Keywords
Serum KIF5A; KIF18A; p53 Autoantibody; Biomarkers; Asbestos
Introduction
The WHO estimates that 125 million people are occupationally exposed to asbestos worldwide and OSHA has estimated that as many as 1.3 million workers in construction and general industry face significant exposures to asbestos on the job in the U.S. [1,2]. Asbestos exposure is known to result in a number of negative health effects, many of which have long latency periods of up to 20-40 years, including cancer, and there has been no evidence of a threshold for the carcinogenic effect of asbestos [3,4]. The WHO has also raised its estimates of the global burden of asbestos related disease to 107,000 annual deaths primarily from asbestos related lung cancer, mesothelioma, and asbestosis [1]. Given the large population occupationally exposed to asbestos, potential biomarkers of exposure and/or of early effect for cancer risk from asbestos could have a large effect on the burden of disease by identifying individuals at the highest risk for malignancy who could be targeted for more aggressive intervention. Based on prior studies, it was hypothesized that certain members of the Kinesin Family Proteins (KIFs) and p53 autoantibodies may be potential biomarkers of asbestos exposure and/or related cancer risk.
The kinesin superfamily of proteins (KIFs) currently includes 45 different proteins classified into 14 families [5]. KIFs are a conserved class of microtubule-dependent molecular motor proteins that have ATPase activity and motion characteristics. Different subtypes of KIFs may participate in different cellular functions, but KIF5s and KIF18s primarily participate in mitosis. While studies have not been reported identifying KIF18A and KIF5A in cell culture experiments as specific targets for asbestos interaction or effect, it is plausible that they could be affected by alterations induced by asbestos exposure in the other proteins that regulate mitosis. Abnormal kinesin expression can alter the equal distribution of genetic materials between daughter cells during cell mitosis. This may occur due to chromosome hyper condensation, aberrant spindle formation, anaphase bridges, defective cytokinesis, aneuploidy and mitotic arrest [6]. The resulting loss or gain of genetic material due to the dysfunctional mitotic process can lead to a number of defects in the daughter cells which can promote carcinogenesis and/or the progression of aggressive behavior of the corresponding tumor cells [7,8].
The TP53 tumor suppressor gene is the most common site identified for genetic mutations in human cancers, which often causes an increase in the stability of mutant p53 protein, leading to its accumulation in cancer cells [9,10]. These mutations can occur early in the carcinogenic process and often may have a molecular signature based on the type of cancer and exposure linked to that cancer, which could make p53 an attractive biomarker of early effect [9]. The inactivation of p53 proteins and accumulation of both mutant and wild type p53 proteins in the tissue and serum can lead to the production of p53 autoantibodies, and in fact there is a close correlation between serum p53 autoantibodies and p53 overexpression in corresponding tissues [11,12]. Serum p53 autoantibodies have been found in patients with a number of pre-malignant diseases and cancers and in workers exposed to occupational carcinogens including asbestos before any clinical evidence of malignancy [10,11,13-15].
This study examined the potential relationship of asbestos exposure to alterations in KIF5A and KIF18A serum concentrations and p53 autoantibody serum concentrations to determine if they may be potential biomarkers of asbestos exposure for purposes of early detection and prevention.
Methods
Cohort
Information and samples from asbestos-exposed workers and unexposed controls were provided by the University of Perugia Occupational/Environmental Medicine Clinic for the years 2007-2011. The asbestos-exposed workers were recruited by the Italian National Institute for Insurance against Accidents at Work (Istituto Nazionale per L’Assicurazione contro gli Infortuni sul Lavoro-INAIL). Information was collected on age, gender, years of asbestos exposure, and smoking history of these workers. They were evaluated for asbestos-related disease by chest radiography, spirometry and diffusion capacity (DLCO), and 198 of these exposed workers were deemed to not have evidence of disease. These patients had the following characteristics: average age=62 with a range=36-83 (1 in his 30s; 6 in their 40s; 52 in their 50s; 94 in their 60s; 38 in their 70s; 8 in their 80s); all white males; average asbestos exposure=26 years (range=11-38 years); 32% non-smokers, 49% ex-smokers, and 19% current smokers (52% of whom average 1-14 cigarettes/day, 40% of whom average 15-24 cigarettes/day, and 8% of whom average more than 24 cigarettes/day). During the same period, normal, healthy, workers without known asbestos exposure were recruited at the University of Perugia hospital and out-patient clinics and 164 were selected as controls based on similar age, gender, and demographic area. Information was also collected on their occupation and smoking history. Based upon occupational histories all were deemed to have had no likely exposure to asbestos or other workplace carcinogens. They had the following characteristics: average age=57 with a range=21-99 (7 in their 20s; 13 in their 30s; 35 in their 40s; 51 in their 50s; 13 in their 60s; 15 in their 70s; 23 in their 80s; 3 in their 90s); all white males; 34% non-smokers, 37% ex-smokers, and 29% current smokers (48% of whom average 1-14 cigarettes/day, 35% of whom average 15-24 cigarettes/day, and 17% of whom average more than 24 cigarettes/day).
Laboratory Procedures
Serum samples were thawed and analyzed for the presence of KIF5A and KIF18A proteins by commercially available ELISAs (LS-F8011 and LS-F8012; Life Span Biosciences, Seattle, WA). In both cases, the assays are quantitative sandwich ELISAs utilizing microtiter plates pre-coated with a monoclonal antibody specific for the particular KIF. After incubation of the sample, a biotin-conjugated polyclonal antibody specific for the particular KIF is added followed by avidin-conjugated horseradish peroxidase and 3,3’,5,5’-tetramethylbenzidine substrate solution. The color change is measured spectrophotometrically at 450 nm and is converted into the concentration of KIF in the sample by comparison to a standard curve generated from known concentrations of purified KIF protein (run in duplicate) on each plate. The KIF concentration of each sample/individual was then compared to a cutoff level to determine positive or negative status for altered protein concentrations. The optimal cutoff level for KIF5A and KIF18A protein concentrations was explored via several methods including: the mean KIF5A level among the unexposed individuals plus 2 standard deviations; the mean KIF18A level among the unexposed individuals minus 1 standard deviation, due to a large standard deviation (greater than half the mean value which would result in a negative concentration) among control KIF18A levels; the mean KIF18A level among the unexposed individuals plus 1 standard deviation; and empirically determined cutoffs utilizing ROC analyses. The direction of the cutoffs explored is due to the observed increase in serum KIF5A levels and decreased serum KIF18A levels observed in a subset of asbestos cancer patients from an occupationally exposed Finnish asbestosis cohort reported previously, as well as the observed increases in KIF18A expression reported in the literature above [16-20]. These assays have been demonstrated to be highly reproducible and to have high sensitivity (LLD<118 pg/mL) and specificity (no cross-reactivity between each specific KIF and known analogues). The manufacturer reported intra-assay coefficient of variation (CV) is <10% and inter-assay CV is <12%. Finally, from the ELISA results comparisons can be made between the KIF levels found in serum and exposure to asbestos as described below.
Serum samples were thawed and analyzed for the presence and concentration of p53 autoantibodies by commercially available ELISA (DIA-0302-1; Dianova, Hamburg, Germany). The quantitative assay utilizes microtiter plates pre-coated with recombinant human wild-type p53 protein. After incubation of the sample diluted 1:100, the plate is washed to remove any unbound material and a horseradish peroxidaseconjugated purified goat anti-human polyclonal antibody is added to the wells which binds to any captured human p53 antibody. Following incubation and a wash step a chromogenic substrate is added to the wells. The horseradish peroxidase catalyzes the conversion of the chromogenic substrate 3,3’, 5,5’-tetramethylbenzidine from a colorless solution to a blue solution (or yellow after the addition of hydrochloric acid stopping reagent), the intensity of which is proportional to the amount of human p53 antibody in the test sample. The color change is measured spectrophotometrically at 450 nm and is converted into the concentration of p53 antibody in the sample by comparison to a standard curve generated from known concentrations of purified anti-human p53 antibody (run in duplicate) on each plate. The p53 antibody concentration of each sample was then compared to a cutoff level calculated from the standard curve on each plate to determine positive or negative status for p53 autoantibody expression and also from empirically determined cutoffs utilizing ROC analyses. The calculated Intra-Assay CV was 6.87% and the calculated Inter-Assay CV was 22%. Finally, from the ELISA results comparisons can be made between the p53 autoantibody levels found in serum and asbestos exposure.
Data Analysis
Data management and statistical analyses were performed using Microsoft Excel 2010 and SAS version 9.4. Distributions of KIF5A, KIF18A, and p53 autoantibody levels (continuous) were evaluated for normality and Spearman correlations were assessed between the continuous biomarkers, continuous exposure (years) and age. Individuals with missing variables were dropped from the analysis. Mean levels of each potential biomarker were compared in relation to asbestos exposure via parametric and non-parametric analyses where appropriate as well as via receiver operating characteristic (ROC) analysis. ROC analysis is a method of analyzing the predictive or discriminatory performance of a potential biomarker or diagnostic test by plotting the sensitivity (true positive rate) against 1-specificity (the false positive rate) for a range of potential cut-points. From this plot one can determine the optimal cut point for each biomarker to differentiate between a binary outcome, in this case exposed and unexposed individuals, utilizing various methods including Youden’s statistic and Euclidian distance from the perfect classifier (point 0, 1) [21]. Univariate logistic regression models for each biomarker on exposure status were run for the ROC analysis. Multivariable logistic regression models were also run including all three biomarkers and the covariates of age and smoking status as well as interaction terms for each covariate and the potential biomarkers of interest to explore their association with exposure status. Additionally, KIF5A, KIF18A, and p53 autoantibody status (Positive/Negative) were each assessed as the outcome in separate logistic regression models (SAS Proc Logistic) based upon each subject’s status of asbestos exposure (Exposed/Unexposed) or alternatively based upon each subject’s duration of asbestos exposure (years). In each logistic regression model, we additionally explored the effects of age, smoking status (current/former/ never), and the other potential biomarkers.
Results
General descriptive statistics on the cohort including biomarker expression levels, asbestos exposure years, and the measured covariates of age and smoking status are presented in Table 1. KIF5A, KIF18A, and p53 autoantibodies were found to be log-normally distributed by statistical tests for normality including the Shapiro-Wilk (p<0.0001), Kolmogorov-Smirnov (p<0.01) and Anderson-Darling (p<0.005). Therefore potential differences in serum biomarker levels between exposed and unexposed individuals were assessed on log-transformed biomarker values and via the non-parametric Wilcoxon ranksum test. Exposed individuals were significantly older than control individuals (p<0.0001) and smoking status was also different between exposed and unexposed individuals (p=0.0335) (Table 1).
| |
Exposed (n=198) |
Unexposed (n=164) |
|
| Age (years) |
63.2 (8.6) |
57.2 (17.0) |
p<0.0001* |
| KIF5A (ng/mL) |
2.01 (2.1) |
1.02 (1.29) |
p<0.0001* |
| KIF18A (ng/mL) |
356.39 (157.57) |
470.13 (275.4) |
p=0.0008* |
| p53AAbs (U) |
0.04 (0.1) |
0.03 (0.09) |
p=0.766 |
| Asbestos exposure (years) |
25.96 (6.13) |
0 (0) |
- |
| Smoking |
- |
- |
p=0.0335* |
| Current |
37 (18.69%) |
42 (25.61%) |
- |
| Former |
95 (47.98%) |
52 (31.71%) |
| Never |
62 (31.31%) |
48 (29.27%) |
| Missing |
4 (2.02%) |
22 (13.41%) |
Age, KIF5A, KIF18A, p53AAbs, and Asbestos exposure are represented as: mean (standard deviation); Smoking Status represented as: n (%). p-values from Student’s T-test for Age, Wilcoxon rank-sum test for KIF5A, KIF18A, p53AAbs, and Chi squared test for smoking. *Indicates significant p<0.05.
Table 1: Serum KIF5A, KIF18A, p53 autoantibodies, asbestos exposure, age and smoking status of Italian workers.
Exposed individuals had significantly higher mean levels of KIF5A (p<0.0001), significantly lower mean levels of KIF18A (p=0.0008), but no difference in mean levels of p53 autoantibodies (p=0.766) in serum compared to the unexposed individuals in non-parametric Wilcoxon bivariate analyses. ANOVA results showed that smoking status was not significantly associated with KIF5A (p=0.6404) or p53 autoantibody serum concentrations (p=0.8294), but was associated with KIF18A serum concentrations (p=0.0386), with lower KIF18A concentrations in ex-smokers than current smokers, and age (p=0.0002), with ex-smokers significantly older than current or never smokers.
As shown in Table 2, age was significantly inversely associated with continuous KIF5A serum concentrations (rho=-0.11, p=0.0371), and with continuous KIF18A concentrations (rho=-0.29, p<0.0001), and significantly positively correlated with continuous p53 autoantibody concentrations (rho=0.38, p<0.0001), and with asbestos exposure years (rho=0.33, p<0.0001). KIF5A and KIF18A were not significantly correlated (p=0.1412), but both KIF5A (rho=-0.16, p=0.0028) and KIF18A (rho=-0.11, p=0.0313) were significantly inversely correlated with p53 autoantibody concentrations.
| |
Exposure |
Age |
KIF5A |
KIF18A |
p53AAbs |
| Exposure |
1 |
|
|
|
|
| 358 |
| Age |
0.3332 |
1 |
| <0.0001 |
|
| 354 |
358 |
| KIF5A |
0.3151 |
-0.1102 |
1 |
| <0.0001 |
0.0371 |
|
| 358 |
358 |
362 |
| KIF18A |
-0.2157 |
-0.2885 |
0.0775 |
1 |
| <0.0001 |
<0.0001 |
0.1412 |
|
| 358 |
358 |
362 |
362 |
| p53AAbs |
0.0870 |
0.3751 |
-0.1566 |
-0.1132 |
1 |
| 0.1003 |
<0.0001 |
0.0028 |
0.0313 |
|
| 358 |
358 |
362 |
362 |
362 |
Each cell presents Spearman's rho, p-value, and number of samples.
Table 2: Spearman’s Correlations of Exposure (years), Age, KIF5A, KIF18A, and p53 Autoantibodies.
The ROC analysis for p53 autoantibody expression confirmed that it was not significant as a predictor of exposure status (p=0.6052) and no cut point could be determined that adequately distinguished exposed from unexposed individuals (Figure 1).
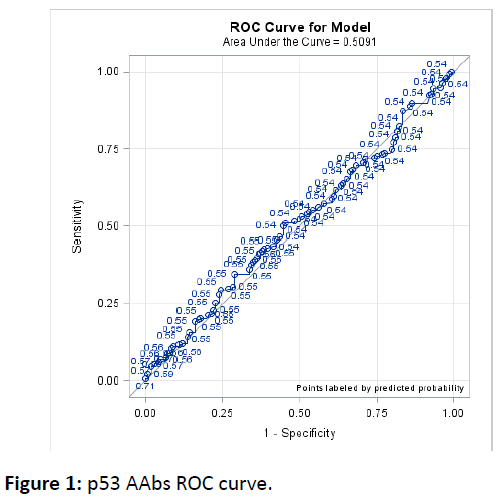
Figure 1: p53 AAbs ROC curve.
Both KIF5A and KIF18A were highly significant predictors of exposure status (p<0.0001) that performed reasonably well at distinguishing exposed from unexposed individuals as shown in Figures 2 and 3 and allowed determination of optimal cut points to distinguish exposed from unexposed individuals(Figure 2 and 3).
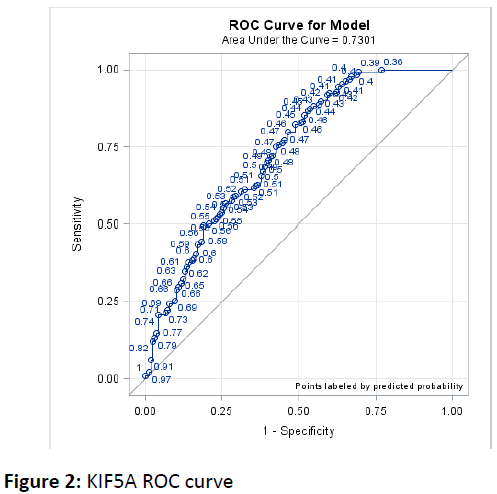
Figure 2: KIF5A ROC curve.
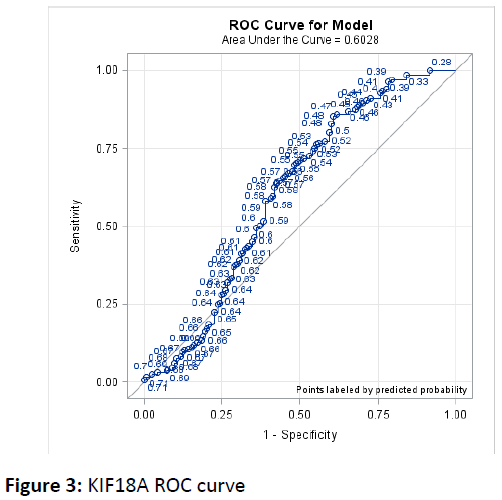
Figure 3: KIF18A ROC curve.
Based upon each cut point determined for the kinesin biomarkers from ROC analyses, individuals were classified as positive or negative for KIF5A and KIF18A, which then served as the outcome in multivariable logistic regression models. The optimal cut point using the Youden’s statistic method corresponded to 0.681 ng/mL for KIF5A and 526.399 ng/mL for KIF18A. The optimal cut point using the Euclidean distance method corresponded to 0.901 ng/mL for KIF5A and 361.436 ng/mL for KIF18A, demonstrating heterogeneity among methods of selecting the optimal cut point. Due to this heterogeneity both cut points were used in assessing the associations of these binary biomarkers to asbestos exposure in multivariable models.
In multivariable models assessing KIF5A positive status as defined by the Youden’s statistic cut point, only exposure status (positive/negative) and age were statistically significant, both at p<0.0001. Exposed individuals had 7.02 times the odds of positive KIF5A status compared to controls, while each additional year of age had 0.954 times the odds of positive KIF5A status (Table 3). In a model using continuous exposure instead of binary exposure status each additional year of exposure had 1.07 times the odds of positive KIF5A status. In multivariable models assessing KIF18A positive status as defined by the Youden’s statistic cut point, exposure status (positive/negative) (p=0.0003) and age (p<0.0001) and the interaction term for status and age (p=0.0016) were statistically significant. Exposed individuals had significantly lower odds of positive KIF18A status compared to controls at the 10th, 25th and 50th percentiles of the age distribution, while exposure status wasn’t significantly associated with KIF18a status at the 75th and 90th percentiles of age (Figure 4). Results using continuous exposure were similar with significantly lower odds of positive KIF18A status for each year of asbestos exposure at the 10th, 25th, and 50th percentiles of the age distribution and a non-significant association at the 75th and 90th percentiles of age. Multivariable modeling results were similar using biomarker status for KIF5A and KIF18A defined by the Euclidean distance method. Model fit was better for the Youden’s statistic method compared to the Euclidean distance method as measured by area under the curve for KIF5A (c=0.767 vs c=0.704) and about equal for KIF18A (c=0.747 vs c=0.746). For this reason the Youden’s statistic defined models were selected as the final models. In multivariable models assessing p53 autoantibody status (positive/negative) as defined by the assay protocol, neither exposure (p=0.89), ex-smoker status (p=0.30), current smoker (p=0.41) status, or age (p=0.13) were significant.
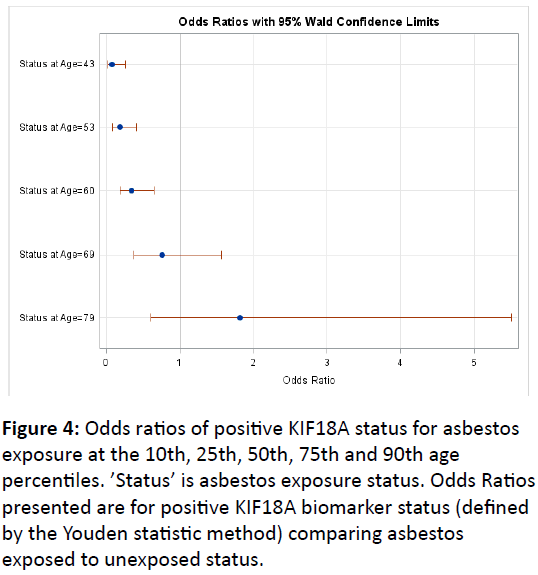
Figure 4: Odds ratios of positive KIF18A status for asbestos exposure at the 10th, 25th, 50th, 75th and 90th age percentiles. ’Status’ is asbestos exposure status. Odds Ratios presented are for positive KIF18A biomarker status (defined by the Youden statistic method) comparing asbestos exposed to unexposed status.
| Outcome: Exposure |
KIF5A |
KIF18A |
Age |
Current Smoker |
Former Smoker |
| beta-coefficient p-value OR (95% CI) |
beta-coefficient p-value OR (95% CI) |
beta-coefficient p-value OR (95% CI) |
beta-coefficient p-value OR 95% CI) |
beta-coefficient p-value OR (95% CI) |
| Model 1 |
0.5978 <0.0001 1.82 (1.43, 2.32) |
|
0.0376 <0.0001 1.04 (1.02, 1.06) |
-0.2692 0.405 0.76 (0.41, 1.44) |
0.2134 0.4431 1.24 (0.72, 2.14) |
| Model 2 |
|
-0.0265 <0.0001 * |
-0.1329 <0.0001 * |
-0.4656 0.1697 0.63 (0.32, 1.22) |
0.1601 0.5802 1.17 (0.67, 2.07) |
| Model 3 |
0.6234 <0.0001 1.87 (1.45, 2.39) |
-0.0283 <0.0001 * |
-0.131 <0.0001 * |
-0.4327 0.2249 0.65 (0.32, 1.31) |
0.1623 0.5956 1.18 (0.65, 2.14) |
| Model 4 |
2.2571 <0.0001 9.56 (5.12, 17.8) |
-1.242 <0.0001 0.29 (0.16, 0.53) |
0.0458 <0.0001 1.05 (1.03, 1.07) |
-0.2266 0.5085 0.8 (0.41, 1.56) |
0.303 0.3121 1.35 (0.75, 2.44) |
| |
Exposed Status |
Age |
Current Smoker |
Former Smoker |
|
| beta-coefficient p-value OR (95% CI) |
beta-coefficient p-value OR (95% CI) |
beta-coefficient p-value OR (95% CI) |
beta-coefficient p-value OR (95% CI) |
|
| Outcome: KIF5A |
1.9488 <0.0001 7.02 (3.98, 12.37) |
-0.0469 <0.0001 0.95 (0.94, 0.97) |
0.0019 0.9959 1.0 (0.48, 2.1) |
-0.3136 0.3279 0.73 (0.39, 1.37) |
|
| Outcome: KIF18A |
-6.2869 0.0003 $ |
0.0525 <0.0001 $ |
0.2484 0.4886 1.28 (0.64, 2.59) |
-0.2449 0.4627 0.78 (0.41, 1.51) |
|
Models 1-3 use continuous biomarkers; Model 4 uses dichotomous biomarkers defined by Youden's Index. KIF18A and Age had a significant interaction and therefore simple OR is not presented, Figure 5 presents ORs for KIF18A by various ages. $ Exposure and Age had a significant interaction (p=0.0016) and therefore simple OR is not presented, Figure 4 presents ORs for Asbestos Exposure by various ages. All Models (n=335) as 27 individuals with missing data were dropped.
Table 3: Final Regression Model Results for Associations of KIF5A, KIF18A, and Asbestos Exposure.
In multivariable logistic regression models of exposure status (positive/negative) including all three biomarkers (continuous) as well as the covariates of age and smoking only KIF5A, KIF18A, age, and the interaction term for KIF18A and age were significant (all p<0.0001) (Table 3). Individuals with 1 ng/mL higher KIF5A serum levels had 1.87 times the odds of asbestos exposure, while individuals with higher KIF18A serum levels had lower odds of asbestos exposure at younger ages, but there was non-significant association or increased odds of exposure at older ages (Figure 5). These findings were consistent with results from models examining KIF5A or KIF18A alone and with the associations from models of each biomarker as the outcome of interest.
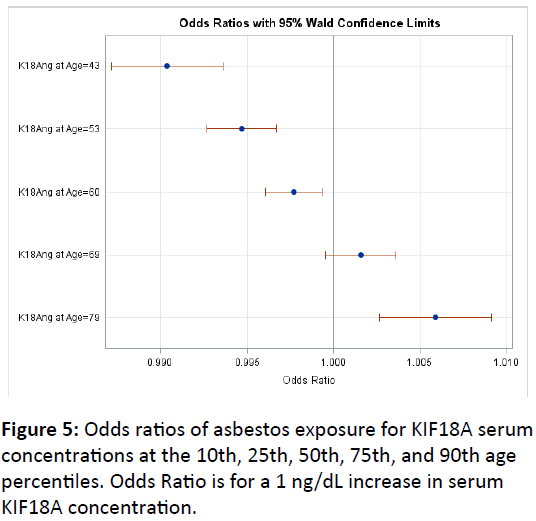
Figure 5: Odds ratios of asbestos exposure for KIF18A serum concentrations at the 10th, 25th, 50th, 75th, and 90th age percentiles. Odds Ratio is for a 1 ng/dL increase in serum KIF18A concentration.
Similar final models and significance levels were obtained utilizing dichotomous biomarkers as defined by either Youden’s statistic or the Euclidian distance method, however the Youden’s defined model achieved a better model fit by area under the curve comparison, (c=0.795) versus the Euclidean method (c=0.76) and therefore was selected as the final model method. Individuals who were positive for KIF5A had 9.56 times the odds of asbestos exposure, while those who were positive for KIF18A had 0.29 times the odds of asbestos exposure compared to those who were negative for each biomarker, and for each additional year of age individuals had 1.05 times the odds of asbestos exposure (Table 3). KIF5A positive status had a sensitivity of 85.35%, specificity of 47.56%, positive predictive value of 66.27%, and negative predictive value of 72.9% for asbestos exposure. KIF18A negative status had a sensitivity of 85.35%, specificity of 39.63%, positive predictive value of 69.15%, and negative predictive value of 63.06%.
Discussion
Previous studies have indicated that kinesin proteins are overexpressed in several types of cancers and involved in tumorigenesis and/or metastasis of breast cancer, renal cell carcinoma, nervous system tumors, lung tumors, retinoblastoma tumors, and cervical cancer, and thus might be useful targets for diagnosis and treatment [5,22-24]. KIF18A has been shown to be essential in the congression of chromosomes and the accurate alignment of the spindle equator and to suppress kinetochore movements during mitosis [25]. KIF18A overexpression has been positively related to tumor size and clinical tumor-node-metastasis in hepatocellular carcinoma (HCC), tumor grade and metastasis in breast cancer, and tumor stage, lymphatic invasion, lymph node metastasis, venous invasion, and peritoneal dissemination in colorectal cancer (CRC) as well as poor clinical outcomes [16-19].
In our present study we show that KIF18A serum concentrations are significantly decreased in asbestos-exposed individuals compared to unexposed controls, but that the relationship between KIF18A and asbestos exposure varies with age. The inverse association between KIF18A serum levels and asbestos exposure is greatest at lower ages in this cohort (40 to 60 years of age) and becomes non-significant by later ages (69+). Lung is one of the few normal tissue types where KIF18A is detectable and this decrease in its serum concentration in asbestos-exposed individuals may signal an early disruption of its expression and function in the lung tissue. Interestingly the association was strongest in younger aged individuals and not significant in older individuals, which may indicate differences in physiologic responses to potential respiratory insult/damage or an already present adaptive response in older individuals. While less is known about the role of KIF5A and its potential relationship to disease, our present study has shown significantly increased serum concentrations of KIF5A in asbestos-exposed individuals compared to unexposed controls. This increase in serum KIF5A concentrations may signal an increase in cell activity and/or cell turnover as an early response to asbestos exposure. Both of these changes in KIF18A and KIF5A serum concentrations may be related to early changes that precede development of disease as increased KIF5A concentrations and decreased KIF18A concentrations were found to distinguish asbestos cancer patients from non-cancer controls in a subset of occupationally exposed Finnish asbestosis patients [20].
We additionally found that serum p53 autoantibody concentration was not related to asbestos exposure in this cohort of Italian workers. This finding is in contrast to the borderline significant association between p53 autoantibodies and cumulative asbestos found in a cohort of Finnish asbestosis patients [10]. p53 autoantibodies were also not significantly associated with smoking status, which was also found in the cohort of Finnish asbestosis patients [10]. Given the well-established relationship between p53 mutations and p53 autoantibodies and numerous cancers including asbestosrelated cancers, our finding of an absence of a relationship to asbestos exposure may indicate that p53 mutations and subsequent autoantibody formation occur nearer to the development of malignant changes and overt disease.
Strengths of this study include the investigation of two new potential biomarkers of asbestos exposure and potentially early effect in the disease process as well as an examination of the potential relationship between p53 autoantibodies and asbestos exposure in a new cohort including occupationally exposed workers with a relatively long average cumulative exposure to asbestos. We were additionally able to examine the potential impact of smoking upon these relationships. Our analyses found consistent magnitude and strength of associations for KIF5A, a potential inverse association of KIF18A, and lack of association for p53 autoantibodies with asbestos exposure utilizing different approaches, lending further confidence to our findings. This research does however have several limitations including highly variable data on smoking that necessitated use of current/ex/never classifications, limited data on actual asbestos exposures consisting only of years of presumed exposure, and only one blood measurement used to quantify representative biomarker levels for each individual. Additionally, while the control group did contain a number of other blue collar and white collar workers it was largely composed of healthcare workers who may have differed from asbestos workers on other unmeasured confounders such as diet, exercise, and other lifestyle factors, and exposure to other occupational or environmental pollutants with health risks.
Conclusion
The results from this study suggest that KIF5A, and possibly KIF18A, could serve as useful biomarkers of asbestos exposure and may signal early changes in cellular functioning that could precede the development of asbestos related disease. While the findings for KIF5A were consistent, the potentially varying association observed for KIF18A and asbestos exposure by age may limit its utility as a reliable biomarker. More research is needed to clarify the potential relationships of these proteins to asbestos exposure to determine if the associations found in this population of occupationally exposed individuals are consistent in other occupationally exposed populations as well as possibly in individuals who would only be environmentally exposed to asbestos. Additional studies could also help to clarify the optimal cut point of each kinesin for the molecule to serve as a useful tool for screening. Studies should also be conducted to assess a potential relationship of these molecules to the development of asbestos related disease. This would help to broaden the understanding of the potential role of these kinesins in response to asbestos exposure as potential markers of early effect.
Acknowledgements
This work was supported in part by grants from NIOSH (R01- OH07590 and R21-OH010311).
References
- WHO (2014) Asbestos: elimination of asbestos-related diseases (Fact sheet 343).
- IARC (2012) Asbestos (Chrysotile, Amosite, Crocidolite, Tremolite, Actinolite, and Anthophyllite). IARC monographs on the evaluation of carcinogenic risks to humans. Lyon: IARC, 100C: 219-310.
- ATSDR (2001) Toxicological profile for asbestos. Atlanta: US DHHS.
- WHO (2006) Elimination of asbestos related diseases. WHO/SDE/OEH/06.03. Geneva: World Health Organization.
- Yu Y, Feng YM (2010) The role of kinesin family proteins in tumorigenesis and progression: potential biomarkers and molecular targets for cancer therapy. Cancer 116: 5150-5160.
- Liu X, Gong H, Huang K (2013) Oncogenic role of kinesin proteins and targeting kinesin therapy. Cancer Sci 104: 651-656.
- Mazumdar M, Lee JH, Sengupta K, Ried T, Rane S, et al. (2006) Tumor formation via loss of a molecular motor protein. Curr Biol 16: 1559-1564.
- Castillo A, Morse III HC, Godfrey VL, Naeem R, Justice MJ (2007) Overexpression of Eg5 causes genomic instability and tumor formation in mice. Cancer Res 67:10138-10147.
- Hofseth L, Hussain SP, Harris CC (2004) p53: 25 years after its discovery. Trends Pharmacol Sci 25:177-181.
- Li Y, Karjalainen A, Koskinen H, Hemminki K, Vainio H, et al. (2005) p53 autoantibodies predict subsequent development of cancer. Int J Cancer 114: 157-160.
- Mattioni M, Chinzari P, Soddu S, Strigari L, Cilenti V, et al. (2013) Serum p53 antibody detection in patients with impaired lung function. BMC Cancer 13: 62.
- Mattioni M, Soddu S, Prodosmo A, Visca P, Conti S, et al. (2015) Prognostic role of serum p53 antibodies in lung cancer. BMC Cancer 15: 148.
- Cordes C, Von Lingen J, Gorogh T, Ambrosch P, Gottschlich S, et al. (2009) Molecular and immunological aspects of p53 and p53-autoantibodies in head and neck squamous cell carcinoma. Oncol Reports 22: 1299-1303.
- Anderson KS, Wong J, Vitonis A, Crum CP, Sluss PM, et al. (2010) p53 autoantibodies as potential detection and prognostic biomarkers in serous ovarian cancer. Cancer Epidemiol Biomarkers Prev 19: 859-868.
- Suppiah A, Greenman J (2013). Clinical utility of anti-p53 auto-antibody: systematic review and focus on colorectal cancer. World J Gastroenterol 19: 4651-4670.
- Shichijo S, Ito M, Azuma K, Komatsu N, Maeda Y, et al. (2005) A unique gene having homology with the kinesin family member 18A encodes a tumour-associated antigen recognised by cytotoxic T lymphocytes from HLA-A2þ colon cancer patients. Eur J Cancer 41: 1323-1330.
- Liao W, Huang G, Liao Y, Yang J, Chen Q, et al. (2014) High KIF18A expression correlates with unfavorable prognosis in primary hepatocellular carcinoma. Oncotarget 5: 10271-10279.
- Zhang C, Zhu C, Chen H, Li L, Guo L, et al. (2010) Kif18A is involved in human breast carcinogenesis. Carcinogenesis 31: 1676-1684.
- Nagahara M, Nishida N, Iwatsuki M, Ishimaru S, Mimori K, et al. (2011). Kinesin 18A expression: clinical relevance to colorectal cancer progression. Int J Cancer 129: 2543-2552.
- Tooker BC, Newman LS, Bowler RP, Karjalainen A, Oksa P, et al. (2011) Proteomic detection of cancer in asbestosis patients using SELDI-TOF discovered serum protein biomarkers. Biomarkers 16: 181-191.
- Youden WJ (1950) Index for rating diagnostic tests. Cancer 3: 32-35.
- Chandrasekaran G, Tatrai P, Gergely F (2015) Hitting the brakes: targeting microtubule motors in cancer. Br J Cancer 113: 693-698.
- Kasahara M, Nagahara M, Nakagawa T, Ishikawa T, Sato T, et al (2016) Clinicopathological relevance of kinesis family member 18A expression in invasive breast cancer. Oncol Lett 12: 1909-1914.
- Myers SM, Collins I (2016) Recent findings and future directions for interpolar mitotic kinesin inhibitors in cancer therapy. Future Med Chem 8: 463-489.
- Stumpff J, Von Dassow G, Wagenbach M, Asbury C, Wordeman L (2008) The kinesin-8 motor, Kif18A, suppresses kinetochore movements to control mitotic chromosome alignment. Dev Cell 14: 252-262.

