Keywords
Lyme disease; Facial paralysis; Meningitis; Simultaneous Bilateral Facial Paralysis (SBFP)
Introduction
Unilateral facial paralysis is a relatively common diagnosis with an incidence of 20-25/100,000 people [1]. However, simultaneous bilateral facial paralysis (SBFP) is a rather uncommon condition and according to a research it occurs in 0.3-2% of cases presenting with facial palsy [2] and is defined as palsy affecting both sides of the face during a period no longer than 30 days [3]. Usual causes of Simultaneous Bilateral Facial Palsy include Head injuries, Bell’s palsy, Sarcoidosis, Lyme disease, and Guillain-Barré syndrome [4]. Bilateral facial paralysis is most often an associated finding in the symptom complex of any systemic disease, compared to unilateral facial palsy, where majority of cases occur because of Bell’s palsy. Since systemic diseases can present with bilateral facial paralysis as the first sign, therefore we recommend that all cases of simultaneous bilateral facial paralysis must be investigated thoroughly using laboratory as well as radiological evidence.
Post-traumatic bilateral facial nerve palsy is a rare entity and is usually associated with transverse fracture of the temporal bones in patients who have sustained a significant head injury [5]. Idiopathic Bell’s palsy is however a diagnosis of exclusion and is usually acute in onset [3] and unilateral but in rare cases may present as bilateral palsy. Sarcoidosis, on the other hand, is a systemic, chronic, granulomatous disease that mainly affects the lungs. Bilateral facial nerve involvement known as Heerfordt fever due to occult Sarcoidosis is an extremely rare phenomenon and can be the presenting complaint in a wide spectrum of the disease [6].
Case Report
Methods
A retrospective case review was carried out for patients presenting with simultaneous bilateral facial nerve palsy over a period of 2 years. Four cases which met the inclusion criteria were selected for evaluation, of which two cases were associated with Road traffic accidents, one with Bell’s palsy and one with Sarcoidosis. Inclusion criteria involved cases having simultaneous bilateral facial palsy involving the other half of the face within 30 days of onset. Cases having recurrent or alternating bilateral palsy were excluded.
Case presentation
1st Patient: A 32-year-old man (Figure 1) presented with sudden onset complete bilateral facial nerve palsy for 3 days. There were no associated complaints such as fever, rash, ear discharge, trauma or any other systemic illness. On examination, there was complete bilateral palsy, left side more than right, and loss of taste sensation on the anterior half of the tongue. The bilateral tympanic membrane was normal on otoscopy.
Figure 1: Patient presented with Bell’s palsy.
2nd Patient: A 35-year-old woman (Figure 2) presented with sudden onset bilateral facial nerve palsy for 1 day, associated with vague complaints of fatigue, excessive sleepiness, and weight loss, dryness of the eyes and mouth, and a dry cough. On otoscopy, bilateral tympanic membranes were normal. The patient’s hearing was normal.

Figure 2: Patient presented with Sarcoidosis.
3rd Patient: A 55-year-old man (Figure 3) was admitted to the casualty department after a road traffic accident (RTA) with associated head trauma and bilateral ear bleeding. The patient was examined and was diagnosed to have sudden onset posttraumatic bilateral facial nerve palsy. Otoscopy revealed Right haemotympanum with a normal Left tympanic membrane. Audiometry revealed bilateral conductive hearing loss (Right side more than Left).
Figure 3: Patient presented with Road traffic accident leading to bilateral facial palsy.
4th Patient: A 32-year-old man (Figure 4) presented with delayed onset complete bilateral facial nerve palsy following Head injury. Otoscopy revealed an intact tympanic membrane. There were no associated complaints of decreased hearing or vertigo.
Figure 4: Patient presented with road traffic accident developing delayed onset bilateral facial nerve palsy.
Investigations
1st patient: Pure tone audiometry (PTA) revealed normal hearing bilaterally with absence of stapedial reflex. Electroneuronography (ENoG) revealed bilateral facial weakness. Complete blood count, liver and renal function, erythrocyte sedimentation rate (ESR), serum titres of anti-EBV immunoglobulin, VDRL, Lyme titre, High resolution computed tomography scan of the temporal bone, Chest X-ray, and Serum ACE levels were all within normal limits.
2nd patient: ENoG revealed bilateral facial palsy (left side more than right). As the patient had associated complaints of dryness of the eyes and congestion, an ophthalmologic opinion was taken which revealed bilateral uveitis. Chest X-ray revealed bilateral hilar lymphadenopathy, and Serum ACE levels were elevated=380 Units (normal 44-113 Units). Complete blood count, Biochemistry, ESR, Serum titres of anti-EBV immunoglobulin, high resolution computed tomography scan of the temporal bone, and VDRL were all within normal limits.
3rd patient: The High resolution computed tomography scan of the temporal bone indicated bilateral longitudinal fractures involving the facial canals (Figure 5). ENoG revealed bilateral complete facial nerve palsy.
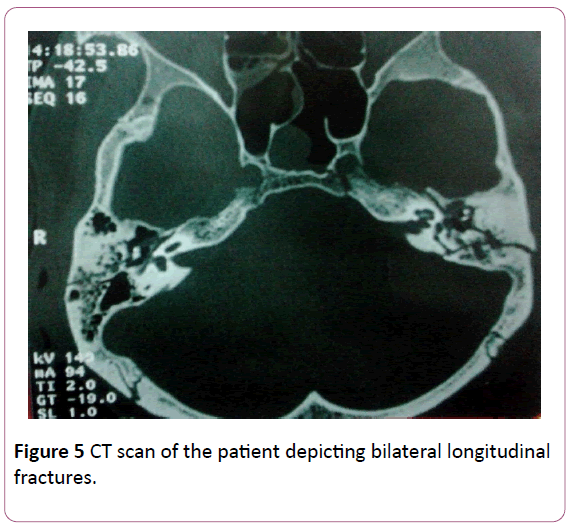
Figure 5: CT scan of the patient depicting bilateral longitudinal fractures.
4th patient: A High resolution computed tomography scan of the temporal bone revealed a longitudinal fracture involving the bilateral facial canals. ENoG was indicative of incomplete bilateral facial nerve palsy (Right side more than Left).
Treatment
1st patient was diagnosed to be suffering from bilateral Bell’s palsy and was treated with corticosteroids at a dose of 1 mg/kg body weight along with physiotherapy.
For 2nd patient a biopsy was taken from the lips and was indicative of Sarcoidosis. The patient was then treated with corticosteroids at a dose of 1 mg/kg body weight.
3rd patient was diagnosed with sudden onset post-traumatic bilateral facial palsy. He was operated for bilateral facial nerve decompression
4th patient was diagnosed with delayed onset post-traumatic bilateral facial palsy, and was treated conservatively with corticosteroids at a dose of 1 mg/kg body weight with regular physiotherapy.
Outcome
1st patient recovered completely after a period of 6 weeks.
2nd patient showed recovery of the bilateral facial nerves after 5 months of follow-up, but was complaining of uveitis for which she was under ophthalmological follow-up for a year.
3rd patient has been under regular follow-up for the past few years. Facial nerve recovered completely after 3 months of physiotherapy and surgery.
4th patients serial ENoG showed an improvement and he recovered completely.
Discussion
Bilateral simultaneous facial nerve palsy presents as one of the findings in the symptom complex of a systemic disease, many of which are potentially life threatening, and therefore this condition warrants an urgent treatment [7]. The aetiologies include congenital, infectious, traumatic, neurological/neuromuscular, vascular, autoimmune, idiopathic, iatrogenic as well as neoplastic, causes [8].
Idiopathic (Bell’s) palsy occurs with a frequency of 15-40/100,000 people [9]. It is acute in onset and is generally a diagnosis of exclusion. It is characterised by oedema of the nerves and is associated with numbness or pain in the ear, face, or neck in 50% of cases. The process is self-limiting, nonprogressive, non-life threatening, spontaneously remitting and most cases improve within 4-6 months. Not only thorough history, but complete physical examination along with laboratory investigations is needed to reach the diagnosis. Most patients presenting with Bell’s palsy respond extremely well to steroids and physiotherapy within a 6-month period [10]. The role of acyclovir in its treatment is still controversial [11]. Patients not responding to conservative management should be assessed for facial nerve decompression [12]. Although the role of surgery (facial nerve decompression) has remained controversial amongst some of the otologists; therefore we suggest that ENoG and the clinical course of paralysis are the best guidelines for selecting patients for facial nerve decompression.
We advocate surgery only if there has been 75-95% degeneration on serial ENoG within 2 weeks after the onset of paralysis, so as to preserve the remaining axons. Surgery is not advisable after 14 days, because the active viral disease has abated already and the early regeneration stage is beginning. Decompression must involve both the meatal and labyrinthine segments and is usually done via a middle cranial fossa approach [12].
Patients presenting with bilateral facial paralysis along with features of uveitis as well as parotitis should be assessed for Sarcoidosis (Heerfordt’s syndrome) [6]. In 1909, Heerfordt first described this syndrome which occurs mostly in the 2nd and 3rd decade and is of unknown aetiology. Early symptoms include mild fever with malaise, gastrointestinal disturbances, joint pains, night sweats and skin eruptions. However, the syndrome characteristically presents with uveitis, mild fever, enlargement of the parotid glands and cranial nerve paralysis (7th nerve being most common). The cause of palsy is evident from altered laboratory findings (increased ACE levels), detection of Hilar lymphadenopathy or diffuse pulmonary infiltrates on chest Xray; uveitis and chronic granulomatous infiltrates on biopsy of the involved tissues, i.e. cervical lymph node, salivary gland, lips or mucous membrane of the nasopharynx [3]. Microscopically, lesions consist of focal collections of epithelioid cells surrounded by lymphocytes. Patients with Sarcoidosis usually respond well with steroids within a time frame of four to six months. Steroid sparing drugs such as methotrexate, azathioprine, and cyclophosphamide have been described in the literature in past but till date their reports have been controversial [13].
Injury to the intratemporal facial nerve can be caused by temporal bone fractures which can be either longitudinal, transverse or mixed fractures. The incidence of longitudinal fractures is approximately 3-4 times higher than that of transverse fractures. However, facial nerve palsy occurs more commonly with transverse and most common site of injury being the geniculate ganglion [5]. Most cases of immediate onset post-traumatic facial palsy are associated with partial or complete nerve transaction and mandate an urgent exploration to preserve the nerve. On the other hand, most cases of delayed onset post-traumatic facial palsy are associated with concussion injury to the nerve resulting in an oedematous nerve and therefore the mainstay of treatment remains conservative [14]. These patients are treated with steroids along with physiotherapy. Regular ENoG not only helps in guiding treatment but can also be used to indicate early deterioration or improvement. According to Fisch an urgent surgical intervention should be performed within 3-4 weeks of traumatic facial nerve injury if the ENoG is indicative of 90% amplitude reduction within 6 days post injury [15]. These guidelines were later modified by Lieberherr and colleagues who recommended that surgery should be performed as soon as the patient’s condition permits in cases when ENoG is indicative of greater than 90% degeneration [16].
Apart from the above mentioned causes, there can be other causes of facial palsy such as Lyme disease, Guillain-Barré syndrome or infectious mononucleosis. Lyme disease is a multisystem illness caused by spirochetal infection by Borrelia burgdorferi which is transmitted by tick bites. Patients usually present with myalgia, erythema, and regional lymphadenopathy. A few may develop associated cranial nerve palsies [8]. Unilateral Facial nerve palsy has been reported to be associated with 11% of patients with Lyme disease compared to 30-40% of these cases which are associated with bilateral palsies [17].
Guillain-Barré syndrome is an acute inflammatory demyelinating polyradiculopathy. Although the aetiology of this condition is unknown, two out of every three patients with this condition have been associated with preceding viral infection 3-4 weeks before the onset of symptoms [17]. The diagnosis is made from cerebrospinal fluid (CSF) biochemistry showing increased levels of CSF protein without any corresponding rise in cell counts [8].
Infectious mononucleosis is caused by Epstein-Barr virus which can be accompanied by simultaneous bilateral facial nerve palsy sometimes. The syndrome is characterized by a prodrome of symptoms including headache, malaise, myalgia, fatigue, sore throat along with lymph node enlargement [3].
Conclusion
• Unilateral facial palsy is usually idiopathic or can occur after road traffic accidents, following chronic ear infections or viral infection leading to Bell’s palsy.
• Bilateral facial nerve palsy is rare and can be associated with life threatening systemic diseases.
• We reinforce the importance of considering a range of differential diagnosis as bilateral facial nerve palsy needs urgent intervention.
• These patients not only need thorough assessment but also laboratory and radiological investigations for evaluation of underlying cause and further management.
References
- George MK, Pahlor AL (1991) Sarcoidosis: A cause for bilateral facial palsy. Ear Nose Throat J 70: 492-493.
- Stahl N, Ferit T (1989) Recurrent bilateral facial palsy. J Laryngol Otol 103: 117-119.
- May M, Klein SR (1991) Differential diagnosis of facial nerve palsy. OtolaryngolClin North Am 24: 613-645.
- May M (1990) The facial nerve palsy. Progressive facial nerve palsy: A management dilemma. Am J Otol 11: 458-460.
- Hasso A, Ledington J (1988) Traumatic injuries of temporal bone. Otolaryngol Clin North Am 21: 295.
- Wilson HL (1957) Facial paralysis in the uveoparotid fever of Boeck’s sarcoid. Ann OtolRhinolLaryngol 66: 164-172.
- Kilic R, Ozdek A, Felek S, Safak MA, Samim E (2003) A case presentation of bilateral simultaneous Bell’s palsy. Am J Otolaryngol 24: 271-273.
- Price T, Fife DG (2002) Bilateral simultaneous facial nerve palsy. J LaryngolOtol 116: 46-48.
- Hauser WA, Karnes WE, Annis J (1971) Incidence and prognosis of Bell’s palsy in the population of Rochester, Minnesota. Mayo Clinic Proc 46: 258-264.
- Adour KK, Diamond CD (1982) Decompression of the facial nerve in Bell’s palsy: A historical review. Otolaryngol Head Neck Surg 90: 453-460.
- Adour KK (1991) Acute facial paralysis. In:Rakel RE, ed. Conn’s Current Therapy. Philadelphia, PA: Saunders 1991: 870-872.
- Hanner P, Anderson O, Frisen L (1987) Clinical observations of effects on CNS in patients with acute facial palsy. Arch Otolaryngol Head Neck Surg 113: 516-520.
- White ES, Lynch JP (2007) Current and emerging strategies for the management of sarcoidosis. Expert OpinPharmacother 8: 1293-1311.
- Kamerer D (1982) Intratemporal facial nerve injuries. Otolaryngol Head Neck Surg 90: 512.
- Fisch U (1980) Management of intratemporal facial nerve injuries. J Laryngol Otol 94: 129-134.
- Lieberherr U, Schwarzenbach D, Fisch U (1990) Management of severe facial nerve paralysis in the temporal bone - a review of 82 cases. Facial Nerve: Proceedings of the Sixth International Symposium on the Facial Nerve. Amsterdam:Kugler and Ghedini Publications 1990: 285-289.
- Arias G, Nogués J, Mañós M, Amilibia E, Dicenta M (1998) Bilateral facial nerve palsy: four case reports. ORL J OtorhinolaryngolRelat Spec 60: 227-229.