Mathew AL1*, Cherian SA2 and Joseph BB3
1Department of Oral Medicine and Radiology, Pushpagiri College of Dental Sciences, India
2Department of Periodontics, Pushpagiri College of Dental Sciences, India
3Department of Oral Medicine and Radiology, Azzezia College of Dental Sciences, India
*Corresponding Author:
Mathew AL
Associate Professor, Department of Oral Medicine and Radiology,
Pushpagiri College of Dental Sciences, Kerala, India
Tel: +91 8547431225
E-mail: drmathewdan@yahoo.co.in
Received Date: October 01, 2018; Accepted Date: October 22, 2018; Published Date: October 27, 2018
Citation: Mathew AL, Cherian SA, Joseph BB (2018) Styloid Process Elongation with Temporomandibular Disorders: Clinical and Radiographic Aspects. J Ora Med Vol.2 No.3:9.
Keywords
Temporomandibular joint; Styloid process; Eagle’s syndrome; Orofacial pain
Introduction
“Temporomandibular disorders or dysfunction (TMD) is a collective term that encompasses many clinical problems involving the masticatory muscles, the temporomandibular joint (TMJ) and associated structures or both” [1]. Patients with TMD most commonly present with signs and symptoms of pain in the TMJ region or preauricular region, limited mouth opening and mandibular movements, joint sounds, headaches, referred pain, vertigo, tinnitus, and earache. There is an increasing number of patients with orofacial pain and temporomandibular disorders. Studies have shown that 40-75% of the population has at least one sign of TMD and 33% has at least one symptom [2,3].
Eagle’s syndrome consists of anatomical changes in the styloid process or stylohyoid ligament, which can lead to clinical manifestations similar to TMD [4]. However, not all morphological changes in the styloid process produce painful symptoms. Thus, diagnosis of Eagles syndrome resulting from elongated styloid process (>30 mm) is difficult and most clinicians have difficulty in diagnosing and ultimately attribute it to some other cause [5]. Misdiagnosis of TMD can hinder treatment success since TMD is treated with conservative therapy [6,7], while Eagles’ syndrome is treated with surgical excision with intraoral or extraoral approach [8-10]. The aim of our study was to investigate the possible association between the intensity of the TMD symptoms and styloid process elongation by analysing the styloid process length from measurements obtained from panoramic radiographs.
Methodology
A cross-sectional study was conducted among patients (n=15), aged 20-65 years, who visited the OPD of the Oral Medicine and Radiology department of a dental school in Kerala, South India, over a period of 3 months presenting with TMD symptoms. Consent was obtained from each patient before the study. Patients with orofacial pain with symptoms of TMD for more than 3 months were included in the study. Pregnant women and patients who have undergone radiation treatment for malignancy because of the possible risk for radiation were excluded from the study.
The clinical and radiographic examinations were done by a single trained examiner to reduce bias and obtain reproducible results and reliability. Patients were evaluated for pain using VAS (visual analogue scale) for assessing the degree of pain for the common symptoms of TMD in Eagles syndrome like orofacial pain, headache, tinnitus, vertigo and dizziness. A scale of 0-3, 4-6, and 7-10 were given for mild, moderate and severe pain respectively. The length of the styloid process was measured with the help of a digital panoramic radiograph. The images were calibrated properly by adjusting the contrast and brightness for good visualization to obtain accurate measurements.
In our study, only the length of the right styloid process was taken into consideration. The panoramic radiograph was zoomed to identify the region of the styloid process. A line was drawn from the lowest point of the external acoustic meatus to the apex of the process and this distance was measured to obtain the length of the styloid process. The association of the elongation of the styloid process and the intensity of pain in patients (groups of VAS) with TMD symptoms was done using Fishers test.
Results
The mean age of the patient was 42.7 ± 13.4 of which 60% were females and 40% males. The styloid process was elongated in 53.3%, the mean length and SE being 27.2 ± 1.51 (Table 1). Mild and moderate intensity of pain measured by VAS was present in 6.7% and 46.7% of the patients with styloid elongation respectively Table 2. Orofacial pain (93.3%) was the most common symptom followed by head ache (20%) tinnitus (13.3%), vertigo and dizziness (6.7%), as shown in Figure 1. The distribution of the symptoms according to VAS is given in Figure 2. Among the 93.3% of the patients who had orofacial pain, 46.7% had mild pain and 53.3% had moderate pain according to the VAS scale. The association between the intensity of pain and length the styloid process by Mann Whitney U test was highly significant (p=0.028), as shown in Table 1 and Figure 3. Mantel-Haenszel Chi-square was done to stratify and analyse the effect of age and gender in the relation of VAS and presence of elongation and found to be significant, p=0.02 and 0.05 respectively Tables 3 and 4.
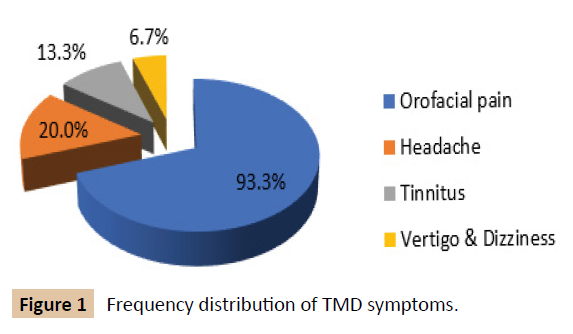
Figure 1: Frequency distribution of TMD symptoms.
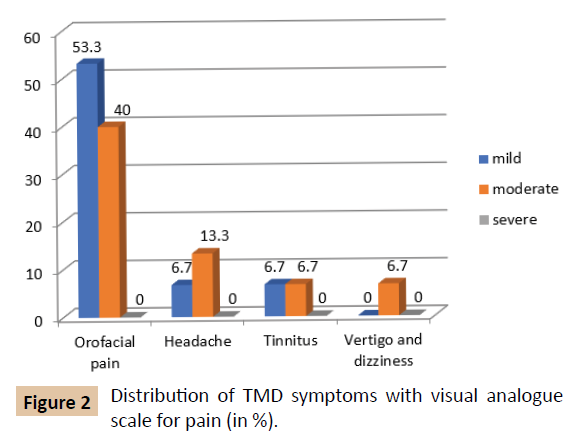
Figure 2: Distribution of TMD symptoms with visual analogue scale for pain (in %).
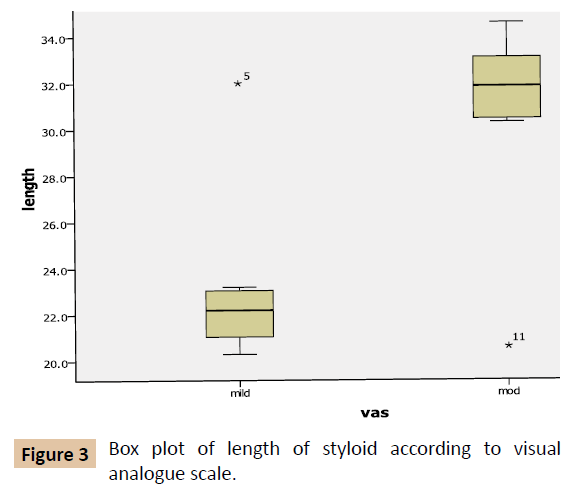
Figure 3: Box plot of length of styloid according to visual analogue scale.
Table 1: Descriptive statistics of styloid elongation according visual analogue scale.
| Visual Analogue Scale |
Mean±SE |
Median |
Range |
P value |
| Mild |
23.24 ± 1.51 |
22.2 |
20.3-32.0 |
0.028 |
| Moderate |
30.75 ± 1.53 |
31.8 |
20.6-34.6 |
Table 2: Distribution of visual analogue scale with presence of styloid elongation.
| Presence of styloid elongation |
Visual Analogue Scale |
| Mild (%) |
Moderate (%) |
| Present |
6.7 |
46.7 |
| Absent |
40 |
6.7 |
Table 3 Effect of age in the relation of VAS and presence of elongation.
| Age group |
VAS |
Presence of elongated styloid process |
p-value |
| Present (%) |
Absent (%) |
| >40 years |
Mild |
1 (6.7) |
2 (13.3) |
0.02 |
| Moderate |
3 (20) |
0 |
| <40 years |
Mild |
0 |
4 (26.7) |
| Moderate |
4 (26.7) |
1 (6.7) |
Table 4 Effect of gender in the relation of VAS and presence of elongation.
| Gender |
VAS |
Presence of elongated styloid process |
p-value |
| Present (%) |
Absent (%) |
| Female |
Mild |
0 |
2 (13.3) |
0.05 |
| Moderate |
6 (40) |
1 (6.7) |
| Male |
Mild |
1 (6.7) |
4 (26.7) |
| Moderate |
1 (6.7) |
0 |
Discussion
In our study, we found that the association between the length of the styloid process and the intensity of the symptoms of TMD was statistically highly significant. Studies by Guimaraes et al., Zake et al. and Krenmair et al., showed that the patients with TMD and elongation of styloid process to have a prevalence of 5.5%, 27% and 76% respectively, but no statistically significant association was found [11-14]. The mean length of the styloid process was 27.2 ± 5.6, which was similar to a study done by Machado de et al., but other studies showed a variation of 15.2 to 60 mm [14,15]. The elongated styloid process was found in 53.3% of the patients in the mean age of 42.7 ± 13.4 with a higher female predilection. The age was similar in almost all the previous studies. Guimararaes et al., show a higher female prevalence, where as other studies show a higher male prevalence [11,16-19]. The disagreement in the distribution of gender can be due to the difference in sample size.
The most common symptom was orofacial pain (93.3%), head ache (20%) tinnitus (13.3%), vertigo and dizziness (6.7%). Similar results are found in the studies by Cooper and Kleinberg and others in the case of orofacial pain [20,13]. These studies also had higher prevalence of headache, tinnitus, vertigo and dizziness compared to our study. The prevalence of tinnitus and dizziness in patients with TMD varies from 28-76% and 5-70% respectively [21,22].
In our study, we used digital panoramic radiograph to evaluate the length of the styloid process. Several authors have used digital panoramic radiograph for observation and analysis because of its ease to perform and availability to the patients [23-26]. Spiral CT with subsequent 3D reconstruction is considered as the most effective method for exact determination of the length of the styloid process and temporomandibular joint defects [27-29]. Studies with larger sample size are required to substantiate the association between intensity of the symptoms of TMD and the length of the styloid process.
Conclusion
Diagnosis is the pillar of any medical treatment. As our study shows a significant statistical association between the TMD symptoms and the length of the styloid process, a good clinical knowledge of the condition is required for proper diagnosis and avoidance of unnecessary intervention of multiple medical specialities.
Acknowledgement
The authors would like to thank Ms. Nisha Kurian, Asst. Professor, Biostatistics, Pushpagiri Institute of Medical Sciences and Research Centre for her contribution to this research.
References
- McNeill CH (1993) Temporomandibular disorders, guidelines for classification, assessment and management. The American Academy of Orofacial Pain. Chicago: Quintessence Publishing, pp: 247-248.
- Atsu SS, Ayhan–Ardie F (2006) Temporomandibular disorders seen in rheumatology practices: A review. Rheumatol Int 26: 781-787.
- De Leeuw R (2008) Orofacial pain: guidelines for assessment, diagnosis and management. The American Academy of Orofacial Pain. Chichago: Quintessence Int 4: 2-5.
- Hotta PT, Hota TH, Batagolion C, Pavao RF, Siessere S, et al. (2008) Bite force in temporomandibular dysfunction (TMD) and healthy complete denture wearers. Braz Dent J 19: 354-357.
- Chickooree D, Ram V (2014) Eagle’s syndrome – View from the General Practitioners Perspective. Clinical Medicine and Diagnostics 4: 9-13.
- Balcioglu HA, Kilic C, Aykol M, Ozan H, Kokten G (2009) Length of styloid process and anatomical implications for Eagles syndrome. Folia Morphol 68: 265-270.
- Zaki HS, Greco CM, Rudy TE, Kubinski JA (1996) Elongated styloid process in a temporomandibular disorder sample: prevalence and treatment outcome. J Prosthet Dent 75: 399-405.
- Gozil R, Yener N, Çalguner E, Araç M, Tunç E, et al. (2001) Morphological characteristics of styloid process evaluated by computed axial tomography. Ann Anat 183: 527-535.
- Trevisan DRS (2002) Analysis of aspects of the stylohydoid complex in panoramic radiography. J Bras Oclus ATM & Dor Orofac 2: 105-115.
- Camarda AJ, Deschamps C, Forest D (1989) Stylohyoid chain ossification: a discussion of etiology. Oral Surg Oral Med Oral Pathol 67: 508-514.
- Guimarães SMR, Carvalho ACP, Guimarães JP, Gomes MB, Cardoso MMM, et al. (2018) Prevalence of morphological alterations of the styloid process in patients with temporomandibular joint disorder. Radiol Bras 39: 407-411.
- Krennmair G, Piehslinger E (1999) The incidence and influence of abnormal styloid conditions on the etiology of craniomandibular functional disorders. Cranio 17: 247-253.
- Andrade KM, Almeida RC, Aranha WPC, Oliveira MM (2012) Styloid process elongation and calcification in subjects with tmd: clinical and radiographic aspects. Braz Dent J 23: 443-450.
- Balbuena L, Hayes D, Ramirez SG, Johnson R (1997) Eagle´s Syndrome (elongated styloid process). South Med J 90: 331-334.
- Gozil R, Yener N, Calguner E, Arac M, Tunc E, et al. (2001) Morphological characteristics of styloid process evaluated bycomputerized axial tomography. Ann Anat 183: 527-535.
- Hernandez C, Rodriguez MM, Sano R, Vargas S, Monasterio MV (2000) Síndrome de Eagle: A propósitode un caso. Acta Otorrinolaringológica 12: 57-62.
- Eagle WW (1937) Elongated styloid process. Report of two cases. Arch Otolaryngol 25: 584-587.
- Aral IL, Karaca I, Gungor N (1997) Eagle’s syndrome masquerading as pain of dental origin. Aust Dent J 42: 18-19.
- Mathew AL, Cherian SA, Joseph BB (2006) Styloid Process Elongation and Calcification Patterns in a South Kerala Population - Radiographic Aspects. J Ora Med 1: 11-14.
- Cooper BC, Kleinberg I (2007) Examination of a large patient population for the presence of symptoms and signs of temporomandibular disorders. Cranio 25: 114-126.
- Camparis CM, Formigoni G, Teixeira MJ, De Siqueira JT (2005) Clinical evaluation of tinnitus in patients with sleep bruxism: prevalence and characteristics. J Oral Rehabil 32: 808-814.
- Urban VM, Neppelenbroek KH, Pavan S, Alencar FGP, Jorge JH, et al. (2009) Association between otalgia, tinnitus, vertigo and hypoacusia, with temporomandibular disorders. RGO 57: 107-115.
- Rodrigues JRC, Chilvarquer F (1991) Clinical and radiographic evaluation of patients with elongated and calcified styloid apophysis with painful TMJ dysfunction. Annals SBPqO 7: 57.
- Noronha MJR, Gandelmann I, Araújo Jr GP, Shunemann WG (1987) Stretching of the styloid process. Eagle syndrome. Rev Bras Otorrinolaringol 53: 60-63.
- Kings SSPM, Carvalho PL, Reis HSM (2001) Elongated styloid process - report of two cases. J Bras Oclus ATM & Dor Orofac 1: 296-300.
- Slavin KV (2002) Eagle syndrome: entrapment of the glossopharyngeal nerve? Case report and review of the literature. J Neurosurg 97: 216-218.
- Savranlar A, Uzun L, U?gur MB, Ozer T (2005) Three-dimensional CT of Eagle’s syndrome. Diagn Interv Radiol 11: 206-209.
- Basekim CC, Mutlu H, Gungor A (2005) Evaluation of styloid process by three-dimensional computed tomography. Eur Radiol 15: 134-139.
- Heitz C, Rocha JRM, Souza PHC, Costa NP (1999) Atypical mineralization of the styloid complex: Case report. Rev Bras Prosthesis and Implant 6: 31-37.