (2016a) JCF increases efforts to dismantle spanish town gangs. Kingston: Jamaica Gleaner.
- Jamaica Gleaner (2016b) Police monitoring spanish town as tension brews among gangs. Kingston: Jamaica Gleaner.
- Jamaica My Way.com (2009) The ghetto in spanish town, Jamaica.
- Jamaica Observer (2013) Police take back spanish town, murders down, gangs in retreat: residents happy, want police to stay in spanish town communities. Kingston: Jamaica Observer.
- Love Jamaica (2015) Gang wars intensify in spanish town, “Donkey” killed.
- Robinson C (2010a) Pastor among 2 killed in spanish Town gang feud. Kingston: Jamaica Observer.
- Robinson C (2010b) Two dead in spanish town gang war. Kingston: Jamaica Observer.
- Turner R, McLeod D (2016) Thugs battle for gang control: six killed in internal conflict. Kingston: Jamaica Star.
- Walters B (2015) Silent night in several spanish town communities. Kingston: Jamaica Observer.
- Haye WDL, Alexis S (2012) The impact of a no-user-fee policy on the quality of patient care/service delivery in Jamaica. West Indian Med J 61: 168-173.
- Hibbert K (2015) Doctors blame lack of resources for poor health care. Kingston: Jamaica Observer.
- United Nation Population Fund (UNFPA) (2016) Country profile: Jamaica.
- Carmen C, Bench NS (2015) The health workforce in latin america and the caribbean an analysis of Colombia, Costa Rica, Jamaica, Panama, Peru, and Uruguay.
- Jamaica Gleaner (2015a) Fixing health: The brain drain of our health professionals. Kingston: Jamaica Gleaner.
- World Health Organization (WHO) (2013) Jamaica: country corporate strategy at a glance.
- Brown P (2003) The health service brain drain: what are the options for change? Immunization Focus pp: 6-8.
- Buchan J, Dovlo D (2004) International recruitment of health workers to the UK: A report for DFID. Department for International Development, DFID Health Systems Resource Centre, London.
- Buchan J, Sochalski J (2004) The migration of nurses: trends and policies. Bulletin of the World Health Organization 82: 587-594.
- Buchan J, Parkin T, Sochalski J (2003) International nurse mobility: trends and policy implications. Report funded by royal college of nursing, World Health Organization and International Council of Nurses. Geneva, WHO.
- Barnett ML, Christakis NA, O’Meally J, Onnela JP, Keating NL, et al. (2012) Physician patient-sharing networks and the cost of intensity of care in US hospitals. Med Care 50: 152-60.
- Society for Healthcare Epidemiology of America (2009) Extensive patient sharing among hospitals could impact spread of infectious diseases. ScienceDaily.
- Chang HH, Donker T, Worby C, Feil EJ, Hanage WP, et al. (2016) Identifying the effect of patient sharing on between-hospital genetic differentiation of methicillin-resistant Staphylococcus aureus. Genome Medicine 8: 18.
- Hill RC, Griffiths WE, Judge GG (2001) Undergraduate econometrics (2nd edn.) Mascheuchet: John Wiley and Sons, Inc.
- Mamingi N (2005) Theoretical and empirical exercises in econometrics. Kingston: University of the West Indies Press.
- Wooldridge JM (2006) Introductory econometrics: A modern approach (3rd edn.) Ohio: Thomson.
- Harcourt BE (2011) An institutionalization effect: the impact of mental hospitalization and imprisonment on homicide in the United States, 1934-2000. The Journal of Legal Studies 40: 39-83.
- Christmas M, Palmer W, Mansingh A (2015) Orthopaedic manifestations of the Chikungunya virus in Jamaica. West Indian Medical Journal.
- Crossan A (2014) Jamaica declares a state of emergency to try to stop the spread of painful chikungunya virus.
- Jamaica Observer (2014b) Chikungunya now an epidemic in the Caribbean.
- Jamaica Gleaner (2015b) Nursing calamity: specially trained nurses leaving Jamaica in droves. Kingston: Jamaica Gleaner.
- Health Sector Task Force (2007) A healthy Jamaica in a healthy world. Kingston: Jamaica.
- Chang HH, Dordel J, Donker T, Worby CJ, Feil EJ, et al. (2016) Identifying the effect of patient sharing on between-hospital genetic differentiation of methicillin-resistant Staphylococcus. Genome Med 8: 18.
- Gordon HS, Rosenthal GE (1996) Impact of interhospital transfers on outcomes in an academic medical center. Implications for profiling hospital quality. Med Care 3494: 295-309.
- Huang SS, Avery TR, Song Y, Elkins KR, et al. (2010) Quantifying interhospital patient sharing as a mechanism for infectious disease spread. Infect Control Hosp Epidemiol 31: 1160-9.
- Lee BY, Bartsch SM, Wong KF, Singh A, Avery TR, et al. (2013) The importance of nursing homes in the spread of methicillin-resistant Staphylococcus aureus (MRSA) among hospitals. Med Care 51:205-15.
- Page D (2009) Patient care. Spread of infectious diseases may run high with patient sharing. Hosp Health Netw 83: 12.
- Collins AS (2016) Preventing health care-associated infections. patient safety and quality: An Evidence-Based Handbook for Nurses 2: 547-575.
- Donker T, Wallinga J, Slack R, Grundmann H (2012) Hospital networks and the dispersal of hospital-acquired pathogens by patient transfer. Plos.
- Eber MR, Laxminarayan R, Perencevich EN, Malani A (2010) Clinical and economic outcomes attributable to health care-associated sepsis and pneumonia. Arch Intern Med 170: 347-353.
- Livshiz-Riven I, Borer A, Nativ R, Eskira S, Larson E (2015) Relationship between shared patient care items and healthcare-associated infections: a systematic review. Int J Nurs Stud 52: 380-392.
- Laxminarayan R (2012) Crafting a system-wide response to healthcare-associated infections. PNAS 109: 6364-6365.
- US Department of Health & Human Services (2016) Information for patients.
- Jennings BM (2008) Work stress and burnout among nurses: role of the work environment and working conditions. patient safety and quality: An Evidence-Based Handbook for Nurses 2: 137-158.
- Bakker AB, Demerouti E, Sanz-Vergel AI (2014) Burnout and work engagement: The JD-R approach. Annual Review of Organizational Psychology and Organizational Behavior.
- Bakker AB, Le Blanc PM, Schaufeli WB (1997) Burnout contagion among nurses who work at intensive care units. Paper presented at the 5th european conference on organizational psychology and health care. Utrecht, The Netherlands.
- Bakker AB, Le Blanc PM, Schaufeli WB (2005) Burnout contagion among nurses who work at intensive care units. J Adv Nurs 51: 276-287.
- Bernardes A, de Oliveira Cecilio LC, Évora YDM, Gabriel CS, Carvalho MB (2011) Collective and decentralized management model in public hospitals: perspective of the nursing team. Revista Latino-Americana de Enfermagem 19: 1003-1010.

